Intimate partner violence (IPV) is defined as ‘physical violence, sexual violence, stalking and psychological aggression (including coercive tactics) by a current or former intimate partner (i.e., spouse, boyfriend/girlfriend, dating partner, or ongoing sexual partner).’1 The IPV epidemic in Canada disproportionately affects indigenous people and is shaped by the enduring impacts of settler colonisation, which is defined as ‘a distinct type of colonialism that functions through the replacement of Indigenous populations with an invasive settler society that, over time, develops a distinctive identity and sovereignty.’1
In 2021, police-reported IPV increased for the seventh successive year across Canada with 344 victims per 100,000 population, which represented a 2% increase from 2020).2 The prevalence of lifetime IPV is significantly higher among indigenous women (61%) and men (54%) than among their non-indigenous counterparts in the general population (44% and 34%, respectively).3 Further, IPV rates are up to 10 times higher in the Northwest Territories (NWT) of Canada—which comprise a majority of the indigenous population — compared to the rest of the country.4 This pervasive violence is largely attributable to settler colonialism, which forcefully eroded traditional indigenous values, identities and systems, replacing them with insidious systems of hetero-patriarchy that value domination over shared power and agency.5 Moreover, settler colonial mechanisms of genocide, displacement, oppression, and assimilation prompted a shift from traditional indigenous practices and complementary gender roles towards the dehumanising attitudes and adversarial gender roles that produce IPV.6,7
Youth are particularly at high-risk for IPV due to the challenges they face navigating adolescence and young adulthood, during which they are likely negotiating intimacy and boundary setting within relationships for the first time.8 In Canada, women (29%) and men (26%) aged 15-24 are over twice as likely to experience recent IPV than the general population (12% and 11%, respectively).3 Despite youth and Indigenous communities being disproportionately prone to IPV, there is a lack of evidence that disaggregates data by ethnicity to demonstrate the prevalence and determinants of IPV among Indigenous youth in northern Canada. Obtaining such data would inform context-specific and youth-tailored interventions to address IPV among Indigenous youth.
Violence victim service providers in the NWT propose that the best approach to reduce IPV is addressing the social environment within which such violence resides.9 Culture-based programming has the potential to redress the social dynamics that sustain IPV in Indigenous communities. Culture-based programmes include interventions that encourage traditional Indigenous beliefs and practices such as connectedness to the land, dance, drumming, poetry, storytelling, crafts, and elder-youth interactions.10–12 A recent Canadian study examined the impact of an artistic, trauma-informed cultural intervention on Indigenous women who survived IPV; the intervention—which did not focus on violence but rather promoted self-care, peer support and Indigenous cultural teachings— improved mental health, resilience, post-traumatic growth, and connectedness to land, community, and nature among Indigenous survivors of violence.13
A narrative review of 104 peer-reviewed publications and intervention research expert opinions by Crooks et al. highlighted a dearth of evidence-based strategies for preventing IPV among Indigenous youth in North America.14 The authors critique many programmes for Indigenous youth as they reflect non-Indigenous perspectives by focusing on individual-level characteristics rather than strengths-based, community-oriented values of connectedness, relational well-being and healing.14 For this reason, Indigenous-led violence prevention programmes tend not to measure violence explicitly; instead, they evaluate the efficacy of violence prevention interventions by focusing on empowerment-related outcomes.13 Measuring IPV among youth participating in strengths- and culture-based programmes could provide crucial evidence to fill the knowledge gap around IPV and potential violence prevention strategies among Northern Indigenous youth. We report findings from a study that aimed to determine the prevalence, correlates and trends of violence over a four-year period among youth participating in a land- and arts-based programme in the NWT.
METHODS
Study design, procedures and population
This community-based, serial cross-sectional study used baseline data from a peer-led, land- and arts-based programme designed by Indigenous Northerners to promote empowerment, resilience, sexual health, cultural connectedness and overall well-being of youth in 18 NWT communities.15 Youths aged 12 to 19 were recruited into the study using venue-based sampling through peer networks, community partners and social media platforms. The study period was between 2018 and 2021; two or three summer retreats were held each year. Since participants could attend multiple retreats, each annual retreat cohort contained a mixture of new and returning participants. Facilitators included sexual and gender-diverse Indigenous cultural leaders/Elders, sexual health educators and staff peers. Indigenous Elders in Canada play a vital role in preventing violence and substance use, and promoting mental health and sexual and reproductive health by transmitting values of tolerance, respect, empathy, sense of belonging and pride to their communities.16 Youths completed paper-and-pen, self-administered surveys under the supervision of a researcher. Participants received sweaters as a token of appreciation for their time.
Ethics
The Aurora Research Institute (license number: 15741) and the University of Toronto Research Ethics Board (protocol number: 31602) provided ethical approval for this study. All participants provided voluntary, written informed consent prior to completing the self-administered survey. Indigenous researchers administered consent forms to all study participants.
Survey Measures
Dependent variables
The two study outcomes were the prevalence of experienced and perpetrated IPV in the 12 months before the retreat. Researchers surveyed participants to evaluate whether they experienced or perpetrated IPV using the 20-item Revised Conflict Tactics Scale.17 Researchers revised the original terminology for violence categories as follows: (1) ‘verbal violence’ represents ‘negotiation’ and ‘psychological aggression’; (2) ‘physical violence’ represents ‘physical aggression’ and ‘injury from assault’; and (3) ‘sexual violence’ represents ‘sexual coercion’. The IPV outcomes were composite variables of verbal, physical and sexual violence.
In accordance with the Conflict Tactics Scale scoring guidelines, respondents were classified as experiencing or perpetrating IPV if they answered affirmatively to one or more questions related to experiencing or perpetrating verbal, physical or sexual violence. Responses to questions on verbal, physical and sexual violence were grouped to form two dichotomous outcome variables: (1) experienced IPV and (2) perpetrated IPV. These variables were coded ‘yes’ for participants who experienced or perpetrated violence and ‘no’ for participants who never experienced or perpetrated any form of intimate partner violence.
Independent variables
Independent variables were grouped into three broad categories: sociodemographic characteristics, sexual health, and mental health. The sociodemographic characteristics included age, gender, sexual orientation, ethnicity, and the number of prior land- and arts-based programmes attended. Sexual health-related variables included knowledge of HIV, condom use, and safer sex self-efficacy. HIV knowledge was assessed using the HIV knowledge questionnaire consisting of 18 true or false questions scored on a scale of 0 to 1818; condom use self-efficacy19 and safer sex self-efficacy20 were assessed using five-point Likert scales, with higher scores indicating greater self-efficacy. Mental health was measured using validated scales for depression and post-traumatic stress disorder (PTSD). Depression was assessed using the two-item Patient Health Questionnaire, which uses a scale of 0 to 6, where a score of 3 or greater indicates major depressive disorder.21 PTSD was assessed using the trauma screening questionnaire, which consists of 10 yes or no questions that measure responses to traumatic events; responding positively to six or more questions indicates a high risk of having PTSD.22
Statistical analysis
Descriptive statistics were performed to generate frequency distributions and measures of central tendency and dispersion. We summarised categorical variables using frequencies and percentages and summarised continuous variables using means and standard deviations (SD). Trends in the prevalence of IPV from retreats spanning 2018 to 2021 were tested using the Mann-Kendall test, with a significance level of p<0.05. We used logistic regression to test whether there was a gendered difference in IPV trends between participants. We used chi-squared tests of association for categorical variables and t-tests for continuous variables to examine statistically significant differences in our independent variables stratified by our outcomes (experiencing or perpetrating IPV). We conducted bivariate logistic regression to determine the independent variables associated with experiencing or perpetrating IPV and included significant variables at p<0.05 in our final multivariable model, which also adjusted for age and ethnicity. We then ran post-estimation commands to check the model specification and fit. Stata 17 software (Stata Corp, College Station TX, USA) was used to perform all statistical analyses.
RESULTS
Our analysis included 240 youth participants. The mean age of respondents was 14.5 years (standard deviation=1.3). Sixty per cent of participants (n=144) were female, 36% (n=87) were male, and 4% (n=9) were non-binary (Table 1). Over two-thirds of participants were Indigenous (n=167, 70%), while the remaining third belonged to different ethnic groups (n=73, 30%) (Table 1).
Table 2 displays the prevalence of experiencing and perpetrating any form of IPV among participants throughout the study. Sixty-two percent of participants (n=112) experienced IPV; the prevalence of experiencing IPV was higher among female participants (n=73, 66%) than male participants (n=34, 54%). Over half of adolescents (n=99, 55%) perpetrated any form of violence against their intimate partner; female participants reported a higher prevalence of perpetrating IPV (n=66, 60%) than male participants (n=30, 48%).
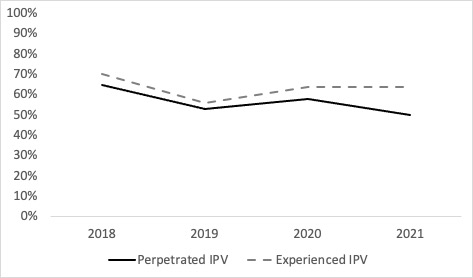
Figure 1 shows the trends of experiencing and perpetrating IPV from 2018 to 2021. The prevalence of experiencing IPV decreased by 6% between 2018 and 2021, whereas the prevalence of perpetrating IPV decreased by 14% between 2018 and 2021. However, neither trend was statistically significant (P>0.05). Gender-based analysis did not reveal any significant difference in trends of either type of IPV between male, female and non-binary participants.
_(n_180).png)
In bivariate analysis, participants with higher scores for depression and PTSD were more likely to experience and perpetrate IPV than participants with lower scores (Table 3). Depression was the only factor that remained significantly associated with experiencing and perpetrating IPV in well-specified multivariable models with a good fit. Specifically, for every one-unit increase in depression severity score, participants were 30% more likely to experience IPV (adjusted odds ratio, AOR: 1.30, 95% CI: 1.05, 1.61) and 24% more likely to perpetrate IPV (AOR: 1.24, 95% CI: 1.01, 1.52) (Table 4).
DISCUSSION
We found a high prevalence of experiencing (62%) and perpetrating (55%) IPV among youth in the NWT. Our findings add to the limited literature on the prevalence of IPV among youth in Northern Canada. The experience of IPV among youth in our study is higher than reported among women (66% versus 29%) and men (54% versus 26%) aged 15-24 in Canada.3 This discrepancy between Northern youth and youth across Canada highlights the need for youth-friendly and context-specific violence prevention programmes for youth in Northern Canada. We stress that before such programmes are implemented, efforts should first be made to engage Indigenous and Northern youth and other key community stakeholders such as Elders and traditional leaders to understand their desires for appropriate programming.23,24 Such an approach would ensure that statistics do not simply guide programmes but also the voices of Indigenous and Northern youth and the wisdom of their communities.
There was a declining trend of IPV over the four years of our study, but the trend was not statistically significant. This finding indicates persistently high levels of IPV in the NWT. Although the land- and arts-based peer-led programming has effectively improved individual-level characteristics such as youth empowerment and leadership skills,12 multi-level approaches are required to address the climate of sustained IPV we observed. Among Indigenous and Northern youth in the NWT, social interventions to address violence could use community-based participatory methods to involve youth in decision-making and dissemination of findings to ensure the translation of research into policy and social change.25 Further, it is vital for future programmes in mostly Indigenous settings, such as the NWT, to note that the inclusion of youth goes beyond incorporating youth voices in programmes. True inclusion must recognise the historical context of colonisation and its impacts on youth agency while accounting for various social dynamics, including Elder/youth and Indigenous/non-Indigenous power relations.26
Both perpetrating and receiving IPV were associated with a higher likelihood of depression among youth in our study, which suggests a syndemic between mental health and IPV that will need to be explored in longitudinal studies to determine directionality. The correlation between highly prevalent IPV and symptoms of depression among youth in our study is consistent with the evidence of mental health hospitalisations that are almost five times higher among youths aged 15-17 in the NWT than among the general Canadian population (23.3 per 1000 people versus 4.7).27 Interventions addressing IPV among youth in the NWT must, therefore, also consider addressing the wider determinants of mental health, which—as shown by our programme previously—include food insecurity, gender inequity and intergenerational exposure to trauma.28,29 We echo the sentiments of other scholars that Indigenous mental health cannot be addressed with a one-size-fits-all approach but rather using upstream, community-engaged efforts and adapting evidence-based approaches in similar contexts.30 An example of a successful mental wellness initiative that could be adapted for youth in our study is the Access Open Minds initiative implemented for and with Inuit youth in the NWT; this initiative redesigned mental wellness services for Inuit youth by using community mapping to identify service gaps, incorporating Inuit approaches to wellness, and strengthening linkages to conventional mental health care.31
This study had certain limitations. Firstly, IPV experience and perpetration were self-reported for the previous 12 months, subjecting them to social desirability and recall bias. Despite these biases, the Revised Conflict Tactics Scale we used to measure IPV prevalence has shown good reliability among US-based youth who experienced (Cronbach = 0.59) and perpetrated (Cronbach = 0.67) IPV.32 Secondly, our study sample was heavily weighted in favour of female retreat attendees, which may have introduced selection bias. Lastly, although our analysis satisfied the minimum requirement of having four data points to perform the Mann-Kendall trend test,33 our four-time points (2018-2021) may have been insufficient to detect a true trend.
CONCLUSIONS
Despite its limitations, our study adds to the limited evidence base around IPV among youth in the NWT. Northern youths participating in our study had a higher prevalence of IPV than the general population in Canada, with inconclusive evidence of a decline in violence over four years. Moreover, both perpetrating and experiencing IPV were associated with a higher likelihood of depression. We believe these findings could inform future violence and mental health programming efforts among youth in the NWT. Our findings call for qualitative studies to delve deeper into the context-specific dynamics that sustain IPV among Northern youth. We also recommend that future programmes be grounded in decoloniality and social justice. This will involve recognising and addressing the influence of colonisation and its ongoing effects on the health and well-being of Indigenous youth in the NWT and dismantling standardised practices for delivering health programming to incorporate locally-driven and culturally relevant interventions. Finally, we call for studies to evaluate the impact of the above programmes on reducing IPV and improving the mental health and well-being of Northern youth.
Acknowledgements
We thank the youth who participated in this study for sharing their time and experiences.
Funding
This work was supported by the Arctic Inspiration Prize, the Public Health Agency of Canada (1718-HQ-000617 and 1617- HQ-000033), Canada Institutes of Health Research, the Social Sciences and Humanities Research Council of Canada and the Government of the Northwest Territories.
Authorship contributions
Conceptualisation was conducted by KM, ZA, CHL and LG; analysis was led by ZA and KM; writing was done by KM and ZA; review & revision was performed by KM, ZA, CHL, CLL, AK, SBT, KIM, CM and LG.
Disclosure of interest
The authors completed the ICMJE Disclosure of Interest Form (available upon request from the corresponding author) and disclose no relevant interests.
Correspondence to:
Kalonde Malama
Factor-Inwentash Faculty of Social Work
University of Toronto
Toronto, ON, Canada
[email protected]