

The “rapid response mechanism” (RRM) is a model which was designed to facilitate multi-sectoral assistance, including health care services to those affected by complex emergencies and is used for timely response to vulnerable populations with sudden displacement. It has been utilized in responses when there is an absence of humanitarian presence or capacity on the ground. Some conflict settings where RRM has been used include Central Africa Republic, Nigeria, South Sudan and the Democratic Republic of Congo.1–3 The standard package comprises of a rapid multi-sector assessments within 72 hours of the emergency, followed by a multi-sector response of selected high impact interventions which often include water sanitation and hygiene assistance, household family relief, and primary education, health and nutrition interventions, alongside advocacy and coordination with other actors and monitoring of activities.1,2,4
The number of people in need of humanitarian assistance in 2022 was estimated to be 235 million – the highest recorded in decades.5 With increasing humanitarian crises from natural disasters and armed conflict, humanitarian needs might even rise further especially with conflicts that are becoming more protracted.5 This is true for communities affected by conflict in Cameroon6 where for the past seven years, the Northwest and Southwest (NWSW) regions of Cameroon have been experiencing armed conflict. This conflict started after peaceful protests and escalated following the burning of 200 villages and the internal displacement of above 900,000 people across the regions, with significant disruption to social services, including basic health care services.7,8 The violent nature of the conflict caused massive displacement of populations into the forest and/or more hard-to-reach locations.9 Accessing life-saving emergency assistance such as primary health care, nutrition, and water hygiene and sanitation was very difficult, motivating the rolling out of the Rapid Response Mechanism (RRM) for communities in hard-to-reach communities of Ekondo Titi.
In a bid to provide lifesaving interventions to displaced communities in hard-to-reach areas, a Rapid Response Mechanism intervention was implemented in Ekondo Titi district by Reach Out Cameroon as implementing partner. The goal of the RRM was to initiate and sustain lifesaving activities and alleviate suffering through an integrated and coordinated humanitarian response focusing on the most vulnerable.
We were directly involved in the implementation of the RRM intervention, and we witness first-hand the challenges and pitfalls of this intervention; especially around the delay in responding to the needs of affected communities. In this article we reflect on our experience and lessons learned for future rapid response mechanism interventions in humanitarian settings.
The case of Ekondo Titi
Ekondo Titi is a health district in Ndian Division of the Southwest Region of Cameroon which comprises nine health areas. Among these health areas, Illor, Bamusso, and Bekumu are predominantly located along the coast, while the remaining six health areas, namely Ekondo titi, Lobe, Bekora, Kumbe Balue, Bafaka Balue, and Bissoro are situated inland Geographically, the Ekondotiti health district encompasses a mix of terrain, including forested areas, hills, and small rivers. This diverse landscape poses unique challenges and opportunities for healthcare delivery. Ekondo Titi health district is bordered by five different health districts (Mundemba HD in the North, Mbonge HD in the South, Kumba HD in the East) and the Atlantic Ocean in the Southwest (figure 1). The closest accessible town to Ekondo Titi is Kumba (60 kilo meters). Other relatively accessible towns are Buea, Muyuka, Limbe, and Tiko.6,10 Ekondo Titi has always had seasonal roads even prior to the crisis. In the raining seasons the access was difficult with transportations cost going as high as $9 USD and took like three to seven hours to travel from Kumba to Ekondo Titi. In the dry season the roads were maintained regularly, and the transportation cost was at $5 USD and usually took an hour to get to Ekondo titi. Within Ekondo titi health district (HD), transportation is primarily using motor bikes to access 7/9 of the health areas and by boat to go to the maritime health areas (Bekumu and Bamusso).6
Pre-conflict, Ekondo Titi had a population of about 56,503 mostly farmers in the 7 mainland health areas and Fishing in the Maritime health areas. Recurrent conflict had made farming very difficult with many abandoning their farms for fear of their lives. Before the Crisis Ekondo Titi HD had thirteen fully functional health facilities as opposed to four by 2019.6 The educational sector has been severely impacted by the crises with school closures for almost six years. Many houses have been destroyed forcing populations to relocate to bushes, farmlands or other remote communities9,11
With the coming of the crisis, the road from Kumba to Ekondo titi received little maintenance and deteriorated to levels were travelling even during the dry season took at least four to five hours and costs at least 9 USD. Using the road in the raining season could take more than twenty four hours and cost up to 25 USD. This was made worse by frequent gun battles along the road with increased risk of kidnaping pushing the population and its visitors to opt for using the sea as the primary means of travelling to Ekondo Titi health district (HD) with a typical travel time of one to two hours from Idenau. Ekondo Titi is one of the districts highly affected by the armed conflict and with extremely bad roads, limited communication networks, limited access to electricity, low literacy levels and high presence of non-state armed groups.6,11

Core components of the RRM
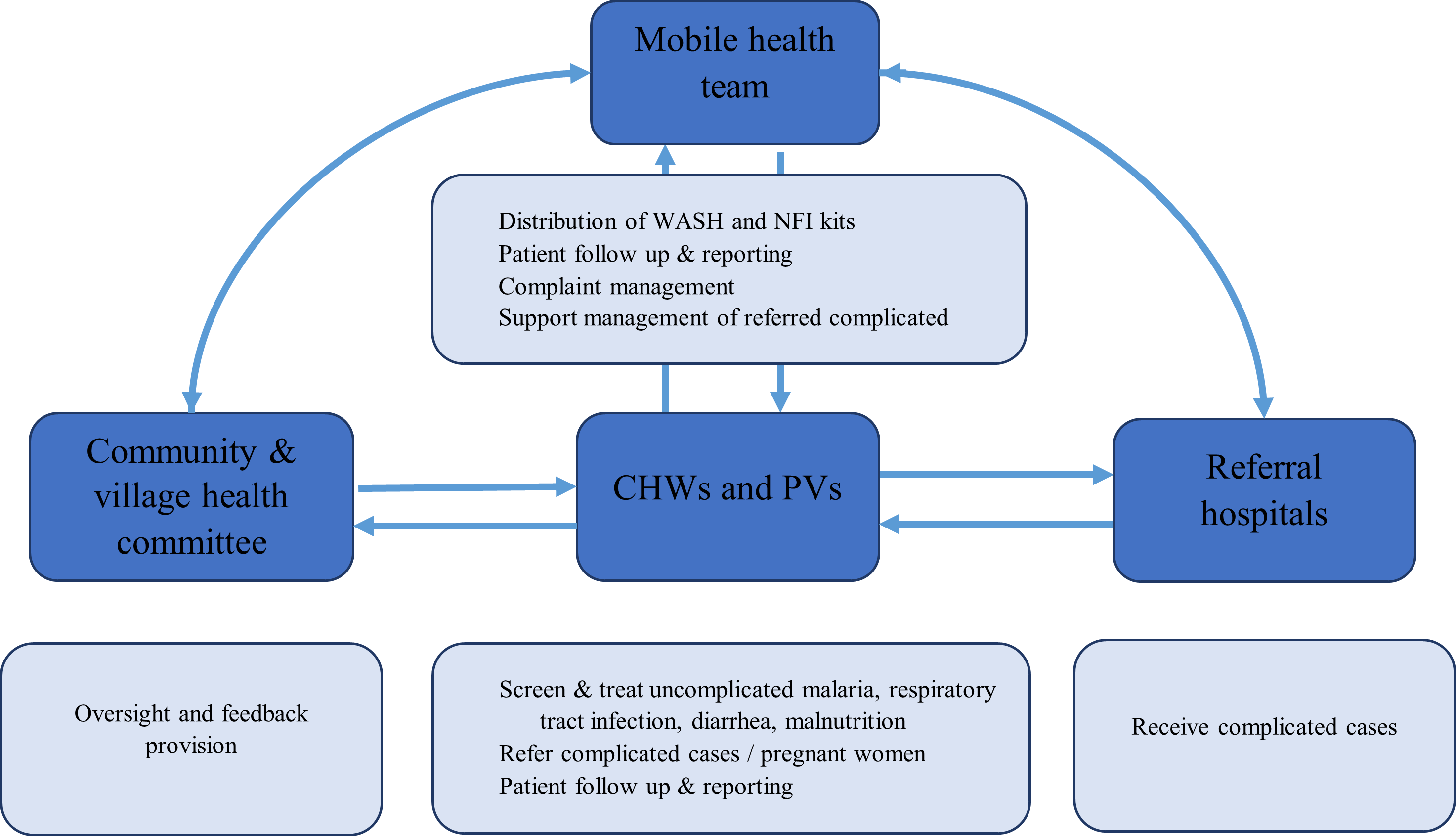
The RRM in Ekondo Titi was designed to provide critical, lifesaving and essential services to the most vulnerable internal displaced persons (IDP) and returnees in twenty extremely hard-to-reach communities who had received no form of assistance. The RRM had four main packages namely, essential health services, nutrition, Child protection, water hygiene and sanitation (WASH) including non-food items; thus, covering four humanitarian response sectors (Table 1). At the time of implementing the RRM, there was limited evidence-based information to guide the implementation of the RRM as an approach and is still the case to the best of our knowledge. Guidance on its implementation and programming was very much based on our past experiences in managing and implementing projects in hard-to-reach contexts and also from our experiences with large-scale distribution of NFIs and food in high-risk communities very early on in the crises in 2018. Our model (figure 3) included the use of community health workers, a mobile health team, child protection volunteers, village committees and referral hospitals.
Primary health care: The provision of primary health care services was based on the integrated community case management (ICCM) approach which included the treatment of acute respiratory infection (ARI), acute diarrhea, uncomplicated malaria and health education. Also, vitamin A supplementation and deworming services were provided to children. A community-based surveillance system was put in place to assist in the early identification, diagnosis and response to any potential outbreaks.6 Emergency delivery kits and maternal kits were provided to pregnant and lactating mothers respectively. Complex medical cases were referred to the Ekondo Titi district hospital. The intervention covered the cost of most referral medical cases especially for children. This was covered in the child protection arm of the intervention.
Nutrition: For nutrition services, all children six months to fifty-nine months of age were screened once every month for malnutrition using MUAC tapes and provided curative nutritional services to all children diagnosed with severe acute malnutrition (SAM) while nutritional education and counselling was provided to the care-givers of children diagnosed with moderate acute malnutrition (MAM). The curative treatment was done through outpatient community management of SAM by community health workers (CHWs) using Ready to Use Therapeutic Food for uncomplicated cases, while all complicated SAM cases were referred to the District Hospital. A mobile health team reviewed children managed in the community (Figure 2).

Non-food Items (NFIs) and WASH services included the provision of buckets, jerricans, Aqua tablets, long-lasting insecticidal nets (LLINs), blankets, and soap. Also, communities were provided with latrine digging kits and toilet flaps for the construction of latrines in their new settlements (mostly in the bushes). Community sensitization on basic hygiene and sanitation practices like water purification, use of latrine, hand washing, waste disposal was done by CHWs. Personal hygiene kits including reusable sanitary pads were provided for women 12- to 45 years old.
Child protection: The child protection package included the provision of basic psychosocial support to vulnerable children after identification, assessment and registration by protection volunteers and a child protection officer in charge of all protection volunteers. Since schools had been non-functional in most of the communities in which the RRM intervened, a key aspect of the child protection component was the creation of child friendly spaces which enable children to meet at an agreed location in the community for engagement with sports and art-like activities. These child-friendly spaces were animated by child protection volunteers where were members of the communities that were trained to run the spaces. The protection volunteers were also identifying separated and unaccompanied children to reunited them with family members or host families. They also identified vulnerable children with lost documentation, and in urgent need for financial support (Figure 3).

Multisectoral assessment: Prior to the start of RRM, no needs assessment was conducted partly due to high insecurity in Ekondo Titi compared to other districts in the region and also due to lack of trust for humanitarian organizations.6 Communities were selected based on population vulnerabilities following security assessment by the organization triangulated with data from the Ekondo Titi council development plan pre-conflict. Priority was given to internally displaced persons (IDPs) in new settlements, bushes/forests, communities with high levels of displacement, and communities hosting high numbers of IDPs.
Coordination and logistics of the RRM
Coordination of the RRM was mostly done at the head office and field office. The RRM had a project coordinator/manager dedicated to RRM. Safety/security staff were part of the RRM response team and worked closely with the project manager and mobile health team to ensure safety of the team and supplies. Weekly partners meetings were held between the project management team and the donor.
The mobile health team had a 4x4 pickup truck at their disposal to aid in transportation to various communities. All NFIs were transported from the donor’s main warehouse to Ebondo Titi warehouse using a 250 cubic meter capacity wooden boat (doing two trips by sea) and several 20 – 30 tons trucks. To our knowledge, this was the first humanitarian attempt at moving commodities of this capacity by sea to any district in the Southwest region using local sea transport boat (figure 2). Transportation of non-food items (NFIs) from the Ekondo Titi warehouse to beneficiary communities were by 4X4 pickups, 10 tons trucks and motor bikes.
DISCUSSION
Successes registered – contribution to the overall humanitarian response
A major contribution of this RRM was its support to the weakened health system through the provision of health services, nutrition services, WASH and child protection interventions. Community health workers (CHWs) and protection volunteers (PV) successfully treated a total of 2310 children for acute respiratory infection, 1882 persons treated against acute diarrhea, and 6482 persons treated for simple malaria. For nutrition program indicators, the CHWs screened 13,177 children aged 6 to 59 months, from which 43 were diagnosed with SAM without complications and placed on treatment by the CHWs. WASH and NFIs were provided to ten communities as this comprised the first service package in the RRM. 2000 families were provided with two LLINs each. In addition, 320 maternal care kits and 290 newborn kits were distributed to pregnant women and nursing mothers, respectively. Protection volunteers successfully identified 471 children needing social assistance. Forty-three of these children received cash support to cover their medical bills. Our RRM model aligned with other RRM models2,4,12 and its mobile health team operated similarly to previously described mobile clinics.13,14
Another success registered in the RRM was the response and containment of disease outbreaks in Ekondo-titi district. Due to the conflict, immunization and disease surveillance programs were weakened as a result of attacks on health care and burning of communities which caused populations to flee into bushes and/or more remote locations. The RRM response led to the establishment of a community-based surveillance program which identified and responded to measles, monkey pox, Buruli ulcer, cholera and meningitis outbreaks.6,11
The RRM in Ekondo-titi was the first humanitarian response of any sort in the district. The security risks that existed with regular gun battles between the state and non-state armed groups made it almost impenetrable to humanitarian actors.9 This in combination to the fact that the most vulnerable people had actually moved into bushes and established new settlements15 making it even more difficult to tract them for any assessment. However, three months into the RRM project, the project team had mapped out all new settlements and could track in real time new displacements and population movements through CHWs and protection volunteers. With better information on the number of IDPs, their exact locations and constant security update other humanitarian organizations began providing additional responses.
Challenges encountered
Unstable and poor telecommunication was one of the biggest challenges regularly faced throughout the RRM program. This affected the response negatively in several ways including, delaying weekly reporting to the head office, inability to communicate emergency field incidents due to prolong loss of signals, prompting the use of tradition forms of communication such as the sending of letters. Also, remote supervision of CHWs by the mobile health team was made difficult.
Poor roads affected field operations, as some communities were completely cut off during the rainy season, making distribution of NFI kits extremely difficult and in some cases impossible. Transportation of response staff from the head office to Ekondo-titi was by sea since the roads had become impassible due to poor roads coupled to frequent arm confrontations between the belligerents.
Administrative bottlenecks delayed implementation of the response and in some instances, got operations temporally suspended due to suspicion of providing humanitarian responses to non-state armed groups. For the entire duration of the response, staff suffered different high-risk security incidents from threats to their lives by some non-state armed groups, to community volunteers being victims of gunshot wounds during crossfire in their villages.
What could have been done differently?
The RRM was only implemented one year after the crises in the Northwest and Southwest Regions had been declared a humanitarian crisis following the massive displacement of people internally to bushes, other rural and urban communities and to neighboring Nigeria. The RRM was triggered, targeting IDPs that had been displaced for an average of six months (Appendix 1). While most RRMs have been triggered and implemented within three months and in some cases within 3 days,1,2 the RRM in Ekondo titi provided aid to populations who had been displaced for over a year. Though the intervention provided aid to communities that had received no form of assistance and were displaced to bushes, we believe an earlier response would have served a better purpose to the affected populations and met the goal of timely intervening to suddenly displaced communities with great vulnerability. Many factors could have contributed to this delay ranging from lack of funding, high insecurity, no prepositioned commodities, funder’s bureaucratic/cumbersome administrative processes, logistical changes in implementing such a response in a highly inaccessible area, and no emergency preparedness/response plan pre-conflict. In conflict-affected contexts, the need for rapid emergency responses for affected communities cannot be overemphasized in mitigating the impact on loss of lives. If an intervention ought to be named “rapid response mechanism”, shouldn’t there be mechanisms in place to ensure quicker activation of such a response? Also, shouldn’t there be simpler ways of quickly accessing funding and resources especially for local organizations. We think there is need to have systems that allow for quick and flexible access to funding with better financing/administrative processes from donors to local organizations to enable timely initiation of responses like the RRM.
We also think there is need for better coordination between sectoral partners to enable quicker response in situations of crises. From our experience with this RRM intervention, this response was shouldered entirely by one UN Agency with its implementing partners at the time it was initiated. A more inclusive process involving the participation of other humanitarian organizations from different sectors and mandates may have reduced the time it took to initiate the RRM intervention. Coordination with other partners may also allow for such interventions to be rolled out in many more communities. To the best of our knowledge, at the time this intervention was implemented, only one district (Ekondo titi) was covered with this approach. More districts could have been covered, if the coordination with the other humanitarian partners was better, to inform on how collectively we could leverage on using a multisector approach to reach other districts simultaneously. The impact of such a collectively response would have outweighed the great results recorded with the RRM in Ekondo titi and many more lives would have been saved in other districts across the Northwest and Southwest Regions.
Further, the package of services delivered by the RRM in Ekondo titi was very similar to that offered in South Sudan covering major sectors providing NFIs to families, water purification tablets, and basic healthcare.12 The South Sudan, DRC, and Diffa RRMs had food distributions as the main package, which wasn’t part of the package of the RRM in Ekondo titi.1,12 Like the Yemen RRM, that of Ekondo-titi also provided dignity, hygiene kits.16 The multisector approached used in the RRM allows for social and economic needs of conflict-affected populations to be addressed. Unlike most RRM interventions, that of Ekondo titi was more primary health care intensive. This might have been because most health facilities in the North West and South West regions were closed.6 We think harmonizing the benefit packages for RRM interventions in general (with primary health care being systematically included) might set the foundation to prepare and respond better in future emergencies.
Conclusions
An emergency intervention like the RRM provides opportunities to meet the health needs of affected communities from a multisector lens. However, the timely initiation of such a response is important in meeting the goal of saving lives. It is important for humanitarian organizations to jointly coordinate RRMs and for benefit packages to be harmonized.
Acknowledgements
We acknowledge and recognise UNICEF for funding the RRM program. We also acknowledge RRM colleagues, and community health workers/ volunteers who gave so much of themselves to save lives in Ekondo Titi. We appreciate Elizabeth Jarman for developing the illustration in Figure 3, used in this paper. We thank the affected communities for accepting the intervention and collaborating with the project team.
Funding
No funding was received for this publication.
Authors’ contributions
LAO and MA conceived, prepared the manuscript, and made pertinent revisions to the paper for significant intellectual content. All authors read and approved of the final manuscript.
Disclosure of interest
The authors completed the Unified Competing Interest form at http://www.icmje.org/disclosure-of-interest/ (available upon request from the corresponding author), and declare no conflicts of interest.