
Diabetes mellitus (DM) is a disorder of metabolism in which an absolute or relative deficiency of insulin results in hyperglycaemia leading to acute and chronic complications.1 DM is a disease that relies on many factors and may vary over time and region, it is said to be chronic when there is the presence of high blood sugar, which results from imperfection in insulin action, insulin secretion or both.2 It is a heterogeneous group of carbohydrate, fat and protein metabolism disorders characterized by chronic hyperglycaemia, degenerative vascular changes and neuropathy. It tends to accelerate degenerative changes throughout the body by widespread vascular changes in the large blood vessels and the microvessels.3
There are a number of factors reported in literature that can cause diabetes in individuals.4 These factors include but are not limited to lifestyle, urbanization, unhealthy dietary habits, family history, cigarette smoking, old age, growing consumption of cheap processed food, genes, and viruses. Physical inactivity and overweight or obesity, which causes insulin resistance, may result in Type 2 diabetes, while Type 1 diabetes occurs when the individual body immune system fights the insulin to produce a beta cell of the pancreas.5
Globally, there has been a reported increase in the number of DM cases in recent times, especially in the world’s low- and middle-income countries where socio-economic conditions are poor, and the life expectancy is low due to poor living standards and ill-health conditions of the inhabitants. Global statistics revealed that there are about 422 million people have diabetes cases worldwide, with most of these people from underdeveloped and developing nations. Annual global deaths attributed to diabetes are about 1.5 million deaths.6 Of these records of cases, about 19 million adults in Africa have diabetes, while Sub-Saharan African (SSA) nations accounted for about 14.2 million of these cases in Africa.7 In Nigeria, the DM prevalence was put at 2.2% in 1982, and the overall pooled prevalence of DM was put at 5.77%, with South-South geopolitical zone having the highest DM prevalence in Nigeria.4
As a result of the foregoing, WHO launched a Global Diabetes Compact in April, 2021 to reduce the risk posed by DM and adequate and accessible treatment and care for those already diagnosed with diabetes and adhere to prescribed medicines. Likewise, prevention of Type2 diabetes from obesity, unhealthy diet and inactivity was also of paramount importance in the initiated compact programme.6
Studies on diabetes have revealed the existence of other health conditions that have made the treatment and management of DM a complex issue.8 Some of these conditions include comorbidities with infectious diseases such as HIV and tuberculosis. Other conditions common among DM patients are hypertension, cardiovascular disease and obesity.8 Apart from the comorbidity conditions, issues relating to immunosenescence effects among the elderly, in which immune systems wane with advanced age, have also affected the adult population in SSA.9
There are several studies on DM in Nigeria and beyond.4 Nevertheless, only a few authors approached and identified its risk factors from a Bayesian Perspective. Likewise, this study will be novel in identifying the potential factors of DM in the study area and its environs and will provide an early warning system for individuals and governments. Therefore, this study models DM using a Bayesian regression model of factors associated with diabetes comorbidity among adult patients in Abuja, Nigeria.
METHODS
Study design
This study was a retrospective study based on 162 adult patients receiving treatments in the Federal Medical Centre (FMC), Jabi, Abuja for the sample period of 2012 – 2020.
Study area
Abuja is the capital of Nigeria. It lies on the latitudes N and 7 N of the equator and longitudes E and E of Greenwich Meridian. It has a landmass of approximately 7315 km2. The city of Abuja had a population of about 776,298 inhabitants based on the 2006 population Census.10 Abuja has a guinea savannah vegetation with a typical tropical climate with two seasons yearly.11,12
The FMC, Abuja, was established on the 7th of June, 2012 and commissioned on 28th of January, 2013. The hospital was built and equipped as a comprehensive Hospital in Jabi to expand the scope of health care delivery system.
Data collection procedure
The data used for this study were extracted from the electronic medical records of 162 diabetes patients receiving care at FMC, Jabi, Abuja. Key variables of interest were mined for this study using these medical records. The diabetes data obtained from FMC, Jabi consist mainly that of patients with laboratory-confirmed cases of DM between 2013 and 2020. The diagnostic procedures were based on identifying the presence or otherwise of hyperglycemia in the laboratory analysis of blood samples of patients, which is the most common and precise diagnostic test for DM.13 The blood test commonly called A1C-glycohaemoglobin (measured in percentage) measures average blood glucose or blood sugar level. A normal A1C level is less than 5.7%, prediabetes is between 5.7 to 6.4% while a Type 2 diabetes is above 6.5%.
Variable description
Table 1 describes explanatory variables and various codes employed for the Bayesian Logistic Regression analysis.
Model description
The Bayesian Logistic Regression technique was employed to test the relevant hypotheses in the study using data covering the sample period of 2013 – 2020. In addition, the methods of data collection and tools, as well as techniques of data analysis for assessing the relationship between T2DM with microvascular complications and/or macrovascular complications, were discussed accordingly. The basic idea of Bayesian analysis is straightforward, prompting the analyst to state explicitly:
-
The prior distribution (for instance, a reasonable opinion regarding the patients’ family history of diabetes mellitus excluding the evidence from the clinical or laboratory data).
-
The likelihood (the evidence from the clinical or laboratory data).
-
The posterior distribution (the final opinion about the diagnosis – diabetes mellitus).
The final combination is done using Bayes theorem, which essentially weights the likelihood with the prior distribution. This theorem is thus defined for the purpose of this study in 1.
P(θ/X)=P(X/θ)P(θ)P(X)
Where; is the posterior probability of the parameters given the data
is the likelihood function
is the prior probability
is the normalizing constant
A Logistic regression model expresses a relationship between a two-level categorical response variable also known as binary response and the explanatory variables which can be continuous or categorical (nominal/ordinal). Assuming that the response variable y is binary and the outcomes are called as y = 1 or y = 0 with probability P and 1 – P respectively. For a particular subject, the logistic regression equation is expressed as:
log(P1−P)=β1+β2x1+β3x2+…+βn+1xn
Where …, are the subject’s feature measurements on a group of explanatory variables, and …, are parameter estimates for explanatory variables. With the logit function, it relates the explanatory variables to the probability of an outcome y = 1.
A Bayesian logistic regression extends logistic regression into a Bayesian framework. Instead of using maximum likelihood methods in logistic regression, it applies Bayesian inference, a useful approach specifying the probability distribution for the underlying categorical or continuous variables, to estimate parameter β. Bayesian inference, which allows incorporation of prior beliefs and the combination of such beliefs with statistical data, is well suited for representing the uncertainties in the value of explanatory variables.
The key of Bayesian inference is to choose the parametric family for prior probability distributions. Two categories are suggested: non-informative prior distributions and informative prior distributions. The common non-informative prior distribution is uniform distribution, which assigns equal probabilities to all value possibilities, and always yields similar results as classical statistics. Thus, Bayesian and classical statistics are not exclusive and they are overlapped to some extent. Classical approaches are approximate Bayesian using certain priors. An informative prior distribution reflects specific and definite information about a parameter. If both the prior and posterior distribution belongs to the same family, the prior distribution is called conjugate prior distribution, which is a special case in informative prior distributions. For the purpose of this study, the following were assumed for the Bayesian Logistic Regression technique, a beta prior and a Markov Chain Monte Carlo (MCMC) method was used to obtain the posterior distribution of estimation based on the chosen prior distribution and the likelihood.
RESULTS
Demographic features of sampled diabetes adult patients in FMC, Jabi-Abuja
Table 2 presents the demographic characteristics of the study subjects. Out of 162 patients, 65(40.1%) were male, while 97 (59.9%) were female. The distribution of the result by geopolitical region of the patient showed that the majority of the patients were from South-East 62(38.5%), South-South region had 37 patients (23.0%), North-Central had 34 patients (21.1%), 13(8.1%) were from South-West, 10(6.2%) were from North-East while North-West were the minority 5(3.1%). 11.1% were single and 88.9% were married, the age distributions were as follows; 3.09% of the patients were less than 31years, 8.02% were between 31 years to 39 years, 21.0% were between 40 years to 49 years, 26.5% were between 50 years to 59 years, 25.9% were between 60 years to 69 years, 11.7% were 70 years to 79 years and 3.7% were over 80 years old. The result by occupational background should showed that 1.23% of the patients were bankers, 1.85% were either priest or clergy, 2.5% were lawyers, 3.1% were self-employed, 6.2% were either teachers or educationist, 8.6% were Applicant (unemployed), 8.6% were other form of occupation, 9.3% were House wives, 12.4% were Retirees, 16.7% were Civil servants and 29.6% were Business men/women. In terms of hypertensive status, 32.1% were not hypertensive while 67.9% were hypertensive. The smoking status showed that 3.1% were smokers while 96.9% were not smokers.
The diabetes duration in Table 3, showed that 0.6% of the patients had lived with diabetes for about 26 years to 30 years, 6.8% of the patients had lived with diabetes for about 16 years to 20 years, 9.3% had lived with diabetes for about 11years to 15 years, 10.5% of the patients had lived with diabetes for about 21 years to 25 years, 34.6% of the patient had live with diabetes for about 5 years to 10 years while majority of the patients 38.27% had diabetes mellitus duration of less than five years. The BMI status showed that 2.5% of the patients were underweight, 3.7% of the patients had normal weight. 11.1% of the patients were overweight, 12.9% of the patients were grade 3 obese while majority of the patient 69.7% were obese. The systolic Blood Pressure readings showed that 27.8% of the patients were either stage 1 hypertensive, pre-hypertensive or had normal readings while 16.7% of the patients were stage 2 hypertensive. The diastolic blood pressure readings differed slightly from the systolic observation as majority of the patients 44.4% had normal blood pressure readings, 31.5% of the patients were pre-hypertensive, 18.5% of the patients were stage 1 hypertensive while the minority of the patients (5.6%) were stage 2 hypertensive patients.
Table 3 also reveals the following observations DM; the minority of the patients (0.6%) were either pre-diabetic or type 1 diabetic patients, 33.3% of the patients were DM patients while the majority of the patients 65.4% were Type 2 diabetic patients. The Type 2 diabetes status showed that 33.9% of the patients were non-type 2 diabetic patients while 66.1% of the patients were Type 2 diabetic patients. It was observed that the patients with diabetes complications 87.0% had macrovascular complications while 12.96% of the patients had microvascular complications. Table 3 also shows that among the diabetic patients 11.2% had discordant comorbidity while 88.8% of the patients had concordant comorbidity. HbA1c distribution showed that 3.7% of the patients had HbA1c above 7.0% while 96.3% of the patients had HbA1c less than 7.0% which implies that majority of the patients had normal HbA1c reading.
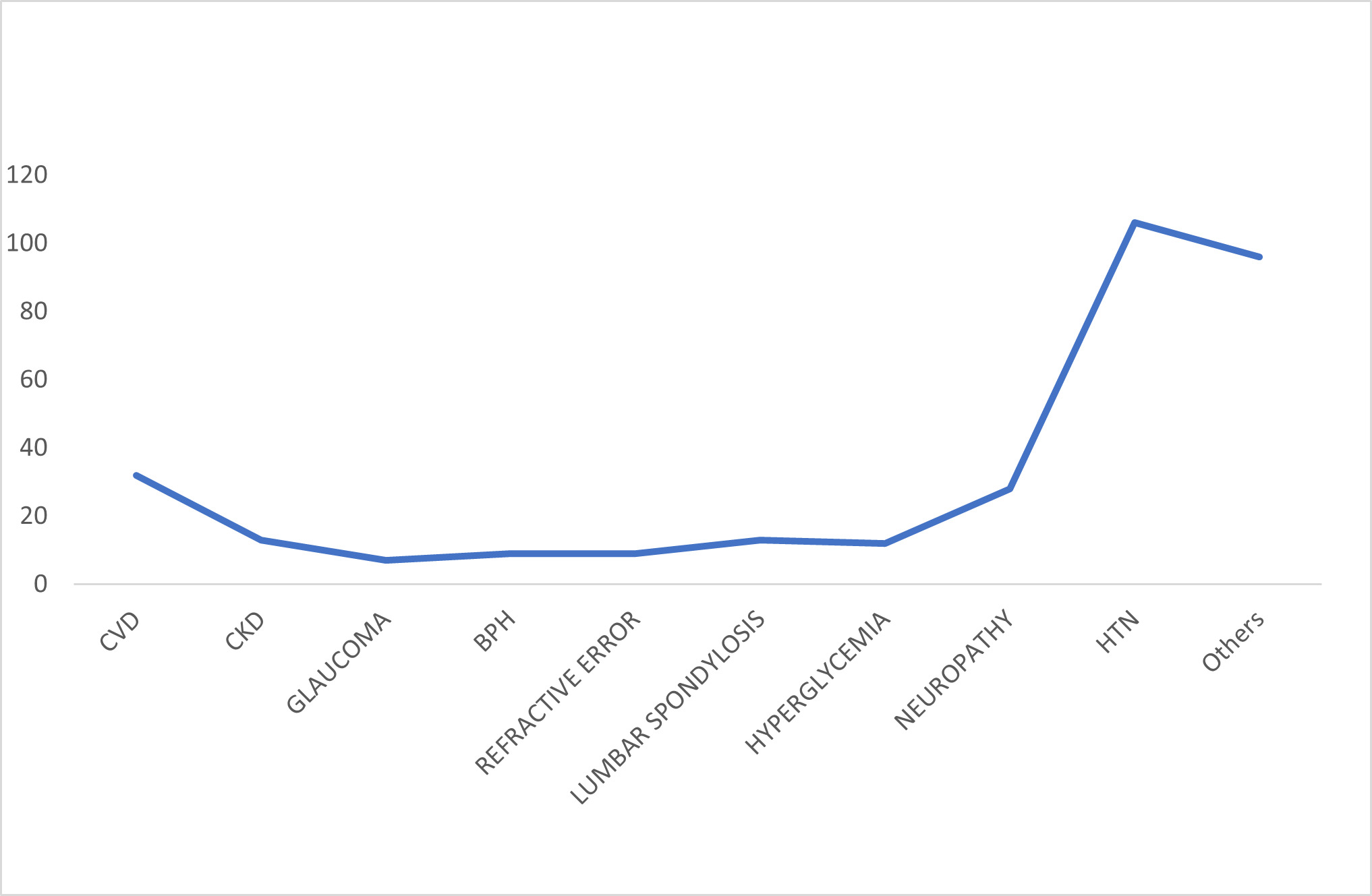
In Figure 1, the line graph showed that hypertension is the most likely comorbid condition for type 2 diabetic patients, followed by cardiovascular diseases and then neuropathic conditions.
In Table 4, 67.4% of Type 2 Diabetic patients had macrovascular complications while 32.6% of non-type 2 DM respondents had macrovascular complications. 57.2% of the respondents with Type 2 DM had microvascular complications while 42.8% of the non-type 2 DM had microvascular complications. 68.5% of the Type 2 DM respondents had Concordant Comorbidity while 31.5% of the non-type 2 DM respondents had concordant comorbidity.
Parameter estimate of a Classical and a Bayesian logistic regression model
Table 5 reveals that gender and smoking were statistically significant association between diabetes mellitus and comorbid.
The Bayesian logistic regression model revealed a positive association between gender and comorbidity; the male patients were 1.65 times more likely to develop comorbidity; patients with history of smoking were 1.56 times more likely to develop comorbidity. T2DM was not associated with systolic blood pressure. Bayesian model produced least standard error compared to logistic regression model (Table 6).
DISCUSSION
The global records of the prevalence of DM in recent times have become a huge public health issue, especially regarding symptoms of one or more other chronic health conditions.4 Some of the variables documented as associated risk factors include sex, age, place of abode, lifestyle, tobacco smoking, family health history and poor glycaemic control, among others.18
The descriptive results revealed a higher prevalence of DM in females than males and in older persons aged 40-69 years. This finding agrees with other related studies documented in the literature.19 The authors found a higher percentage of female diabetes patients, about 53% of the study population, with a mean age of 66 years.
Based on the result of this study, gender, smoking, comorbidity status, marital status, obesity status, HbA1c, microvascular/macrovascular complications and concordant/discordant comorbidity were identified as risk factors associated with T2DM in the study area and its environs. This study’s finding agrees with a related study in literature which documented similar risk factors of DM.18
From various statistical analyses in this study, comorbidity conditions were common, with 159 (98.2%) of subjects considered to have one or more comorbidities. This result is consistent with what has been documented in previous studies.19 Common comorbidities among DM patients are hypertension, obesity, cardiovascular diseases, and kidney diseases. The finding of this study indicated hypertension, cardiovascular disease (CVD), and neuropathy were the three most comorbid conditions associated with T2DM). This also agrees with the findings in a related study.19 Macrovascular complications were identified as positively associated with T2DM, although this was contrary to Li’s submission.14 The authors were of the view that microvascular complications were consequences of T2DM and should not be considered as one of the comorbidities. This study showed that T2DM patients were 2.11 times more likely to have macrovascular diseases.
The study revealed that the odds ratio of present to absence of other disease(s) ranges between 1.01 and 2.71 times with a 95% confidence level. This study also revealed that T2DM was not associated with age; this implies that T2DM may be diagnosed at any age. With reference to the results of the analyses carried out on T2DM, smoking, obesity, comorbidity were found to increase the chance of T2DM. A Bayesian logistic regression model has a satisfactory sensitivity to distinguish between T2DM and non-Type 2 diabetes groups.
Ethics statement
Ethics approval obtained from the Federal Medical Centre Abuja, Nigeria (FMCABJ/HREC/2023/091)
Authorship contributions
DEU: conceptualization, data collection, data analysis, manuscript writing (methodology and data analysis sections). ESO: data collection, data interpretation, literature review, manuscript writing (introduction, literature review, and discussion sections), review and editing. DMO: data analysis, results interpretation, manuscript writing (results and discussion sections), critical review (of the entire manuscript), and final approval of the manuscript.
Disclosure of interest
The authors completed the ICMJE Disclosure of Interest Form (available upon request from the corresponding author) and disclose no relevant interests.
Correspondence to:
Damilare Matthew Oladimeji
Department of Statistics, University of Abuja
Airport Road, Abuja
Nigeria
[email protected]