The World Health Organization (WHO) states that a healthcare system should improve population health, prevent healthcare costs, and meet health expectations. Risk sharing and financial protection are crucial since health care is expensive and uncertain.1 Responding to people’s expectations shows respect for dignity, autonomy, and information confidentiality. Improving health means increasing the population’s average health and reducing health disparities.2 Life expectancy and health care access have improved worldwide in recent decades.3 These advancements have greatly increased wellbeing.4 The microeconomic studies on health and worker productivity, education, and savings suggest that improved health boosts economic growth.5 However, some macroeconomic research shows a big and meaningful influence.6,7 Hence, health reforms are more and more becoming a key priority in all countries to address/ improve the accessibility, affordability, and availability of quality services along with improved efficiencies in spending.8
By definition, secondary benefits are any additional effects that may arise from a project’s economic ties.9 When pertaining to health - secondary health benefits are the additional benefits received by an individual or community apart from the original objective as a result of the presence of a project in a specific geographical area.10 Second-order health benefits may include: An increase in equity, employment, literacy level, women’s education and empowerment, income, productivity, local wealth and lifestyle. These may also lead to a decrease in out-of-pocket expenditure, poverty, socio-economic, geographic and gender inequalities. Fostering local partnerships with communities, innovations and implementation of technology, upscaling of human resources and infrastructure development, and opportunities for advancement and career development are also included as second-order benefits.
However, second-order benefits of Health systems are little researched and not discussed in mainstream policies and practice. This report explains the rationale, evidence, and methods for understanding the health schemes’ significant potential socio-economic impacts and linking the indirect impacts/association by health systems in other facets. The work aims to support broader efforts to see health systems as critical in promoting equitable and inclusive development in benefiting the entire community, particularly those who are frequently left behind.
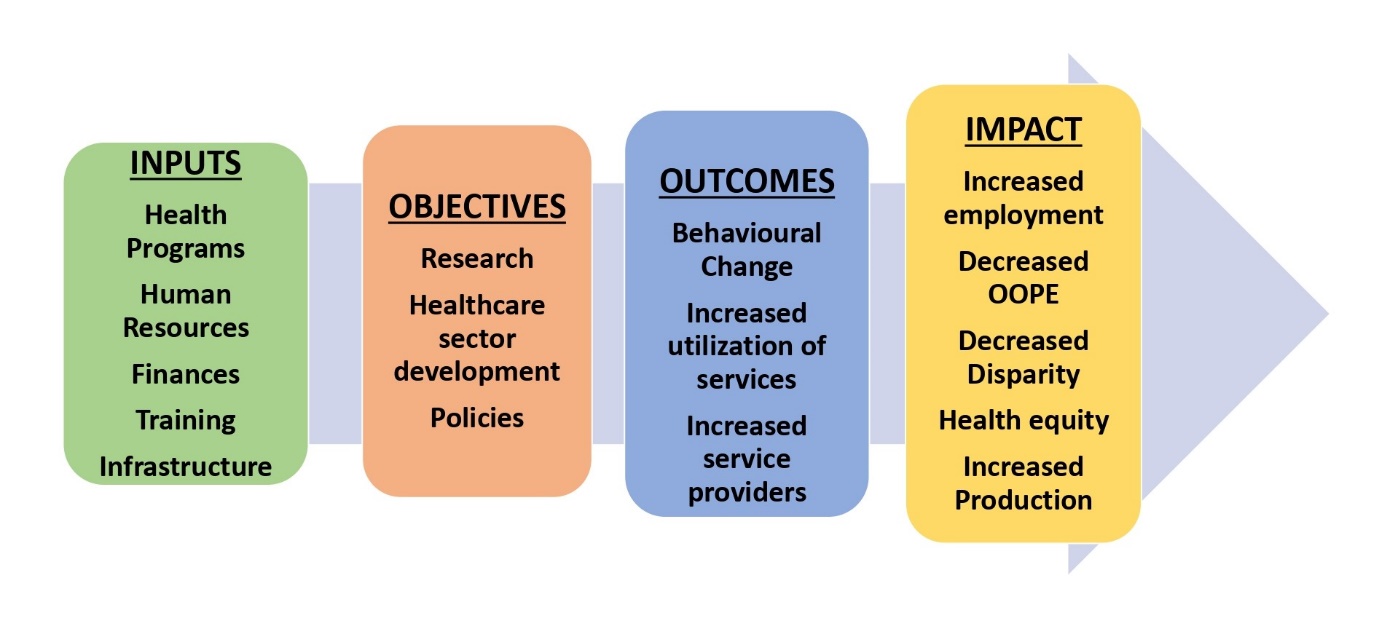
Logical framework
The logical framework approach (Figure 1) was used to evaluate the second-order benefits of the health schemes. The inputs, objectives, outcomes, and impacts (primary and secondary) were compared. To assess coverage, independent household sample surveys such as National Family Health Surveys (NFHS) and National Sample Surveys conducted on a regular basis by independent agencies, the government of India’s budget and rural health statistics were used.

Employment opportunities and their benefits
The health sector has always been a source of employment generation, directly for the healthcare workers and indirectly for all those involved in medical infrastructure, supply chain, medical technology, pharmaceuticals, logistics, etc. Total private infrastructure accounts for nearly 62% of all of India’s health infrastructure with 43,486 private hospitals11 and linked with this growth is the exponential increase in the jobs in the fields of medicine, nursing, allied and other healthcare workers, medical technology manufacturing drugs and maintenance, diagnostics and vaccines; infrastructure creation and maintenance, healthcare management, etc.
The concerted efforts towards health system strengthening under National Health Mission (NHM)12 have also seen an exponential growth of human resources and health institutions. From 2006 to 2022, the number of Accredited Social Health Activist (ASHA) has risen to approximately 1.04 Million, Auxiliary nurse midwives (ANMs) to 207,587 from 133,194, Allopathy Doctors to 30640 from 20308, specialist Doctors to 4485 from 3550 and Community Health Centres to 5649 from 3346.13,14 Overall, 0.26 Million contractual healthcare workers have been employed under NHM and recently more than 0.125 Million Community Health Officers (CHO) have also been added.
Healthcare financing has increased, which led to infrastructure development and increased employment opportunities. In the Union Budget 2023-24, the health sector has been allocated INR 891,550 Million15 as against INR 739, 320 Million allocated in 2021-22 and INR 102,800 Million in 2005-06. Healthcare financing also helped the growth of healthcare training institutions, the 15th Finance Commission has recommended allocating more than INR 130,000 Million for the training of allied healthcare workers, which is expected to create an additional 1.5 Million workforce.16 From 2014 to 2023, a 67% increase in Medical Colleges to 648 from 387, 87% increase in Medical seats to 96077 from 51348 and 105% increase in medical Post graduate seats to 64059 from 31185. Since 2018, 22 new All India Institute of Medical Sciences (AIIMS) have been established out of which 6 are functional and 16 are in the process of completion. Allied training institutes like General Nursing Midwifery (GNM) have increased to 3215 from 2865 and Nursing colleges to 1936 from 1641 between 2014 and 2018.17 There have been considerable employment opportunities across government sector, private hospitals, Third party administrators (TPAs), insurance companies and other such related sectors. Innovative business models encourage new market entrants and setting up of economical hospitals as per an early analysis of the Ayushman Bharat – Pradhan Mantri Jan Arogya Yojana (AB PM-JAY).18 The Health schemes have changed local communities by raising local income, as staff who live locally spend locally, which improves economic and social resilience, and lowering carbon emissions, as people travel less to work. Health workers living and spending locally improve housing, nutrition, social cohesion and the environment.19
Benefits of local partnerships with communities
Health schemes have resulted in massive public institution purchasing budgets, which are unquestionably an opportunity to build sustainable local economies and communities. Public procurement in India accounts for 20 - 22% of GDP and 11.13% of government spending.20 Supply chains contribute to economic growth, job creation, poverty reduction, entrepreneurship, and workers’ transition from the informal to formal economy; it is thus a powerful route for supporting, enabling, and strengthening local businesses, fostering growth and increasing local employment.21 Health schemes partner with government departments and ministries (finance, commerce, business, and development sectors); education (primary, secondary, and higher education); businesses (private and social enterprises); civil society organizations/the third sector; and local communities.22
Decreased inequities and population-level impacts on socioeconomic development
After the launch of various national health schemes over a period, a significant reduction in socioeconomic, geographic, and gender disparities has been observed. Trend analysis of several cross-sectional surveys from 1995-96 to 2019-21, clearly shows increasing institutional deliveries from 43% to 95.5%, with almost 100% coverage in many of the states which evidenced a large reduction in the magnitude of inequity in institutional delivery.13 This increase in proportion was about similar across all socioeconomic groups, the differential rate of relative increase (i.e. from 16% to 45% in poorest district quintile vs from 40% to 69% in richest ones) has helped to reduce inequities.23
Adolescent Friendly Health Clinics in Rashtriya Kishore Swasthya Karyakram (RKSK)24 have resulted in more intervention at the adolescent life stage with wider social variables such as poverty, child labor, education, societal, and familial pressures.25 Adolescent engagement in group discussions and value-added lectures resulted in larger societal consequences such as peer influence, community engagement, interpersonal relationships, integrated community, and adolescent empowerment.26 To complement this, USAID review on adolescent interventions discovered enhanced gender equality and decreased violence.27
Women empowerment
Literature shows that social support from healthcare staff during pregnancy empowers women to make home decisions, which improves children’s educational outcomes.28 A mother who can freely move around is more likely to get useful child health and educational development information and visit health centers for necessary health checkups.29 As a result of conditional cash transfer in Janani Suraksha Yojana (JSY) (30), 81% urban and 77.4% rural women own a bank account that they operate themselves.13 Overall, there has been a big jump in numbers, with 78.6% women across India owning bank accounts as compared to 53% as recorded in 2015-16.30,31 Increase in women literacy and owning of bank account contribute to women empowerment.
Comparison of NFHS-4 and NFHS-5 shows an increase in percentage of married women who participate in their household decisions as 84% to 88.7%, and also women owning a house and/or land (alone or jointly with others).13 The number of Auxiliary Nursing Midwife (ANM) at subcenter (SC) and Primary Health Centre (PHC) increased to 207587 from 133194, which is 55.9% rise between 2005 and 2022. Overall, 21501 Health Worker (Female) / ANM are in position at urban PHCs, with 13.4% posts vacant out of the total requirement at all India level.14 A total number of 83,767 female CHO and 2,33,278 Female Multi-Purpose Worker are in position at Health and wellness Centers (HWC).32 More than 60% of team leaders (CHOs and Medical Officers) and more than 90% of field workers of HWC teams are women.33 All these clearly indicate a surge in women employment and a gender sensitive approach to healthcare contributing to women empowerment.
Increase in literacy and school completion rates
Educational attainment is critical in imparting the feeling of self-worth and self-confidence and enhanced education of mothers has declined the inequalities.34 In JSY program, encouragement of behaviour change towards later marriage has been reported coupled with women delaying their first pregnancy by 3-4 months and postponing pregnancies over the age of 19 in order to qualify for JSY cash transfers. Because the programme has a significant impact on women’s first pregnancies, it is considered to improve girls’ high school completion rates,35 similar to the results of a cluster randomized trial from Malawi by Baird S, where conditional cash transfers (CCT) have significantly reduced the dropout rate to 43% among its beneficiaries on the completion of school education in girls and avoided teenage pregnancies.36
Comparing NFHS-4 and NFHS-5, Infant Mortality Rate (IMR) and Under-five mortality rates (U5MR) have decreased from 40.7% to 35.2% and 49.7% to 41.9%, respectively, which encouraged people for family planning acceptance, increasing it from 53.5% to 66.7%. Also, NFHS-5 points to a literacy rate among adult women (15-49 years) as 71.5%, compared to 64.64% as per 2011 census.13 Small family size leads to increased finance availability for education and other socio-economic activities, which improves quality of life.
The adolescent health clinics in RKSK program are likely to have played a vital role in the continuation of adolescent girls’ education, avoiding early marriage and childbearing in the future, and reducing teen pregnancies. It is also supposed to increase knowledge about various government schemes and how to use them properly, which ultimately leads to women’s empowerment, employment and a better quality of life.37 This is much evident from the drop of adolescent fertility rate (birth/1000 women between 15-19 years) from 51% in NFHS-4 to 43% in NFHS-5. Reduction in the adolescent fertility rate also had an impact in the likeliness of continued education which was evidenced by an increase in the adolescent girl’s literacy level from 65% to 70% (2011 to 2021) and an increase in the female literacy rate from 80.35% in 2010 to 91.95% in 2021.12 The percentage of female enrolment in higher education has risen from 45% in 2014-15 to about 49% in 2020-21. This increase can also be associated with the increase in Gender Parity Index (GPI), which is the ratio of Gross enrollment ratio (GER) of female to male at both Secondary and Higher Secondary education. The GPI has been most pronounced at the higher secondary level, which has gone up to 1.04 in 2019-20 from 0.97 in 2012-13.38
Rashtriya Bal Swasthya Karyakram* (RBSK)* program39 involves screening of children from birth to 18 years of age for 4 Ds- Defects at birth for early detection, disability, deficiency and diseases and free treatment and management, with the assurance of a higher quality of life. The programme has led to improved educational opportunities, fewer school dropouts due to illness, and has contributed to improved social well-being of affected children.40 These benefits can be well correlated with the primary school enrollment rate, which increased from 94 to 103 (% gross) from 2000 to 2021 and the decrease in dropout rate at the primary level (Classes 1 to 5) to 1.5% in the academic year 2021-22, from 3.5% in 2015-16, after the launch of the scheme.41,42
Decrease in out-of-pocket expenditure (OOPE)
Janani Shishu Suraksha Karyakaram (JSSK)43 and JSY, both 100 % centrally sponsored schemes were launched with the objective of reducing maternal and neonatal mortality by promoting institutional delivery among poor pregnant women. This safe motherhood intervention entitles all pregnant women delivering in public health institutions to absolutely free and no expense delivery, including caesarean section, while JSY integrates cash assistance with delivery and post-delivery care. In the case of institutional deliveries, there was a significant reduction in high out-of-pocket expenses incurred by pregnant women and their families in the form of drugs, user fees, diagnostic tests, diet, and C-sections.
The total direct expenditure among non-JSY women was approximately 16 times that of JSY beneficiaries, total maternal expenditure among JSY beneficiaries worked out at about 8% of their annual household consumption expenditure, whereas among non-JSY women, it turned out to be much higher with about 28% of their annual household consumption expenditure. Average out-of-pocket expenditure per delivery in a public health facility declined from INR 3,197 (NFHS- 4) to INR 2,916 (NFHS-5). Share of JSY incentives on cost of antenatal and delivery care - After deducting JSY incentives, OOPE per delivery was estimated and government share accounts 44 % of OOPE per delivery, 77 % for normal delivery, 38 % for delivery that had complications during pregnancy or delivery and 23 % for those deliveries which had complications both during delivery and pregnancy. JSY incentives reduced the total cost by 47 % among Below Poverty Line (BPL) families and 32 % among Above Poverty Line (APL) families.44 The scheme has thus been successful in reducing the OOPE of the beneficiaries opting for delivery at public health facility. Since the incentive was the highlight of the scheme, the increase in institutional deliveries could be attributed to the satisfaction with the incentives attached to the scheme.45
Data show that only 6% of seniors over 60 are receiving pensions post retirement that can support their healthcare needs.46,47 National Programme for health care of elderly48 evidently supported economic independence of elderly to support the health care expenditure, such that healthcare services offered under the program helped the elderly to avoid financial hardships and reduced the OOPE. The program brought about a universal, accessible, and affordable long-term care service system with high-quality upstream prevention to postpone impairment and offer support services for family caregivers.49 An early analysis of the PM-JAY, the largest health assurance scheme in the world which aims at providing a health cover of INR 0.5 Million per family showed median OOPE in private hospitals for the PMJAY-enrolled as 17% lower than for those non-enrolled in PMJAY.50
Hospitalization-related costs and procedures accounted for most Non-Communicable Disease (NCD) care related OOPE.51 The National Programme for prevention and control of cancer, diabetes, cardiovascular diseases and stroke (now renamed as National NCD programme)52 evidently reduced the OOPE, such that private NCD patients had 3–5 times greater mean OOPE than public patients.53 NCD illness hospitalization led to 47% of households to catastrophic expenditure. Males had greater OOPE for all NCDs at INR 26,585.54 For all NCDs, private hospitals spent five times more (INR 39,466) than public ones (INR 7,905). Public facilities and beneficiary awareness are also associated with lowered OOPE.55
Tobacco quitting through the launch of National Tobacco Control Programme (NTCP)56 prevented indirect expenses of premature death, lost jobs, and family income and eventually improved the family’s socio-economic status.57,58 Global adult tobacco survey 1 and 2 showed the reduction in prevalence of tobacco use to 28.6% from 34.6%.59 Between 2004 and 2017, the national health care spending for premature deaths caused by smoking came down to 75% from 84% and smoking-related illnesses to 5.3% from 6.8%.60,61 Tobacco cessation initiatives, have also reduced healthcare and productivity expenditures, and many linked disorders as many studies have estimated years of potential life lost and productivity loss.62
Increase in manufacturing and agricultural productivity
As per the Economic Survey Reports 2022-23, average daily employment has increased by about 46% with the increase in estimated employment in Manufacturing Sector of India as; 5.7 crore in 2017-18, 6.12 crore in 2018-19 which further increased to 6.24 crore in 2019-20.44 The alternative viable opportunities created to tobacco farmers through NTCP boost agricultural production and cultivation which was evident by supporting economically viable alternative activities for tobacco farmers. The state of Andhra Pradesh found that paddy and Bengal gram are more profitable than tobacco. Kharif maize with low tillage of Rabi crops like red gram, chickpea, and horse gram could replace Flu Cured Virginia tobacco in Andhra Pradesh’s vertisols.63 The analysis on cost of production and returns of tobacco, paddy and Bengal gram crop cultivation in the selected villages reveal that the paddy (INR 8,985.78/Acre) and Bengal gram (INR 8,534.29/Acre) are more profitable crops than the tobacco (INR 7,151.1/Acre). Comparatively the tobacco crop cultivation also required more investment than paddy and Bengal gram.64
Improved access to drinking water
The National Programme for Prevention and Control of Fluorosis (NPPCF),65 aimed to prevent and control Fluorosis also improved provision of safe drinking water.66 Under NHM, Accredited Social Health Activist (ASHA) receive INR 75 for motivating Household for individual tap connections, Versatile Insurance Services in Well-equipped Accounting System (VISWAS) campaign and RKSK scheme with an objective to improve the overall quality of* *life of children and adolescents. The Jal Jeevan Mission (JJM)67 has contributed to access to safe drinking water, with 61.5% of the rural population in 2022 having access to safe and adequate drinking water compared to 40% in 2016.68
Conclusions
The second-order benefits of health that are covered in this report demonstrate the trickle-down economic effect of investing in health systems by creating high-quality jobs and acquiring goods and services from local businesses. These benefits are explored in relation to the first-order benefits of health. Not only do healthcare systems play an essential role in the economy of national and local communities through employment and the reduction of OOPE, but they also play a key role in the social lives of these communities through the employment of women, the promotion of gender equity, and the formation of local partnerships. Health systems can demonstrate their worth by having a net positive effect on the economy of their communities; thus we need to invest in health as there are benefits beyond good health and well-being.
Funding
We did not receive any funds for this study.
Authorship contributions
Delfin Lovelina Francis: Formal analysis, Methodology, Data curation, original draft preparation, Preparation of necessary format in software. Neha Dumka: Methodology, Arranging Resources, assisting in original draft preparation, Scientific Content Verification, Reviewing and Final Editing. Atul Kotwal: Conceptualization, Methodology, Formal analysis, Sequence of Ideas, Supervision, Reviewing and Final Editing. PK Dutta: Supervision, Reviewing and Final Editing.
Disclosure of interest
The authors completed the ICMJE Disclosure of Interest Form (available upon request from the corresponding author) and disclose no relevant interests.
Correspondence to
Atul Kotwal, Executive Director, National Health Systems Resource Centre, New Delhi, India. [email protected]