
The Sustainable Development Goal (SDG) 3.1 target aims to reduce maternal mortality ratio (MMR) to less than 70 per 100,000 live births globally.1 The most recent MMR estimates show that 223 maternal deaths per 100,000 live births occurred in 2020, with considerable disparities among countries; the sub-Saharan African (SSA) region accounted for 70% of maternal deaths worldwide.2 These high levels highlight the gap in reaching the target by 2030. The World Health Organization (WHO) promotes antenatal care (ANC) as a package of health interventions women receive during pregnancy.3 It presents an important opportunity for the prevention, diagnosis, and treatment of conditions that could threaten the health of the woman and unborn baby, as well as for providing information on nutrition, danger signs, family planning, and birth preparedness.4,5 Thus, good quality ANC for pregnant women is an important component of health services aiming to improve maternal and perinatal health.
WHO recommended focused antenatal care in 2001, with four ANC visits during pregnancy for women with uncomplicated pregnancies; more otherwise.6 The four visits in this model are scheduled; the first visit is between 8 to 12 weeks after conception, and the three other visits should occur between 24 and 38 weeks of gestation. In 2016, a new standard model of at least eight ANC contacts was recommended by WHO on the basis of improved perinatal outcomes and women’s preferences.7 Worldwide, countries differ in the speed and manner of implementation of this doubled number of the minimum recommended ANC visits from four to eight. The coverage with four or more ANC visits, a key indicator of ANC utilisation, increased in most SSA countries in the past decades.8 However, a number of studies which explored how the recommended components of ANC contacts are adhered to found that increasing the number of ANC visits does not always translate into better content or higher quality of ANC.9–11 It is important to understand whether and how a higher number of ANC visits influences the quality of ANC in order to inform the implementation of this new eight-visit model.
Burundi is a landlocked country with nearly 13 million inhabitants, 87% of which live in rural areas.12 The total fertility rate is estimated at 5.1.13 Burundi made impressive progress in improving maternal health, but maternal and neonatal mortality rates remain high. According to WHO, MMR reduced from 874 to 594 deaths per 100,000 live births between 2000 and 2020, an annual rate of reduction of 2.9%.2 However, there is a threat of stagnation due to low use of key maternal health services; 49% of pregnant women received four or more ANC visits, and 47% initiated the first ANC visit in the first trimester.13 A positive achievement is a reduction in home births over the past decade (84% births occur in health facilities; 85% are assisted by a skilled health personnel). However, this has not translated into a commensurate reduction in maternal mortality ratio toward reaching the SDG by the end of 2030.
The Burundi health policy is currently aligned with the previous model of focused antenatal care (minimum of four ANC visits). The 2019 Plan Stratégique National de la Santé de la Reproduction, Maternelle, Néonatale, Infantile et des Adolescents aims to improve utilization and quality of ANC services. Specifically, it aims to increase the percentage of health facilities offering high-quality ANC services from 62% in 2019 to 80% in 2023. It targets the quality of several interventions, such as intermittent preventive treatment for malaria, two or more doses of tetanus and diphtheria vaccination, and HIV testing.14 It is therefore critical to understand whether increasing the number of contacts women have with the health system during pregnancy can support such health policy targeting improvements in the content and quality of ANC. Our understanding of the content and quality of ANC in Burundi is limited. Jiwani et al analysed the timing and number of ANC contacts in low- and middle-income countries, including Burundi, and found a positive association between timely ANC initiation (first visit in the first trimester of pregnancy) and the number and content of ANC.15 In addition, several studies focused on the coverage of four or more ANC visits during pregnancy and its determinants. In contrast, another study of the quality of ANC and associated factors in East Africa excluded Burundi because the data for Burundi did not contain all of the six ANC components used by the study to capture the quality of ANC.16–18
The objective of this study was to estimate the percentage of pregnant women who used the recommended number of ANC visits and routine components of ANC using the Burundi Demographic and Health Survey 2016/2017. Second, we examine the association between number of ANC visits and number of ANC components received.
METHODS
Study design and data source
This is a cross-sectional study using data from the most recent Burundi Demographic and Health Survey (DHS) 2016/2017. The Burundi DHS is a national representative household survey using a stratified two-stage sampling design. To design the frame, each of the 18 provinces in Burundi was stratified into rural and urban strata. At the first stage, a total of 554 primary sounding units were drawn from the list of enumeration areas according to the general population and housing census carried out in 2008. A number of households in each of these clusters provided a list of households from which a sample of 30 households per cluster was drawn, both in urban and rural areas. Then, 3,180 households in 106 clusters and 13,440 households in 448 clusters were selected respectively in urban and rural areas. All women age 15–49 who were usual members of the selected households or who had slept in the households the night before the survey were eligible for interviews. About 99 % of eligible women were interviewed.
For data processing, android-based computer tablets programmed using a mobile version of CSPro were used. The CSPro software was developed jointly by the U.S. Census Bureau, Serpro S.A., and The DHS Program. A follow-up of the data collection was regular at the office and field level. The Work was assigned by supervisors and shared via Bluetooth to interviewers’ tablets. At the end of each day, the supervisors did initial data checks and edits and then submitted data to the central servers via internet. At this level, data were checked again in order to detect any errors, which were communicated back to the field teams for correction. Data were checked lastly in the central office to resolve any errors that were not corrected by field teams during data collection.
Detailed information about sampling, data collection methodology and data analysis is available elsewhere.13
Among women who were interviewed, information about ANC use and components of ANC received was collected for the most recent pregnancy, which resulted in a live birth in the 5-year recall period of the survey.
Population
We included all women aged 15-49 years who had a live birth in the two years preceding the survey to maximise the accuracy of recall of ANC use. ANC for the pregnancy leading to this period’s most recent live birth was analysed.
Definitions
Women were asked how many ANC visits they received during pregnancy. We considered women who reported at least one facility-based ANC visit to be ANC users. Among ANC users, those who reported receiving at least four visits were considered as having had adequate ANC. Coverage of adequate ANC was defined as the percentage of all pregnant women in the sample who received 4 or more ANC visits. Next, we examined the content of ANC based on ANC users’ responses to questions about various components of ANC. Eight components were captured on the survey and used in this analysis:
-
iron tablets or syrup taken at least one day during pregnancy,
-
drugs for intestinal parasites taken,
-
blood pressure having been taken at least once during pregnancy,
-
urine sample taken at least once during pregnancy,
-
blood sample taken at least once during pregnancy,
-
intermittent preventive treatment for malaria (sulfadoxine-pyrimethamine [SP]/Fansidar) at least one dose during pregnancy,
-
tetanus protection (defined as women who received two injections during pregnancy or who were protected before the index pregnancy [have already received 2 or more injections and the last within 3 years before birth or 3 or more injections the last within 5 years before birth or 4 or more the last within 10 years before birth or 5 injections or more before birth]), and
-
HIV testing services received in the context of ANC.13
For each component, if the woman responded yes (component received), the value assigned was 1; otherwise (did not receive or response do not know/missing), the value was zero. For HIV testing services, value 1 was assigned if the response to all following questions was yes: talked about HIV transmitted from mother-to-child, talked about things to do to prevent getting HIV, talked about getting tested for HIV, tested for HIV as part of ANC visit, obtained HIV test result as part of ANC.
Among users of ANC, we examined the receipt of each of the eight components separately, as the number of components received (continuous variable range 0-8) and as a complete package (received all eight components = 1, received fewer than eight =0).
Covariates
Demographic, obstetric, and socioeconomic characteristics were considered as covariates. They were selected considering their availability on the DHS and relevance for the utilisation of ANC services as shown in published literature19–21. Anderson’s behavioral model for healthcare use was adapted to select explanatory variables; several studies have used this model to investigate the determinants of the ANC services utilization.19,20 The variables include: woman’s age group in years (15-24, 25-34, 35+) at the time of survey; woman’s education level (no education, primary, secondary or higher); marital status at time of survey (married, living with a partner, other [never in union, divorced, widowed or separated]); household wealth quintile as constructed by the DHS program; religion (Catholic, Protestant or other); residence (rural, urban); region (Bujumbura mairie, Southern [Makamba, Rutana, Bururi, Rumonge], Western [Cibitoke, Bujumbura rural, Bubanza], Northern [Ngozi, Kayanza, Kirundo, Muyinga], Eastern [Ruyigi, Cankuzo, Karuzi], Centre [Gitega, Muramvya, Mwaro]; woman’s exposure to mass media (yes if exposure at least once a week to one of the media: radio, magazine or internet; otherwise no); woman’s healthcare decision-making about the woman’s own health (alone or with partner, partner alone or someone else); woman’s perceived distance to health facility (big problem, to a big problem); woman covered by a health insurance (yes, no); parity at index pregnancy (first, second, third, fourth or more); and wantedness of index pregnancy (wanted then, later, wanted no more).
Analysis
Description of the study population was done using frequencies and percentages with 95% confidence intervals (CI). We calculated the percentage of women attending at least one ANC visit and the percentage of ANC users attending 4+ visits. Then, we estimated the percentage of all ANC users and all users of 4+ ANC visits who received each component of ANC and the whole package of eight components. In bivariate analysis, we examined the association between the number of ANC components (continuous variable from zero to eight) and each category of the selected variables. The statistical significance was tested by a chi-square (svyschisq) test for the categorical dependent variable and analysis of variance (ANOVA) for the numerical dependent variable (mean of number of the component). A p-value <0.05 was considered statistically significant. Second, we fitted a series of bivariate linear models, including the primary exposure (number of ANC visits as a continuous variable from zero to ten) to identify potential confounders. Finally, multivariable statistical analyses using a generalized linear model (GLM) approach were carried out to estimate the association between the number of ANC visits and the number of ANC components received when adjusted for confounding. This explanatory model included only variables that changed the regression coefficient by more than 10% or showed a significant association with the mean number of ANC components. Since the interest outcome and the primary exposure are continuous variables, Poisson regression model might have been appropriate.21 However, using Poisson regression assumes that the mean of the distribution is equal to the variance, which may always not correct; variance can either be larger (over dispersion) or smaller (under dispersion) than the mean. The violation of equidispersion produces invalid inferences when using Poisson regression and negative binomial regression may be recommended in that case.22 The key variables ─ number of ANC visits and the number of ANC component─ were over dispersed. Thus, we used negative binomial regression model for the regression coefficients estimates. Due to the complex survey design used in the DHS, adjustments for sampling using weights, strata and clustering were applied in all analyses.23 All statistical analyses were conducted using R package version 4.2.2.24
RESULTS
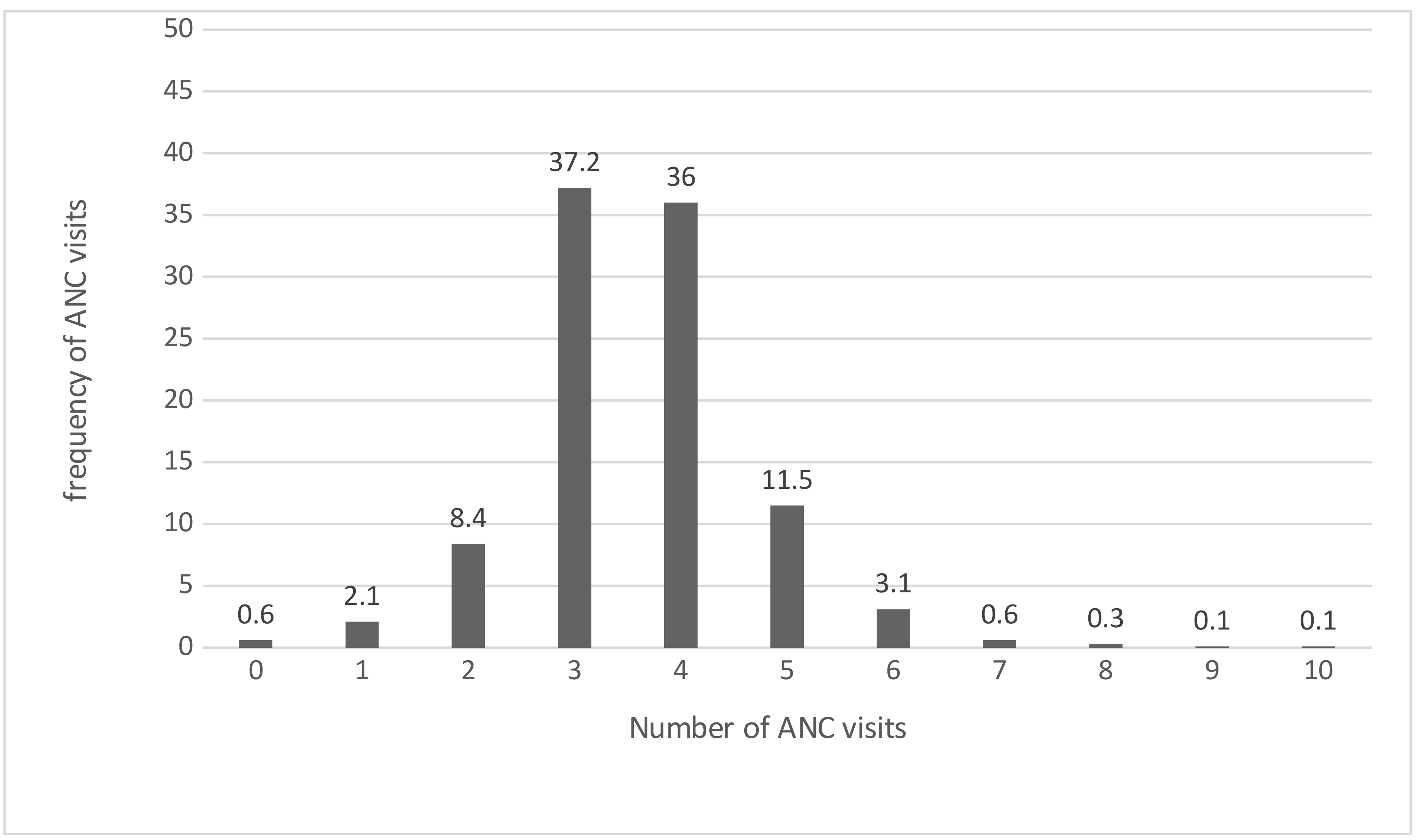
Table 1 presents the demographic, obstetric and socioeconomic characteristics of the 5,261 women who had a live birth in the two years preceding the survey. Half of the study sample were 25-34 years old; 43.7 % and 44.3 % received no formal education and attained primary school, respectively. The majority of women lived in rural areas (91.0%), and about a third in the Northern (31.0%) region. Approximately 64.2% wanted the last pregnancy at the time, and for 17%, it was their first birth. Women with four or more previous pregnancies represented about half of the sample (48.2%). Nearly all women (99.4%, 95% CI=99.2-99.6) reported receiving some ANC. The distribution of number of ANC visits among ANC users (n=5,227) is shown in Figure 1. The maximum reported number of visits was ten, and the median number of visits was 3.6. Half of ANC users (51.7%, CI 95%=49.8-53.6) reported receiving an adequate number of visits (four or more).
.png)
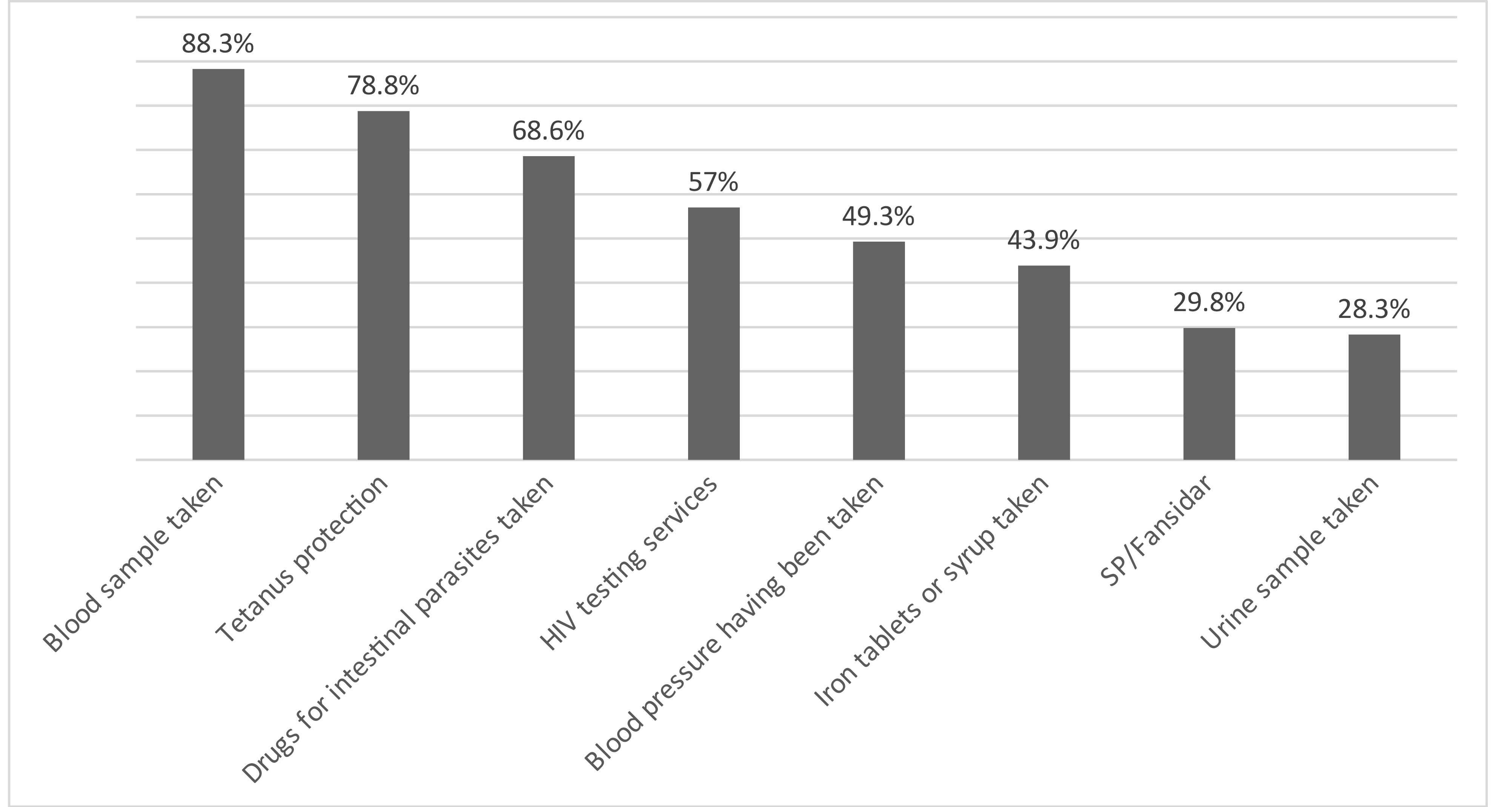
Among ANC users (n=5,227), we examined the percentage who reported receiving each of the eight measured ANC components. Blood sample taken was the most commonly reported component (88.3%), followed by tetanus protection (78.8%). Urine sample taken was the least received component (28.3%) (Figure 2). Online Supplementary Document, Table S1 shows the percentage of ANC users and adequate ANC users who received each component of care. A bivariate analysis of the receipt of each ANC component among ANC users is shown in the Online Supplementary Document, Table S2. The component with the least variability across demographic, obstetric and socioeconomic categories was having had a blood sample taken. Geographic region was the covariate with the highest difference in receipt of ANC components, with significant variation across regions found for all eight components.
.png)
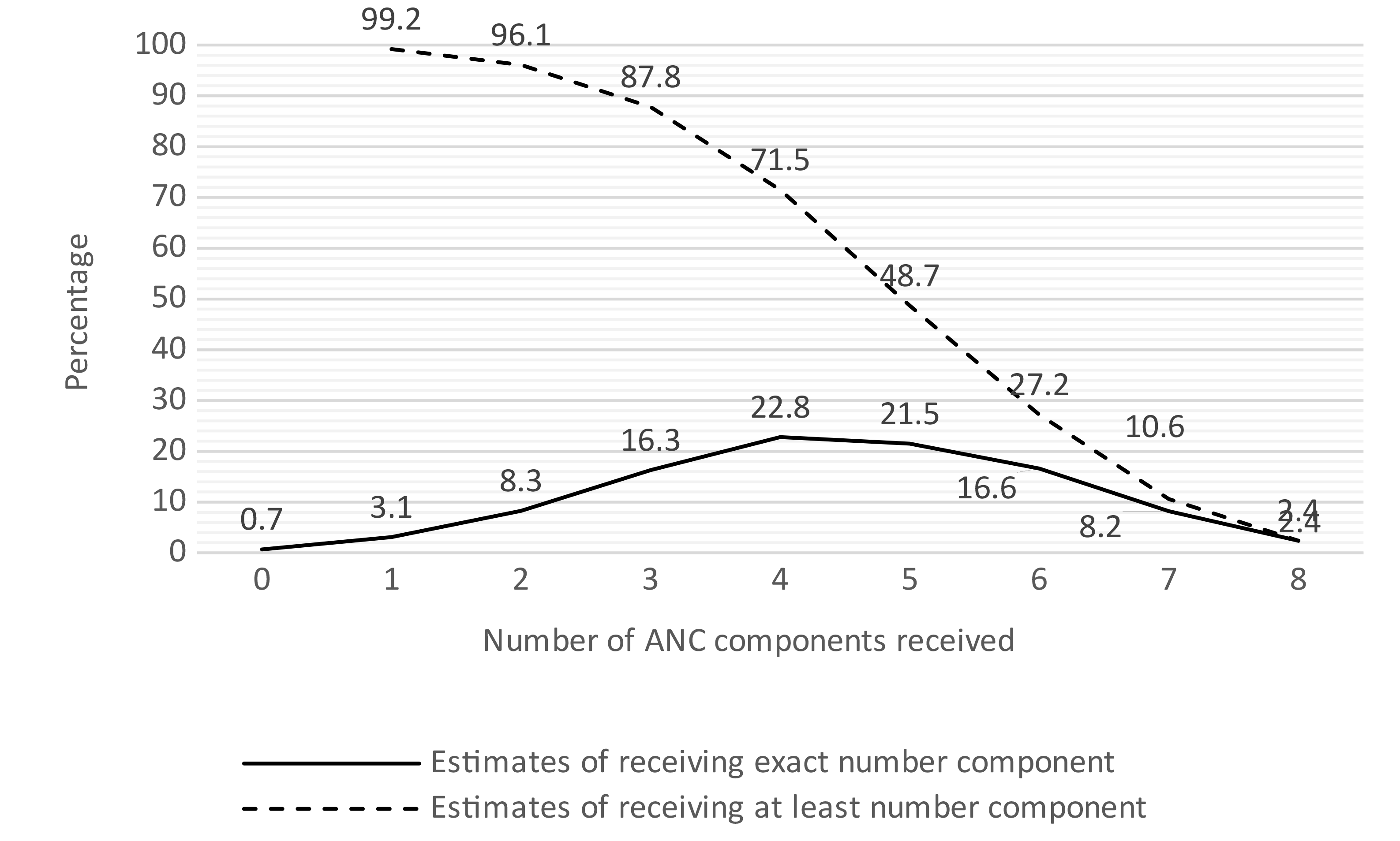
The total number of components received by ANC users ranged from zero to eight, with a mean of 4.44 (CI 95%=4.37-4.51). Less than 1% of ANC users did not receive any care component, and 2.4% (95% CI=1.9-3.0) reported receiving all eight components (Figure 3). Among adequate ANC users (n= 2,726), the mean number of components received was 4.63 (CI 95%=4.55-4.72), with 3.4% receiving all eight components.
.png)
Bivariate analysis assessing the association between the number of ANC visits and the receipt of each individual ANC component showed that women’s reports of blood pressure having been measured and iron tablets or syrup taken were not significantly associated with the number of ANC visits (p>0.05), Figure 4. The probability of receiving the other six components increased with an increasing number of ANC visits.

Determinants of the number of components of ANC received
The result of ANOVA test examining variation among the number of components received by selected covariates is in Table 2. The number of ANC components received was significantly associated with women’s age group, education level, marital status, household wealth quintile, religion, region and residence. The number of ANC components received was positively associated with the number of ANC visits (p<0.001), rising from a mean of 3.53 among ANC users with one visit to 5.50 among those with 10 visits. Table 3 shows the results of the linear regression of factors associated with the number of ANC components received among ANC users. The number of ANC visits was significantly associated with the increasing number of components received in both bivariate (regression coefficient= 0.23; 95% CI=0.18–0.28; p<0.001) and multivariable (adjusted regression coefficient= 0.21; 95% CI= 0.16–0.25; p<0.001) models. Other variables significantly associated with the number of ANC components received were region, education, household wealth, religion, residence, coverage by health insurance, and parity.
DISCUSSION
This study examined key clinical interventions offered during ANC and investigated whether, in Burundi, a higher number of ANC visits is associated with the number of ANC components received. The coverage with any ANC among pregnant women in Burundi was more than 99%. However, only half of them received an adequate number of visits (four or more). These findings indicate that the very high utilisation of ANC did not translate into high continuity of care. Existing literature points to some factors that affect the number of ANC visits, including income, residence, education, parity and quality of the health system.25–27 Another factor known to influence the number of ANC visits is early ANC initiation (in the first trimester). According to the study from Tanzania, this can contribute to 51% of the changes in the number of adequate ANC visits.25 The quality of ANC is among the strongest drivers of retention in maternal care.28 Our findings indicate that this low continuity of care might be at least partly related to the low quality of ANC.
When looking at components of ANC reported by women as a proxy for quality of care, we found that a blood sample taken was the most commonly performed ANC component (9 in 10 ANC users). This was inconsistent with findings from other SSA countries, which reported that blood pressure measurement was the component with the highest coverage.11,29 The respondents were asked whether the blood sample had been taken once for their most recent pregnancy. However, there were no other questions to know the nature of the test done using that sample blood, hence possibly reflecting a commitment to HIV testing. On the other hand, blood pressure, which should be measured on multiple occasions during ANC, showed a relatively low coverage among ANC users (49%). The method using a cuff around the arm and a device that inflates the cuff is commonly used in Burundian health facilities. We suggest further research to understand the reasons for the lack of blood pressure monitoring among pregnant women, including the availability and functionality of equipment and training of health workers. Urine tests are a key intervention for pregnant women because they can detect early health problems such as diabetes, urinary tract infections and preeclampsia.30 However, urine tests were the least performed ANC component in our study, which might be due to a lack of guideline implementation, availability of consumables, and functional laboratories in health facilities in Burundi.
A key finding of this study was the high variation in the receipt of ANC components across regions within the country; this was found for all eight components. According to a study from Nigeria, the geographic location of residence influences receipt of ANC services.31 Blood samples taken and HIV testing services received were the components with the least variability across demographic, obstetric and socioeconomic factors, possibly due to these interventions being universally routinely implemented by the vertical HIV program. A qualitative study is needed to understand the accessibility, availability, and acceptability of each ANC component in the Burundian context. Considering ANC components as a package, we found that less than 5% of ANC users received all eight ANC components. This is consistent with the findings of a study from Ethiopia (3.3%) and an analysis of data from 20 countries in SSA (5%) which explored also the ANC components.32,33 However, almost all ANC users reported having received at least one care component; this suggests that the high utilisation of care by women is not matched by high quality of services. We suggest further investigation of the quality of maternal health care and its impact on the continuum of care during pregnancy in the context of Burundi.
We also assessed the association between the number of ANC visits and each ANC component received and found that iron supplementation and blood pressure being measured were not significantly associated with the number of ANC visits. In effect, this means that despite multiple opportunities (ANC visits), the effective coverage of these key ANC interventions remained low. The number of ANC visits should increase the likelihood of receiving ANC components, particularly those which should be given at multiple visits. For instance, according to WHO recommendations, blood pressure measurement is an essential component of ANC to be taken at each visit 7. We suggest further research to understand why more ANC visits are not associated with higher chances of blood pressure measurement and iron tablets or syrup consumption among ANC users in Burundi. It is possible that women receive ANC in the same health facilities during pregnancy and some of these health facilities are not providing some of the ANC components to women during any ANC visit. Additionally, it is also possible that some of the less invasive components of ANC might not be easily remembered by women; especially if women do not receive an explanation or test results. Lastly, studying ANC components as a package, we found that an increase in the number of ANC visits was significantly associated with the receipt of a higher number of ANC components. Every additional ANC visit was associated with an increase of 0.21 of an ANC component in multivariable analysis, which is consistent with several studies from other SSA countries.29,34
Strengths and limitations of the study
This study used nationally representative household survey data with a large sample size. We included births in the two years preceding the survey to reduce recall bias. The survey was conducted in 2016/2017, and all information on the use of ANC and components received were self-reported by women, potentially leading to some social desirability bias. In addition, due to the survey skip pattern, women who had a miscarriage or stillbirth were not included in the sample. These factors together could cause that our results of the already low percentage of ANC users who received ANC components might be slightly overestimated. In addition, we could not assess the receipt of some key ANC components such as nutrition, danger signs of pregnancy, or family planning-related information because these were not captured in the survey. We also had no information about whether the follow-up actions to the tests and measurements captured among the ANC components were timely, evidence-based, and of high quality. Last, it is possible that some residual confounding remained in the multivariable model, for example by sector of ANC facility or individual women’s health condition).
CONCLUSIONS
Our findings show a near-universal coverage of ANC among pregnant women, with a steep drop to half when we look at an adequate number of ANC visits (four or more). In addition, we found suboptimal receipt of key ANC components, even among women accessing ANC the recommended number of times. The number of ANC visits was found to be significantly associated with the receipt of six of the eight components investigated, and an increasing number of ANC visits was associated with a higher number of ANC components reported. For measuring and evaluating the provision of ANC in Burundi, programmers and policymakers could be guided by the simple indicator assessed in this study, such as the percentage of the ANC users who received all recommended ANC components. In addition, rigorous mixed-methods research is needed to understand barriers and facilitators for achieving a high retention rate in the continuum of ANC and improving the quality of ANC in line with the national guidelines.
Acknowledgements
We thank the women who participated in the Demographic and Health Survey 2016–2017.
Authorship contributions
NC was involved in the conceptualization, design, data analysis and preparation of the draft of the manuscript. LB contributed to the idea research, the study design, results interpretation and then finalised manuscript. TS provided a contribution to the statistical analysis.
Disclosure of interest
The authors declare that they have no competing interests.
Additional material
This is included as Online Supplementary Document.
Correspondence to:
Nshimirimana Clement.
Department of public health, Institute of Tropical Medicine, Antwerpen, Belgium
E-mail: [email protected]