
Advances in neonatal care have led to a shift in the global focus from “essential newborn care” to the care of “small and sick neonates” especially after WHO recognized prematurity and low birth weight (LBW; defined as birth weight of less than 2500 grams) as the leading causes of under-5 mortality and a major contributing factor to the overall burden of childhood handicap in both developed as well as developing countries.1
LBW babies are at increased risk of morbidities such as temperature instability, feeding problems, sepsis, hypoglycemia, neonatal jaundice, and apnea, and thereby need specialized care in addition to that provided to babies with normal weight in postnatal wards. However, all LBW babies do not fall under the “small and sick” neonates requiring intensive care in neonatal units.2
Most (80%-85%) of them are “small but stable”. LBW neonates are born beyond 32 weeks gestation as moderate to late preterm or intrauterine growth-restricted full-term babies. They need extra feeding and temperature maintenance support and may not need intensive care. Most of these infants can survive with adequate supportive care without requiring admission to the neonatal units. However, under current guidelines, these small babies are admitted to the NICU despite being clinically stable across the globe. It results in needless separation from mothers during the critical bonding period and hampers the establishment of exclusive breastfeeding. These neonates are managed in a similar way to sick infants or those with sepsis, exposing them to interventions and infectious hazards. This is besides the fact that neonatal units are already overburdened, and have to function with scant resources alongside inadequate staff allocation.3
The zero Separation concept was introduced by Bergman and it means one parent will be present all the time with neonates. Zero separation is an important part of family-centered care as per the Swedish National Board of Health and Welfare. As per the Global Alliance for Newborn Care, zero separation is a family-centered approach to newborn care where the newborns should be accompanied by their mothers/parents, regardless of whether or not they have health problems.4 The ‘Zero Separation Policy’, if feasible, is likely to benefit both the mother and her baby. It will not only prevent exposure of the baby to potentially hazardous NICU environments but will also relieve the mother’s anxiety and help her bond early with her baby. Maternal separation is a source of toxic stress for infants admitted to the NICU. It affects the hormonal milieu and alters the development of neural and autonomic systems, negatively impacting mental and physical health in the long term. Increased mother-infant interaction can shorten the duration of hospital stay and promote early initiation of breastfeeding and Kangaroo mother care (KMC) with better weight gain and long-term neurodevelopmental outcomes.
As India strives towards achieving the Sustainable Development Goal target of reducing preventable neonatal deaths to at least 12 per 1000 live births by 2030,5 and with an increasing number of institutional deliveries, there is a need to develop cost-effective strategies to decongest the neonatal units, deliver accessible and quality newborn care to the ones in need. This can be achieved by early rooming-in of small and stable LBW babies with their mothers under the supervision of doctors and nurses without admission to the neonatal unit.
Recent evidence from developed and developing countries suggests that mothers can be easily trained in healthy neonatal care practices including feeding, skin-to-skin care, and identifying danger signs. The presence of a mother with her baby, right from the time of birth, strengthens her confidence, prepares her for discharge, and helps in reducing post-discharge mortality and morbidity in the long run.6
Therefore, this study was conducted to assess the feasibility of a zero-separation policy among clinically stable neonates weighing 1500-2000 grams at birth, in terms of ‘complications requiring admission to neonatal unit’ or ‘successful discharge home’ among babies cared for in the same room with their mothers in the mother-baby unit.
Methods
This study was done at a tertiary care hospital equipped with a level III NICU in a low-and middle-income country (LMIC) over 36 months from January 2017 to December 2019. Ethical approval was obtained from The “Ethics Committee for Human Research”, Lady Hardinge Medical College, New Delhi. LBW neonates weighing 1500-2000 grams delivered via vaginal birth and clinically stable at birth were shifted with their mothers to a 12-bed “Mother Baby Unit (MBU)” within 6 hours. ‘Clinical stability’ was defined as a baby being hemodynamically stable (normal color, oxygenation, and perfusion with capillary refill time <3 seconds), along with the absence of hypothermia or any respiratory distress requiring respiratory support (Temperature 36.5˚C-37.5˚C, RR<60/min, no retractions/grunt or cyanosis). Neonates with major congenital malformations, gestation age less than 32 weeks (either by date or the timing of the ultrasound scan for the 1st trimester), or requiring resuscitation beyond 30 seconds of positive pressure ventilation were directly admitted to the neonatal unit irrespective of their birth weight. Infants whose mothers could not be moved to the MBU within 5-6 hours of delivery due to maternal issues like uncontrolled hypertension/diabetes, PPH, or severe anemia were also excluded.
“Mother Baby Unit” is a twelve-bed area, designated in the typical postnatal ward, with round-the-clock availability of nurses (at least 3 in the morning and 2 in other shifts) trained in essential newborn care, care of low birth babies, including temperature maintenance and lactation management, and provision of basic obstetric and postpartum care to the mother. Comfortable chairs for providing Kangaroo mother care (KMC) were made available in addition to the other postnatal ward facilities, including sufficient space for maternal beds and toilet and bathing facilities for mothers. The resident doctors from the Department of Obstetrics and Neonatology examined the mother and the baby respectively.
Case management
All babies were monitored and managed as per standard operating protocols. Mothers were counseled regarding breastfeeding, KMC, maintenance of general hygiene, including hand washing, and detection of danger signs. Vital parameters (heart rate, respiratory rate, temperature, oxygen saturation, capillary refill time, peripheral pulses) and overall activity were recorded at the time of admission and then every 6 hours for the initial 72 hours of life and every 12-24 hours after that until discharge. Mothers provided KMC on the reclining chairs provided in the MBU, and the duration of skin-to-skin contact (in hours) was recorded. In addition, the frequency and mode (direct breastfeeding or assisted feeding via cup spoon or oro-gastric tube) of feeding, along with the type of milk consumed (MOM, Preterm formula milk), cumulative duration of KMC, daily weight, and any morbidity such as hypothermia, hypoglycemia, feed intolerance, jaundice, signs of sepsis, seizures, and apnea were noted daily.7
Hypothermia was defined as axillary temperature less than 36.5 and was graded as cold stress (36-36.4 degrees Celsius), moderate hypothermia (32-35.9 degrees Celsius), and severe Hypothermia (<32 degrees Celsius).6 Babies with cold stress were placed on immediate skin-to-skin contact with their mothers, followed by regular checks of temperature every 30 minutes. Immediate transfer to the neonatal intensive care unit (NICU) for monitoring and further management was instituted for babies with moderate to severe hypothermia and those who continued to remain hypothermic even after 60 minutes of skin-to-skin contact with the mother.
Dextrose monitoring was performed in all these babies at 2, 6, 12, 24, and 48 hours of life and 72 hours of life for cases where breastfeeding was not well established. Hypoglycemia was defined as blood glucose less than 45 mg%, measured by the heel prick method using a Glucometer and point-of-care reagent strips.7 All babies with hypoglycemia, irrespective of symptoms, were shifted to the NICU and managed as per standard NICU protocols. A trial of oral feeds with the mother’s own milk (MOM) or formula was given to babies with asymptomatic hypoglycemia, provided the blood glucose levels were between 25-45 mg/dl.8 Babies with symptomatic hypoglycemia or asymptomatic hypoglycemia with blood glucose levels less than 25 mg/dl or those who continued to remain hypoglycemic even after feeding (checked after 1 hour of feeding) were started on glucose infusion rate (GIR) at 6mg/kg/min.9,10
All babies were examined for the presence of jaundice every 8-12 hours during the initial 3-5 days of life, and serum bilirubin levels were estimated for those with significant jaundice on clinical examination and/or by transcutaneous bilirubin meter. The need for treatment in the form of phototherapy or exchange transfusion was decided as per the American Academy of Pediatrics (AAP) criteria in babies with gestation age ≥ 35 weeks and according to the National Institute of Health & Care Excellence (NICE) guidelines in babies < 35 weeks.11,12 Hyperbilirubinemia requiring phototherapy was managed at the bedside in the MBU itself, and babies requiring exchange transfusion or those with serum bilirubin levels nearing the exchange transfusion range despite 12-24 hours of phototherapy were transferred to the neonatal unit.
Infants who developed morbidities in the form of feed intolerance, clinical signs of sepsis, seizures, and apnea were also shifted to the NICU for further management.13 Discharge home criteria included regaining birth weight or weight gain of at least 10 grams/kg/day for at least 3 consecutive days, exclusive breastfeeding, mother about caring for the baby, and absence of any morbidity. Mothers were instructed to seek health care post-discharge if danger signs were observed. The need for readmission after discharge was established by enquiring about it during follow-up visits and/or telephonic follow-ups within 2 weeks of discharge.14
Outcome measures
The primary outcome was the proportion of neonates at MBU requiring transfer to NICU for further management. Secondary outcomes include the incidence of morbidities like hypothermia, hypoglycemia, feed intolerance, jaundice, sepsis, seizures, and apnea, mortality during the hospital stay, and the need for readmission after discharge.
Statistical analysis
Data analysis was performed using IBM Statistical Package for Social Sciences (SPSS version 23) for MS Windows. Descriptive statistics were used to report discrete variables expressed as percentages and proportions, continuous variables were presented as mean with standard deviation and median with interquartile ranges.
Results
Out of 39465 vaginal deliveries during the study period of 36 months (January '2017 to December 2019), 1736 (4.4%) neonates had birth weights between 1500-2000 grams. Of these, seventy-two percent of infants (n=1247) were unstable or sick, requiring admission to the neonatal unit (63%), or had maternal complications preventing early rooming in (9%). A total of 489 stable neonates (28%), were moved to MBU with their mothers making up the cohort for this study.
The mean birth weight of enrolled babies was 1738 ± 102 grams with a median gestation of 34 weeks (ranging from 32-41 weeks). The baseline characteristics of the mother-baby dyad are given in Table 1.
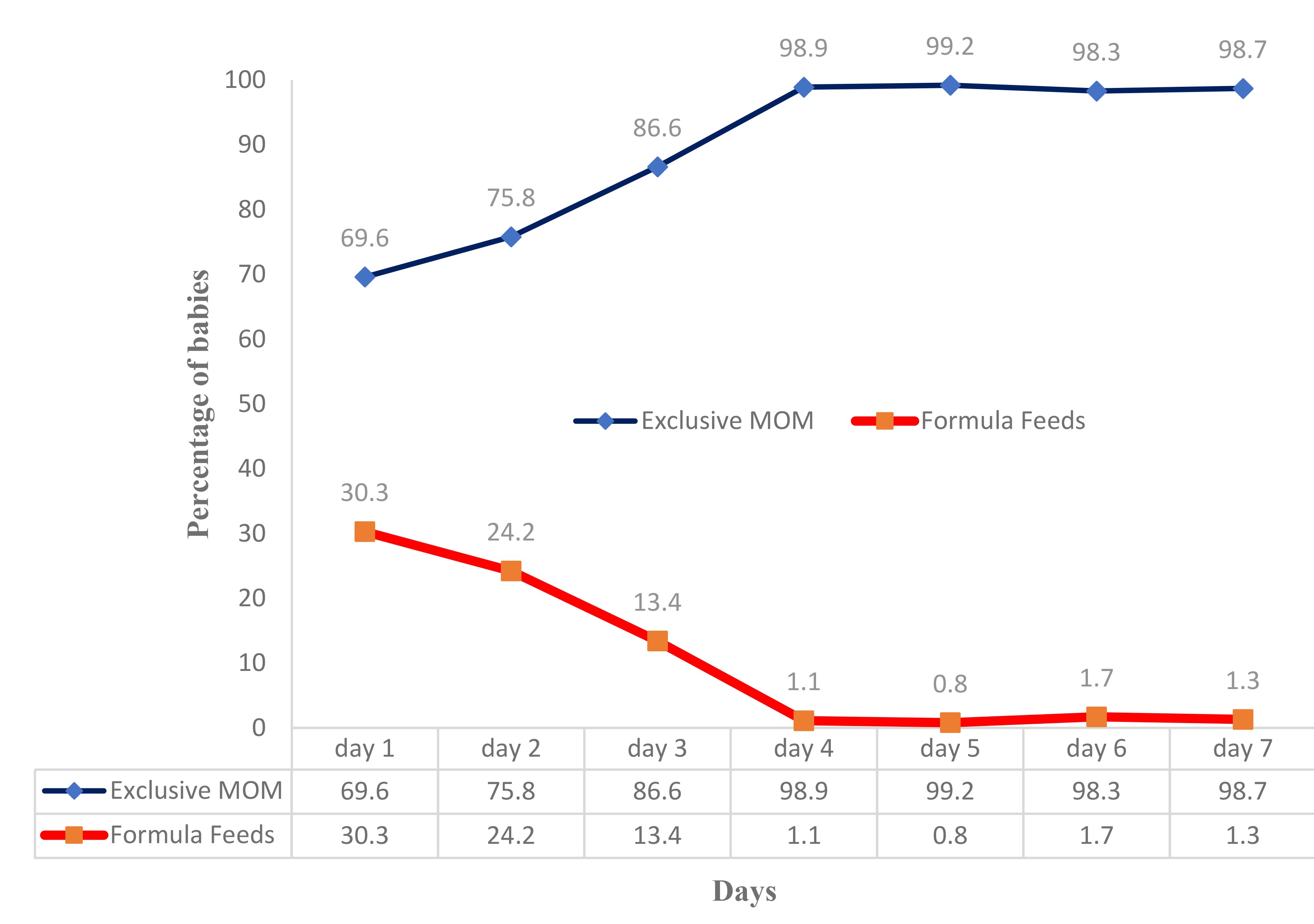
Feeding: Most mothers fed their babies 10 -12 times a day. Seventy percent of infants exclusively received their mother’s own milk (MOM) on day 1, which increased to more than 95% from day 4 onwards (Figure 1). Similarly, three-fifths of mothers started direct breastfeeding within the first 24 hours after birth, and the rest received assisted feeding using a spoon or paladai. From day 2 to 5, direct breastfeeding rates increased to 71%, 83%, 95% & nearly 100%, respectively.
.png)
Skin-to-skin care: Two-thirds of mothers provided KMC for at least 5-8 hours on day 1, increasing to 85% by day 5 (Figure 2). The median duration of Skin-to-Skin care was 6 hours/ day (IQR 5-6 hours/day).
.png)
Primary outcome
Thirty-nine babies (8%) required transfer to NICU for management. (Table 2)
Secondary outcomes
Neonatal hyperbilirubinemia requiring treatment (phototherapy) was the most common morbidity (28.8%), most of which was managed at the bedside in the MBU (Table 3). No baby had hypothermia, apnea, FI, seizures, or hemodynamic instability.
All neonates were successfully discharged home (Table 2). However, eight babies needed re-hospitalization for jaundice. , The median duration of hospital stay was 6 days (IQR 5-8 days).
Discussion
Increasing awareness and focus on newborn health have changed the focus from essential newborn care to care of small and sick newborns in developing countries. The postnatal wards do not have round-the-clock availability of trained pediatricians and nursing staff to monitor illness signs in small neonates leading to overburdened neonatal intensive care units.15 This prospective cohort study evaluated the outcome of clinically stable, LBW babies weighing 1500-2000 grams at birth who were in the same room to allow for mother and baby to be together in the MBU following ZSP. The present study aimed to determine the proportion of stable LBW babies (1500-2000 g) who could be roomed in with their mothers after birth and could be successfully discharged home. The mean birth weight and gestational age of the babies’ enrolled were 1738.32±101.8gm and 34.59 ±1.69 weeks, respectively. In the present study, approximately 31% of babies were SGA which is higher in comparison to the incidence of SGA babies in the world, which ranges from 2.5% to 10%. As per an Indian study by Kushwaha et al, the incidence of SGA babies was reported as 28.4%.16 In the present study, these SGA babies were successfully managed in MBU with little additional support in terms of feeding and monitoring. This population of SGA babies is unique in the context of our country, and the management of this population in MBU highlights the importance of lactation counseling and temperature management.
In this study, 4.7% of neonates required NICU admission due to hypoglycemia, and most of them developed hypoglycemia in the first 24 hours. It is a well-established fact that LBW and SGA babies are more prone to hypoglycemia, more so the SGA infants.17 In the current study, too, most hypoglycemic babies were SGA which again highlights the importance of strict monitoring for hypoglycemia in the initial 72 hours in this population.
Two-thirds of babies received KMC on day 1, which increased to 85% from day 5 onwards. Kangaroo mother care (KMC) is a special method of care for LBW infants more specifically below 2000 gm. It consists of skin-to-skin contact, exclusive breastfeeding, and early discharge with an adequate follow-up. A Cochrane review on early skin-to-skin contact (SSC) for healthy newborns and their mother’s reports that SSC improves physiological regulation, increases breastfeeding and KMC rates, and lowers mortality.18 Research in the past few decades has made it clear that KMC may be an alternative to incubator care for stable LBW infants. However, despite the known advantages of KMC in LBW infants, it is still not widely practiced in LBW infants in India. An open-labeled randomized control trial from southern India included 140 stable VLBW infants and these were then randomized into two groups, the KMC group and the Conventional medical care (CMC) group. The babies who were in the CMC group received the conventional incubator/warmer care while the babies in the KMC group were shifted to the KMC ward located near the NICU. There was no difference in weight gain from randomization to hospital discharge between the Kangaroo care group and the conventional care group. Mortality and morbidities and duration of hospitalization were equally distributed between the two groups. This study established that KMC is as effective as conventional care of stable VLBW infants in the NICU.19
Recently in a multicentric trial conducted in LMICs, immediate kangaroo mother care (I-KMC) has shown a reduction in neonatal mortality among babies weighing 1000 grams to 1799 grams. A special 12-bed M-NICU was established to provide I-KMC in sick neonates, and mothers were counseled and trained to provide KMC to neonates.5 Establishing a special M-NICU requires extra resources for budgetary allocation for additional manpower, and infrastructure, while the MBU can be established easily in postnatal wards with existing resources. The same manpower (working staff nurses and doctors) can train mothers to provide KMC after birth and monitor the babies for complications of the early neonatal period. The only extra requirement in terms of resources is comfortable KMC chairs for mothers to provide KMC to stable LBW neonates.
In this study, 95% of these small and stable babies received breastmilk by day 4 of life, and babies were discharged on exclusive breastfeeding, which highlights the importance of zero separation at birth. The birth of a child is a stressful experience for the mother, and separating the baby from the mother for any reason escalates her distress. Bonacquisti and colleagues reported that lack of privacy, provision of a structured feeding schedule, exhaustion, and anxiety were the factors that affected maternal breast milk supply adversely during the neonate’s NICU stay. Additionally, factors likely to provide lactation support and direct breastfeeding were shown to improve satisfaction among mothers.20
In the present study, 92% of enrolled babies were discharged without admission to the neonatal unit, with zero mortality. Neonatal hyperbilirubinemia was the most common morbidity that developed in these babies, and it was managed with phototherapy in the same MBU, by keeping the baby by the mother’s side. Eight percent (8%) of the babies required NICU admission due to hypoglycemia, significant jaundice, and sepsis. After discharge, 1.6% of babies required readmission for jaundice and ultimately got discharged from the NICU. As per available literature, the primary reasons for early readmission in moderate and late preterm infants are jaundice and feeding difficulties with a readmission rate of around 3% to 4%. In the present study, the main reason for readmission was jaundice and the readmission rate was quite low which again highlights the importance of zero separation in this population.21
The possible implications of the present study are that LBW babies can be segregated into two main groups – small & stable neonates and small & sick neonates. Both groups of babies are being admitted to the neonatal units for management, but the current study has shown that it is feasible to manage small and stable LBW neonates in MBU with some extra monitoring and lactation support. It will reduce the workload of the already inadequate neonatal staff and will lead to better allocation of resources for small and sick neonates.
This study evaluated a new concept of zero separation amongst mother-baby dyads of small and stable neonates which seems feasible. A similar policy/practice was implemented with obstetric and neonatal teams and it permitted the promotion of best practices for the mothers and their babies. While this is a preliminary study, evaluating the feasibility and studying a few outcomes, a multicentric study to evaluate the feasibility on a larger scale to incorporate this new concept of LBW care is warranted. The global community needs effective utilization of available limited resources in LMICs to achieve 'sustainable development goals".
Acknowledgements
The authors are grateful to the residents and nursing staff working in the MBU and are thankful to all the mothers and infants who participated in this study.
Ethics approval
The ethical approval for the study was obtained from the Ethics Committee of Human Research Lady Hardinge Medical College, New Delhi, India LHMC/EHCR/2016/156.
Informed consent to participate
Informed consent was obtained from the legal guardian of all included participants.
Funding
None
Availability of data and material
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Authorship contributions
SN conceptualized and designed the study with data collection instruments. RA, SS, and GK collected data. SG coordinated and supervised data collection and conducted the statistical analysis. SG and RA drafted the initial manuscript. BD and SN provided intellectual inputs and critically reviewed and revised the manuscript. All authors approved the final version of the manuscript submitted to the journal for peer review and agreed to be accountable for all aspects of the work.
Disclosure of interest
The authors completed the ICMJE Disclosure of Interest Form (available upon request from the corresponding author) and disclosed no relevant interests.
Correspondence to:
Prof Sushma Nangia, DM
Director-Professor and head
Department of Neonatology
Lady Hardinge Medical College and associated Kalawati Saran Children’s Hospital, New Delhi, India, 110001
Email – [email protected], Contact no.- +919810838181.