


.tiff)
_and_repairs_(dotted__blue_line)_from_2004-2018.tiff)
To achieve global sustainable development, it is critical to ensure healthy lives and promote well-being for all at all ages (sustainable development goal, SDG, 3).1–3 Many assume access to medical care is the primary cause of poor health in low- and middle-income countries (LMICs): this is why much of global health policy focuses on providing healthcare goods and services.4 Yet, research has suggested it is not access but quality of medical care that is responsible for poor health among residents of LMICs.4,5 Key to providing effective medical care is an in-depth understanding of the patient population (e.g., demographics, current medical provisions, medical needs), allowing medical care providers and policymakers to identify what medical care is needed and how such care can be provided. This can be difficult to obtain in LMICs, where patient medical records may be sparse, dispersed, and/or inaccessible. This is particularly true for amputees, who often rely on non-hospital facilities and centres for medical care and prosthetic provisioning past the point of amputation.
Prosthetic and orthotic (P&O) centres regularly gather standardised patient data. Recent work has shown how analysis of this type of data can reveal historical trends in the region6 and how there is a gender imbalance in those attending Red Cross P&O centres around the world.7 Transitions in amputee populations, e.g., due to the end of a conflict, can greatly change P&O needs, and thereby P&O development and delivery within a region.6
In 1983, a civil war began in Sri Lanka that would last until 2009. This war used shells and landmines, creating a large amputee population in the north, where the civil war was being fought. Established in 1987, the Jaffna Jaipur Centre for Disability Rehabilitation (JJCDR) has been the sole provider of prosthetics, orthotics, and non-orthopaedic services in the Jaffna Peninsula for more than 30 years.8 Previously known as the Jaipur Foot Programme, the JJCDR is a non-governmental voluntary social service organisation (registration number L 25716) located in Jaffna in the far north of Sri Lanka that was established as a direct consequence of the civil war to help those requiring assistive devices.8 A reported ~70,000 people were killed and ~800,000 displaced, and ~1,000,000 land mines were planted during the war.9,10 Prior to the establishment of the JJCDR, only two other centres provided similar services in Sri Lanka – the Friend in Need Society in Colombo and the Navajeevana Centre in Tangalle – both of which were hundreds of kilometres south of Jaffna and on the other side of the front-line.11
Since its founding, the JJCDR has maintained extensive medical records of its patients. In 2004, with the help of Motivation (https://www.motivation.org.uk/sri-lanka), the JJCDR transferred its records to an electronic database. Some of this data has been summarised and published in a document online.12 Amputee databases and datasets are rare, even in high-income countries,13,14 but necessary for the development and delivery of efficient P&O services.6 Depending on the data contained, these datasets can be used to
-
Develop patient-specific comprehensive care plans to maximize functional activity and community participation,
-
Identify ongoing medical trends and develop efficient intervention plans to improve community health,
-
Investigate questions of socio-political, gender, ethnic, race, and income inequalities,7
-
Identify spatial distribution of such inequalities and amputees to improve medical provisioning, and
-
Investigate the socio-political history of an area, and understand how it affects medical provisioning, both past and present.6
Here, we introduce the JJCDR database, perform preliminary investigatory statistical analyses and discuss possible limitations of the dataset. Through this analysis, we (1) provide necessary baseline data for providing efficient medical care to amputees in northern Sri Lanka, (2) demonstrate the usefulness of this database in identifying key events in Sri Lanka’s history, and (3) identify current trends necessitating intervention.
Methods
The JJCDR collects information relevant to the provision of prosthetics, orthotics, and non-orthopaedic services and records the information in a digitized electronic database. The database contains patient records of all individuals who have accessed JJCDR services since its establishment in 1987. Data was collected by patients when they registered with the JJCDR and updated on subsequent visits, and includes basic patient information, financial records, and information about the medical devices provided by the JJCDR to the patient.
Access to an anonymised Microsoft Access version of the database was supplied to Imperial College London (ICL) researchers on 29 November 2018. To protect anonymity, patient addresses were limited to village level and date of births were binned to a quarter of a year before database acquisition to ensure anonymity without eliminating useful information (i.e., Jan-March = quarter 1, April-June = quarter 2, etc.).
All tables in the database were imported into Microsoft Excel 2013 and saved as *.csv files. Descriptive statistical analyses were carried out in R15 and RStudio.16 Ggplot217 was used for visualization. Most data were extracted directly from the database. However, some data alterations were made: details for this are listed below. Unless otherwise stated, all data was included in these analyses.
Inclusion criteria for this study was people receiving prosthetic, orthotic, or rehabilitation services and having a written record with the JJCDR when the database was digitized in 2004.
Demographics
Year of registration was taken directly from the database, and age first seen was estimated by subtracting year of registration from year of birth. Year of amputation was taken directly from the database, and age of amputation was estimated by subtracting year of amputation from year of birth. One excluded individual had a year of amputation after 2018, which was not possible given the data was access in Nov 2018. Nineteen individuals were excluded as they had negative ages of amputation.
Financial
Before the creation of the electronic database in 2004, most jobs/repairs did not have associated costs recorded. As such, financial data before 2004 should be viewed as incomplete.
Data availability
Given the sensitivity of the data, the data agreement between the JJCDR and other researchers, and the possibility that individuals could be identified using information from this database (e.g., using age, amputation location, and village, it may be possible to identify amputees), the database has not been made available with the article. The database can be accessed by contacting the leading author of the study and/or the JJCDR directly.
Ethics
Ethical approval was obtained from London South Bank University (reference number: ETH2122-0172) and the University of Jaffna (reference number: J/ERC/22/136/NDR/0275).
Results
General
Nineteen *.csvs were needed to capture the full range of data (Table 1). Some columns in the *.csvs contained duplicate data (e.g., patient ID, job number), allowing *.csvs to be connected. File names were derived from the Table names in the Access document provided by the JJCDR.
The database contained medical and patient data for at least 3,665 patients, orthopaedic history information for 3202 patients, and financial records for 10,404 transactions. Financial information was split between “jobs” and “repairs”: jobs correspond to the fitting of a new medical device and repairs the maintenance of those devices. Jobs and repairs were assigned unique job numbers. Jobs were assigned integer job numbers, and repairs were assigned the integer value of the job being maintained plus 0.01 for each repair on the device, making it possible to link repairs to specific jobs, e.g., a device with a job number of 374 that is being repaired for the third time will be assigned a job number of 374.03. Patients were entered as “deceased” when they were (i) deceased, or (ii) there had been no contact with the patient for 5+ years.
Demographics
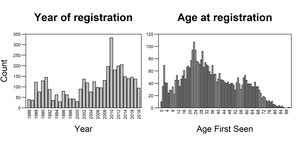
The Patient *.csv was used for demographic analysis. It contained 3,663 unique patient IDs stored corresponding to 3,665 unique patients who registered with the JJCDR from 1986-2018 (M= 2,605, F =1,060; see Limitations of the JJCDR Database). From 1986 to 2018, the centre had approximately 97-111 new patients registered yearly (mean = 111, median = 97; Figure 1). More new registrations occurred in 2010 (n = 333), a year after the civil war ended, than any other year. Although the JJCDR was established to aid those afflicted by war, it has had, on average, more new patients register per year after the war ended (2010 onwards; mean = 176, median = 148) than it did when the war was occurring (1986-2009; mean = 83, median = 79).

Age at time of registration ranged from 0 – 90 years old with a mean/median age of 34.76/32 years old, and more people registering at 23 years old (n = 107) than any other age (Figure 2). 21.4% (783/3,665) of the patients were 0-18 years old at the time of registration.
Data on civil status was recorded at the time of registration. Of the 3,357 patients with civil status recorded, 2,179 were married, 1,166 single, 6 divorced and 6 widowed. Occupation was recorded for 15.1% (555/3,665) patients in the Patient *.csv (Table 2). The most held occupation was housewife, followed by unemployed and labourer (i.e., patients who partake in whatever labour is available). The term “housewife” does not necessarily refer to a married woman, but is a general term used for a person without a job who takes care of the household and has domestic responsibilities (e.g., cleaning, cooking, laundry, etc.). In some countries (e.g., Cambodia) it does not necessarily refer to a woman, but it is uncommon to find older men who identify as housewives. In our database, one housewife was listed as male (age: 57) and the rest were female.
Patients seen by the JJCDR with address details (3,660) came from 909 villages representing 22 districts and 9 provinces. 94.4% (3,455/3,660) of patients had addresses in the Northern Province. Of those, 82.5% were from the Jaffna District (2,851/3,455; Figure 3). Given JJCDRs location, it was expected most/all of patients would be from the Jaffna peninsula: however, 17.5% (604/3,455) of the patients came from the surrounding districts in the Northern Province. This may be because the JJCDR was the sole provider of prosthetics and orthotics north of Colombo when founded, with other local centres (e.g., the Jaffna White Pigeon Technical Institute of Prosthetics in Kilinochchi, Valvuthayam Mannar Rehabilitation Center, and Handicap International Physical Rehabilitation Center in Batticaloa) being founded at later dates.18

Relevant Medical History
Here, we present data pertaining to the patient’s medical history, specifically related to their amputation. There were 3,202 patients with historic orthopaedic information (OrthopedicHistory *.csv). Of these patients, 2,489 were admitted for amputations, 705 for orthotic assessment, 6 for arthrodesis and 1 patient each for arthroplasty and laminectomy. Patients were admitted to 84 hospitals, 66% (2,100/3,202) being admitted to Jaffna Teaching Hospital (Table 3). Most care given to patients prior to the JJCDR is from the public sector, with the private sector only accounting for 4.0% of admissions (129/3,202).
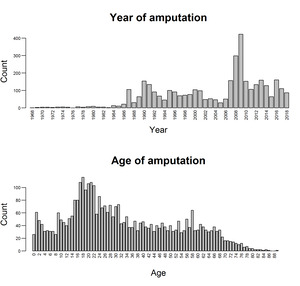
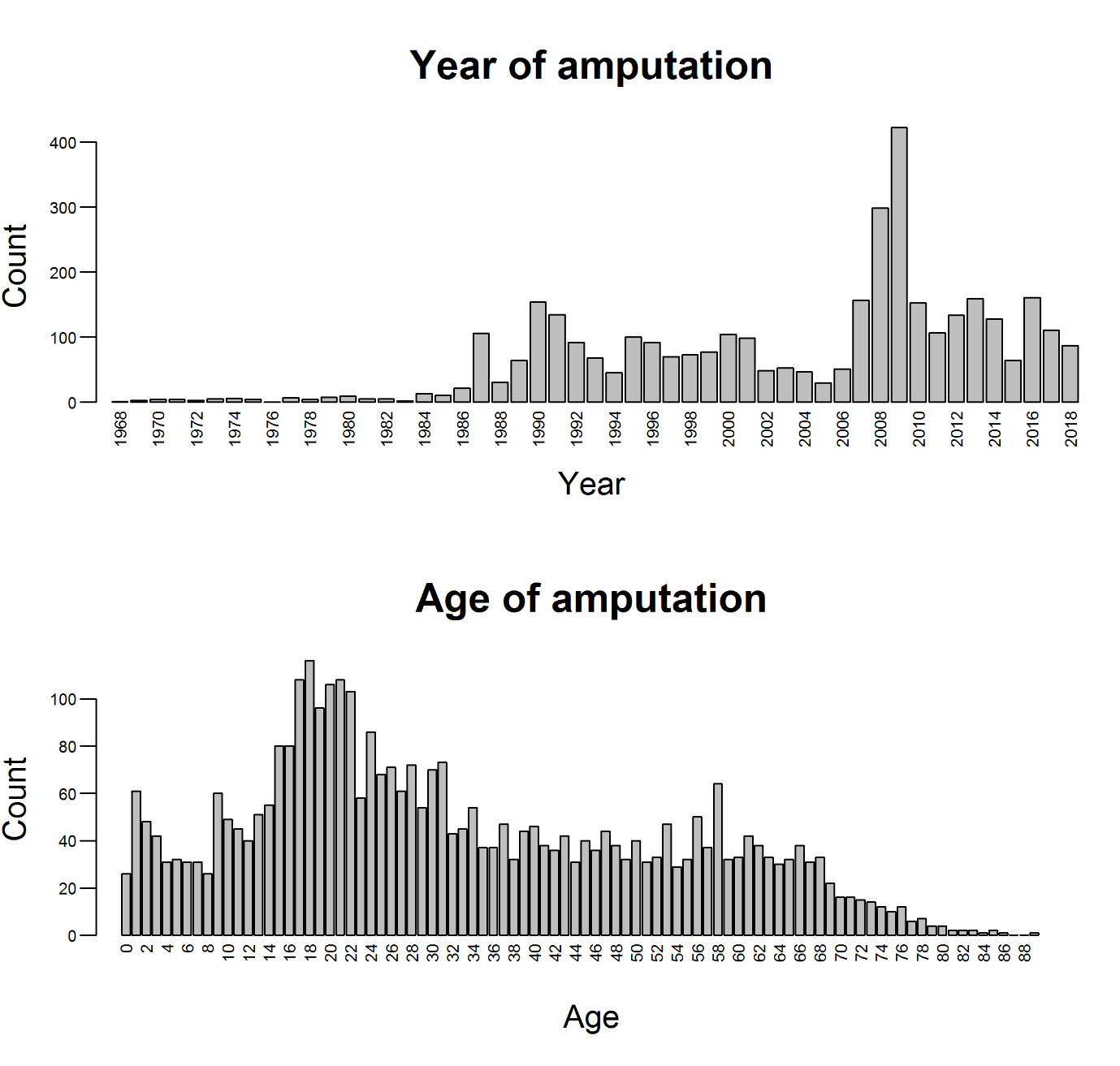
The Medical *.csv contained information on date of amputation, which was combined with information from the Patient *.csv to determine age of amputation. All 3,654 unique patient IDs in the Medical *.csv could be found in the Patient *.csv. It was not possible to match the two sets of individuals with duplicate patient IDs in the Medical *.csv, meaning all four individuals were excluded. The breakdown of year and age of amputation for the 3,652 remaining individuals is given in Figure 2. The mean/median number of amputations per year was 71.33/53, with more people receiving amputations in 2009 (n = 422), the last year of the war, than any other year. The mean/median age of amputation was 33.12/29 years old, with more people receiving amputations at 19 years old (n = 116). 25.1% (915/3,652) of patients were 0-18 years old at the time of amputation.
Of the 3,654 patients with treatment data (MedicalRecord *.csv), 2,548 had either unilateral or bilateral amputations. 24 patients had information on cause but not site of amputation or if it was unilateral or bilateral. Of those with data, 96.6% (2,462/2,548) had unilateral and 3.4% (86/2,548) had bilateral amputations. Of the bilateral amputees, 8.1% (7/86) were bilateral upper limb, 80.2% (69/86) were bilateral lower limb, and 11.6% (10/86) had no data on site of amputation. One of the bilateral lower limb amputees was a triple amputee, and six of the unilateral amputees had upper and lower limb amputations.
The distribution of site of amputation is given in Table 4. Ten of the bilateral and 77 of the unilateral amputees had no information on site of amputation, and two of the bilateral amputees had only one amputation listed. The amputation site was missing for 3.7% (99/2,641) amputations. 69.1% of amputations were transtibial (1,756/2,542; Table 4), which may, in part, be due to the large number of land mines that were planted in northern Sri Lanka.9
Of the 69.1% of patients with geographic location of injury data (2,525/3,654; MedicalRecord *.csv), 94.3% (2,382/2,525) were wounded in the Northern Province. Within the Northern Province, most were injured in Jaffna District (68.0%; Fig 4). Not all people have current addresses in the same provinces/districts of injury.

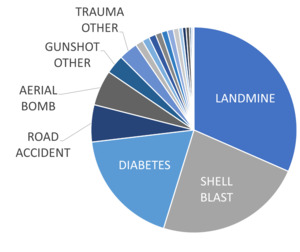
There were 2,556 patients with reason of amputation recorded (Fig 5; Table 5). Most amputations (61.2%; 1,564/2,556) were war-related (i.e., aerial bomb, gunshot war, landmine, or shell blast). Temporal distributions for the four most common causes of amputations are in Figure 6. Each person is counted once, even if they have more than one amputation. The temporal increase in amputations due to diabetes in consistent with global trends.20–22
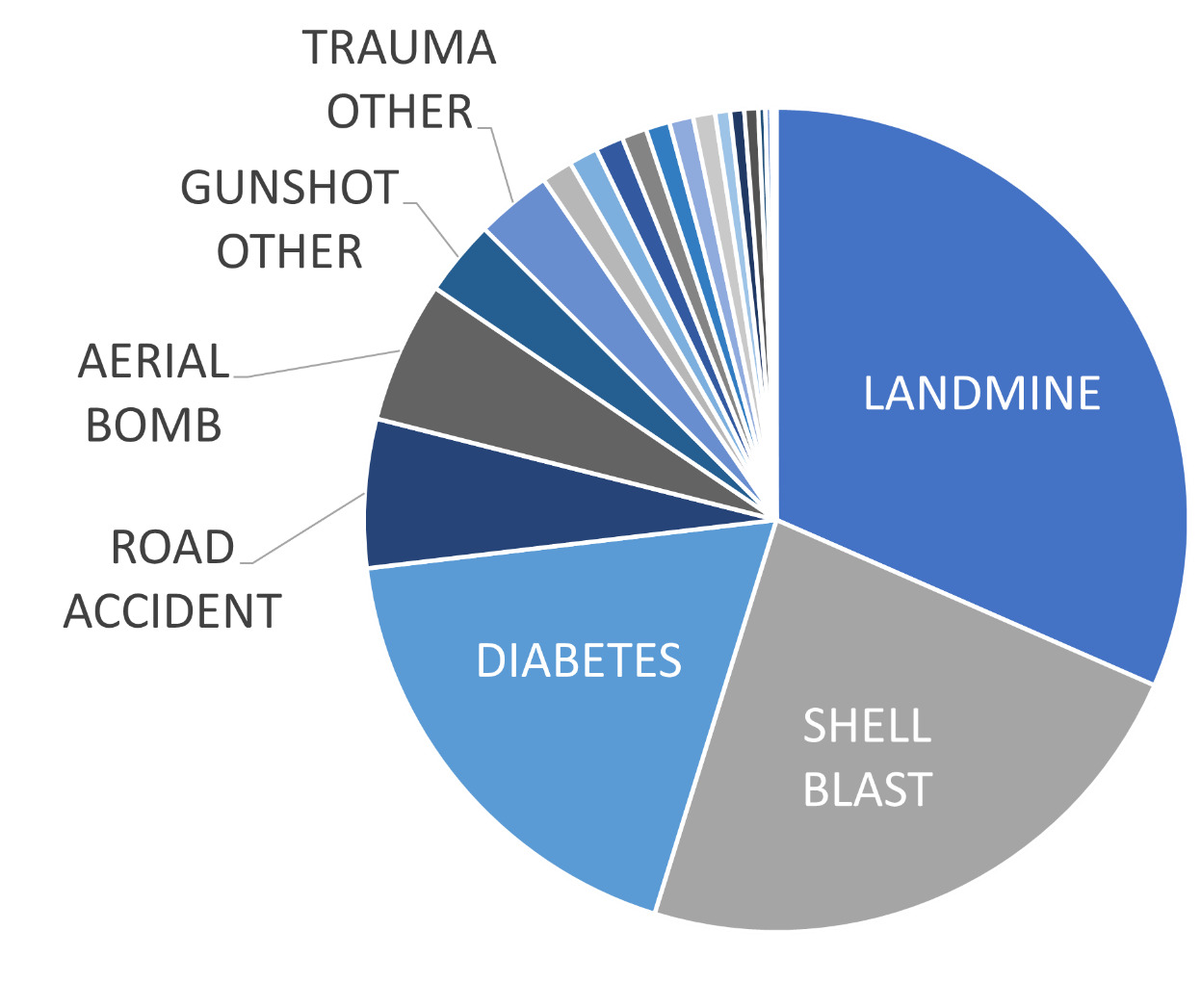

Landmine and shell blast were the two most common reasons for amputation, being the reason for amputation for 54.8% (1,400/2,566) of the patients and occurred even after the war concluded. Diabetes was the largest non-war-related reason for amputations (18.3%; 469/2,566). Consistent with global trends,23–25 diabetic amputations appear on the rise in northern Sri Lanka.
Financial
The JJDCR receives some public funding but relies largely on donations to provide amputee care.8 Between the Finances and FinancesDetailsJobs *.csv’s there were a total of 10,405 job numbers that had associated costs. These costs correspond to the cost of supplies necessary to manufacture or repair the device itself (e.g., for an articulated ankle foot orthosis, AFO, this includes POP Bandage, POP Powder, flexural joints, polypropylene sheets, strap, two sizes of Velcro, two loops, and four buttons), as well as costs of labour and overheads. It does not correspond to costs associated with rehabilitation, patient travel, room and board, or research and development into new technologies. Some of these services (e.g., rehabilitation, board) are provided free of cost to patients in an as-needed basis.
The total cost of jobs and repairs in the JJCDR electronic database were 94,540,927.50 LKR and 10,802,547.50 LKR (£402,682.00 and £46,011.72), respectively. A breakdown of costs is provided in Table 6. Additional information concerning the calculations of the financial data are presented in the Supplementary Information S1 text.
To investigate temporal changes in costings requires data from the Finances, Jobs, and Repairs *.csvs. Jobs contained three dates per job: date of patient assessment, product commencement, and product delivery for all jobs. Year of commencement was used to investigate temporal trends. Repairs only contained one date – date of repair – which was used to investigate temporal trends. In Jobs, there were 7,892 unique jobs, and 99.5% (4,682/4,705) of jobs with costings had associated date information. In repairs, there were 10,402 unique repairs, and 99.6% (5,676/5700) of repairs with costing had associated date information.
Fig 7 compares the number of jobs/repairs per year against the number of jobs/repairs per year with associated financial costs. Most of the financial record keeping for the jobs and repairs commenced in 2004 and 2007, respectively. A spike in the number of repairs occurs in 2013, three years after the spike in registrations and jobs. A closer examination of this data will reveal which prosthetics and orthotics are failing, and when, where, and how they are failing. When combined with occupation data, it may reveal which occupations carry the largest risk of breaking which components, which can help with the redesign of occupation specific devices.
.tiff)
From 2007-2018, the mean cost to the centre per year for jobs and repairs was 7,220,390 LKR ± 2,883,980 (£30,754.10 ± 12,283.85) and 870,291.60 LKR ± 668,351.50 (£3,706.87 ± 2,846.74), respectively. The total cost (sum of jobs and repairs) and patient costs of jobs and repairs against year is shown in Fig 8. From 2007-2018, the mean cost to the centre per year was 8,090,682 ± 3,481,167 LKR (£34,460.96 ± 14,827.48). The centre experienced peak costs in 2013, due to an increase in both jobs and repairs. This data is particularly useful, showing new devices incur a heavier cost on the centre than repaired ones, and can be used to predict costs associated with prosthetics and orthotics in coming years.
_and_repairs_(dotted__blue_line)_from_2004-2018.tiff)
Discussion
Data on local amputee populations is rare, even in high-income countries.13 The JJCDR database offers a unique insight into the P&O population of northern Sri Lanka. Interrogating the database has revealed unique baseline data necessary for providing efficient medical care to amputees in northern Sri Lanka, demonstrated the usefulness of this database in identifying events in Sri Lanka’s history, and identified current medical trends necessitating intervention.
Most individuals in the database were male and less than 35 years old at the time of amputation, with a large percentage (21.4%) 18 or younger. This is likely a consequence of the civil war, although there were a significant number of women who played a major role in the war.26 This is supported by the large percentage of individuals who suffered from war-related amputations (Fig 5; Table 5).
The large percentage of young individuals with war-related amputations has many long-term implications for the communities of northern Sri Lanka. Amputation is a lifelong condition, meaning amputees require medical aid their entire life: having such a large population of young amputees implies the north will need decades of aid to help these individuals. Additionally, research has shown blast-related amputees can suffer from a condition known as heterotopic ossification, where bone begins to form in the residual limb.27 This can cause irritation and pain, requiring follow-up surgeries to remove the newly formed bone. The large percentage of amputations due to blast injuries (e.g., shell blasts, landmines) suggests many people may require follow-up surgeries, and/or have decreased functionality as they age.
It was not possible to determine length of occupation, or if patients changed occupation after amputation. Through conversations with amputees, we discovered many amputees were forced to change occupation following amputation, and many would return to their previous occupation if they could. For example, we met many lower limb amputees who were farmers before their amputation but were forced to change occupation post-amputation as their prosthetic feet would often get stuck in the mud. All the individuals we interviewed would return to being a farmer if they could. Improved occupation data, including not only people’s current but also desired professions, could serve to improve prosthetic/orthotic devices through the design/production of function-specific prosthetics. This would improve device functionality, and longevity, increasing amputee quality of life while decreasing the JJCDR’s workload.
A recent review of procurement of medical services in LMICs suggested a large percentage of patients utilized private medical care.4,5 The high proportion of amputations in public hospitals suggests this pattern may not hold true in Sri Lanka, and/or this pattern may not hold true for major surgeries and/or war injuries, like amputations. This does, however, correspond with the understanding that most Sri Lankans are treated in public hospitals.28 Further interrogation of this database can produce critical information related to the year and age of amputation, such as the numbers of children and juveniles affected by war-related injuries, like land mines.
Most amputees had lower limb amputations: this could be related to the large percentage of war-related amputations. Anti-personnel mine blast is primarily associated with lower limb amputation, as the primary blast wave and secondary detonation products come into close contact with the foot. This initially damages and subsequently causes massive trauma to the lower limb.29 At least some of the upper limb amputations were also due to landmines. Some civilians have been reported to excavate and dismantle landmines to use the explosive for alternative purposes (e.g., fishing). Occasionally the mine detonates during dismantlement, resulting in the loss of one or both hands/upper limbs, as well as facial (e.g., eye) injuries.30
There were no through knee amputations. Generally, through knee amputations yield better long-term results than transfemoral amputations due to a longer residual limb with a load bearing distal end, and the potential for self-suspension of the socket over the residual limb.31,32 Through knee amputations are uncommon in LMICs,33,34 as it is difficult to fit a prosthetic over the stump which positions the centre of rotation for the knee joint correctly, and there are few affordable, commercially available prosthetics for through knee amputees.35
These analyses represent brief overviews of what can be learned from this database. They highlight the usefulness of using this type of data in investigating socio-political trends. For example, the spike in shell-blast amputations observed in 2009 (Fig 6) corresponds to the intense clashes between the Sri Lankan government and the Liberation Tigers of Tamil Eelam (i.e., the Tamil Tigers, LTTE) during the last year of the war. Although less clear, this spike can still be seen in Fig 1 where there is no differentiation between type of amputation, implying it is not necessary to know cause of amputation to see these trends. Additionally, these analyses highlight the usefulness of using this type of data in planning for the community’s future. For example, the decrease in mine-related amputations suggests the demining efforts by organizations like the HALO Trust have been successful. However, the increase in diabetic amputations suggests (community) interventions are needed to improve diabetic care.
Limitations of the JJCDR Database
One of the limitations presented here is the incompleteness of the database, as it is not always possible to gain all information on all patients, and the database does not contain information on the entire P&O population of northern Sri Lanka. However, very few good databases like this exist for LMICs, particularly those in conflict zones. A major benefit of this database is the JJCDR was the sole provider of these services in the northern region for several years, including through the civil war, and still serves as a primary prosthetics and orthotics centre today. It is therefore reasonable to assume this database provides a good view on the prosthetic and orthotic (P&O) population in northern Sri Lanka.
Another limitation is patient IDs. Patients were identified using unique patient IDs which were occasionally assigned to more than one patient. E.g., 7 of the 3,659 patient IDs in the medical *.csv (0.2%) were assigned to two patients. When analysing the database, duplicate IDs were either 1) deleted, if data from additional columns in the *.csv were identical, or 2) treated as two separate patients if data from additional columns in the *.csv were not identical. Duplicate patient IDs cause us to make potentially incorrect assumptions about the patients served by the JJCDR.
According to the summary patient data recorded in the register, the JJCDR had provided 7,005 prosthetics (6,737 lower limb and 268 upper limb) from July 1987 – May 2016, but as some amputees have received several prosthetics, this does not correspond directly to the number of patients. No *.csv contained more than 3,663 unique patient IDs. There is a possibility more than 3,663 patients have received prosthetics because 1) exhaustive records were not always kept on all patients prior to the electronic database in 2004 and 2) not all data is available for all patients in the electronic database, as some patients gave false information to the centre. Finally, the data reported here for 2018 does not include the month of December.
In LMICs, the creation of electronic databases, such as the one employed at the JJCDR, can be challenging due to poor quality and incomplete original records, lack of personnel, and limited resources.36 Given these hurdles, we believe the limitations discussed here are acceptable, and the JJCDR database represents a vital tool to investigating a cohort of those requiring P&O services in Sri Lanka.
Conclusion
Despite challenges, the JJCDR has been able to digitise and maintain a prosthetics and orthotics database of thousands of patients. Here we presented the JJCDR database, and performed preliminary demographic, medical and financial analyses on the database. This data will be of great value to the centre for improving future care as metrics such as prosthetic efficiency, patient outcome and demand on the centre can all be monitored. In the future, increasing data quality will aid the JJCDR in providing high-quality P&O care for northern Sri Lanka and help researchers provided targeted aid to this population. It further shines a light into the needs of P&O centres in LMICs, and what can be done to help both these centres and their patients.
Acknowledgements
The authors thank the members of Imperial College London’s Musculoskeletal Modelling and Biomechanics research groups and Lucy Foss for useful discussions on the database. The research was commissioned by the National Institute for Health Research using Official Development Assistance (ODA) funding. This work was part supported by the Royal British Legion Centre for Blast Injury Studies who provided logistical support to help with data collection. They were not involved in data analysis, or in the presentation of the results.
Disclaimer
The authors declare no conflict of interest for this study.
Ethics statement
Ethical approval was obtained from London South Bank University (reference number ETH2122-0172) and the University of Jaffna (reference number J/ERC/22/136/NDR/0275).
Funding
Funding for this project was provided by the National Institute of Health Research (NIHR), awarded to Professor Anthony Bull.
Authorship contributions
MAB, SB, SH, JCC, AK, GS, and JG conceived of the study. AK, GS, and JG gathered the data and MAB and GS received ethical approval. MAB and SB cleaned the database, performed statistical analyses, and created figures/tables. MAB and SB wrote the initial draft. MAB, SB, SH, JCC, AK, GS, and JG edited the draft and approved its final version.
Disclosure of interest
AK worked for the JJCDR, and GS has done unrelated work at the JJCDR. JG was a co-founder of the JJCDR.
Correspondence to:
Michael Berthaume
Department of Engineering, King’s College London
Strand Building, Strand Campus, Strand, London, WC2R 2LS
United Kingdom
[email protected]