The first Coronavirus Disease 2019 (COVID-19) case in Nepal was confirmed on 23 January 2020 and was identified as a person returning to Nepal from Wuhan.1 The Nepalese government implemented stay-home policies from 24 March to 21 July 2020.2 The first COVID-19 death was reported on 16 May 2020 as a 27-year-old postpartum woman.3 Frontline health workers and people aged >60 years were prioritised for the first vaccine campaign conducted on 27 January 2021. The incidence of cases with the delta variant increased in April 2021 after people from Nepal began participating in a religious gathering called Kumbha Mela in India.4 Gradually COVID-19 cases increased in Nepal, creating a state of health emergency. Due to its limited infrastructure, Nepal faced a scarcity of hospital beds, intensive care units, oxygen supplies, and personal protective equipment (PPE), among other resources.5,6
Multiple health sectors were affected due to the COVID-19 pandemic. Notably, maternal mortality was substantially increased during the lockdown, and immunisation was stopped in most parts of the country. Patients involved in other medical sectors, such as patients with cancer, Outpatient Department (OPD) patients, dialysis patients, and patients with tuberculosis, were unable to receive their required services. Moreover, the programmes directed towards decreasing the Maternal Mortality Rate (MMR) were severely halted, resulting in a decrease in hospital and preterm deliveries and an increase in the MMR, neonatal mortality rate, and maternal complications following deliveries during the pandemic.
To date, no paper has investigated both maternal and neonatal mortality and the routine national immunisation of children during the COVID-19 pandemic in Nepal. A considerable number of articles have been published from other countries depicting their situation of maternity services during the pandemic. Thus, this review article intends to provide a summary of maternal and child health and the Child Regular National Immunisation Programme during the pandemic in Nepal.
METHODS
Objectives
The objective of this study is to determine the effects of COVID-19 on the utilisation of maternity services and the status of child immunization during the pandemic in Nepal and identify the factors responsible for these effects. Specifically, the study aims to summarize existing articles to gain a clear view of maternal mortality and child immunisation in Nepal during the COVID-19 pandemic.
Literature search
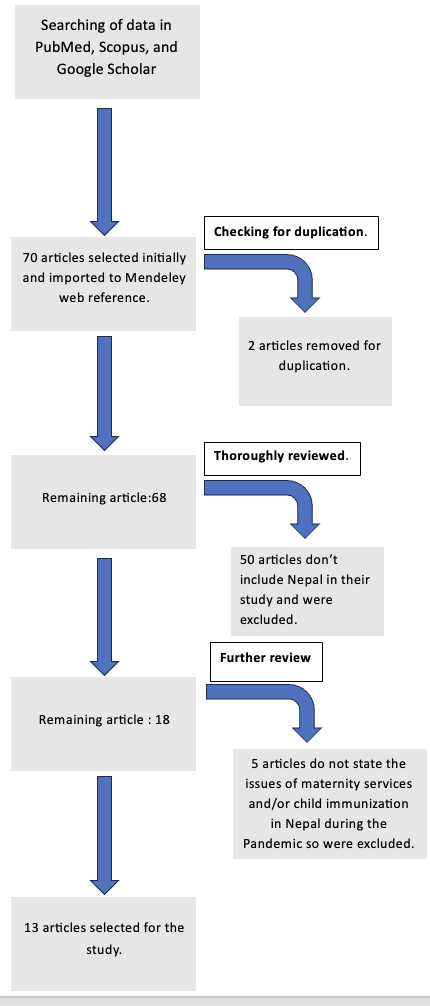
A comprehensive literature search was conducted to identify relevant articles. The following databases were used: PubMed, Scopus, and Google Scholar. The search terms employed were “maternal mortality in Nepal during COVID-19”, “maternity service utilisation in Nepal during COVID-19”, and “child immunisation in Nepal during COVID-19”. The search was limited to articles published between 2019 and 2022, research conducted in Nepal, and articles that included maternal mortality, utilisation of maternity services, and child immunisation in the title of the full text.
Seventy articles were found during the search, of which 13 articles were selected. Fifty articles were excluded as they were not related to the study report of Nepal. Additionally, 5 articles did not evaluate the MMR and hospital service utilisation in Nepal, so they were excluded. Two articles were also excluded due to their low sample size. Therefore, a total of 13 articles, which studied MMR, hospital service utilisation, and immunisation status during the COVID-19 pandemic in Nepal, were included. These studies were conducted in tertiary centres or depicted in various states of Nepal.
Study selection
The articles selected for inclusion in this review were those that examined the impact of the COVID-19 pandemic on maternity services in Nepal. Both retrospective and prospective studies were included, provided they were conducted in tertiary centres and evaluated the results. The inclusion criteria ensured that the article investigated maternal mortality, utilisation of maternity services, and child immunisation during the pandemic in Nepal.

Data collection
Data for this study were collected from the hospital database of the selected tertiary centres. Information pertaining to maternal mortality, utilisation of maternity services, and child immunisation was extracted. The collected data were then compared with the data available on the official website of the Ministry of Health of Nepal to verify the findings.
RESULTS
Maternal and neonatal health
Nepal has made progress in reaching Sustainable Development Goal 3 (SDG3, 2015-2030); the child and neonatal mortality rates have decreased, and institutional deliveries have increased over time.7 The MMR for the year 2016 was 239 per 100,000 live births (decreased by 19 from the previous year).7 The goal set by the government of Nepal is to reduce the MMR to <70 per 100,000 live births by 2030. According to the Family Welfare Division of the Department of Health Services of Nepal, 153 women died because of pregnancy and childbirth between the implementation of pandemic stay-home policies (March 2021 to September 2021), while only 104 deaths were recorded during the same duration in the previous year before the pandemic.8 Several factors are responsible for the increased MMR during the stay-home policies in Nepal.
The institutional delivery rate has increased continuously in Nepal for the past 5 years but did not significantly increase in 2020, probably due to the significant decrease in institutional deliveries during the COVID-19 lockdown months9 (Table 1). Antenatal care (ANC) visits proposed by the Nepalese government decreased by 25.6% in July and 32.4% in August 2020 during the stay-home policies compared to the same months of the previous year. The United Nations Population Fund (UNFPA) in 2020 reported decreased use of sexual and reproductive health during the pandemic period in Nepal. Failure to use the institutional services by pregnant mothers was strongly associated with poor maternal and neonatal health outcomes.10
Similarly, Table 2 outlines a prospective observational study by Ashish et al. from January to May 2020. The study compared the intrapartum care and related parameters 12.5 weeks before the COVID-19 lockdown and during 9.5 weeks of the lockdown in nine hospitals across all seven provinces of Nepal (11.2% of total births in Nepal occurred in these hospitals in 201911).
The study findings suggest that while institutional birth decreased during the COVID-19 stay-home policies, stillbirth and preterm deliveries increased over this time, with an increase in the complicated pregnancy hospital admission ratio.12
The government of Nepal usually distributes misoprostol directly to pregnant mothers to prevent postpartum haemorrhage in the eighth month of pregnancy through the Matri Surakshya Chakki (MSC) programme. However, this programme was halted during the pandemic. Consequently, the Nepalese government reported that a major cause of maternal mortality during the pandemic was postpartum haemorrhage.13 Similarly, several other factors like the closure of transportation, closure of maternal health services in a substantial number of places, mothers’ fear of COVID transmission, decreased midwifery services, decreased ANC visits, and increased domestic violence, among others, were considered to explain the increased MMR during the pandemic period.14
Child immunisation programme
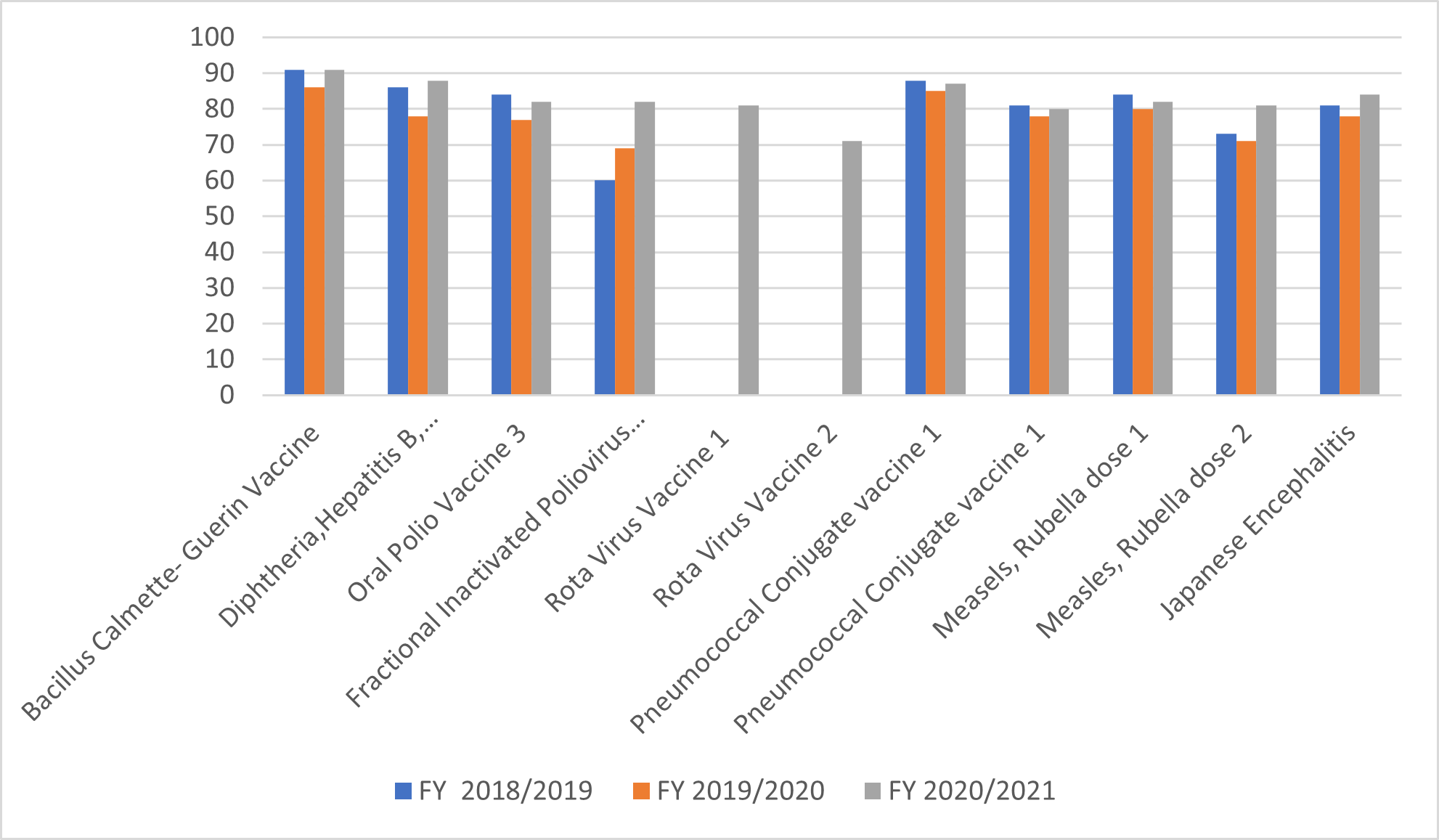
Childhood immunisation through the National Immunisation Programme is one of the main priorities of the government of Nepal, under which it supplies 13 types of vaccines against a range of diseases, including measles-rubella, pneumonia, tuberculosis, diphtheria, pertussis, tetanus, hepatitis B, rotavirus, Japanese encephalitis, and typhoid.15 National routine immunisation coverage from 2018/2019 to 2020/2021 is charted in Figure 1. Among the targeted population of <1 year of age, 620,258 patients were immunised.9
_in_nepal_before_and_after_the_pandemic.png)
As of September 2022, 95.7% of Nepal’s population is vaccinated against COVID-19. Through UNICEF, the WHO, and other partners, Nepal is gradually getting back on track for immunisation against childhood diseases other than COVID-19.16
During the 2020 COVID-19 pandemic, outbreaks of measles occurred in villages of Nepal’s Dhading and Gorkha districts because parents were unable to immunise their children.17 Moreover, 50% of the immunisation centres ceased operations during the first wave in 2020. In total, 220 measles cases occurred between February to March in eight districts; the district of Dhading had the highest number, with 138 cases, during the lockdown period in Nepal. The number of measles cases according to the district and outbreak period in Nepal is tabulated in Table 3.
DISCUSSION
This study aimed to identify and raise awareness about the extent of the secondary impact of the COVID-19 lockdown on maternal and neonatal health and the child routine immunisation campaign in Nepal, as well as to provide possible measures to reduce such disasters in future pandemics. This article attempts to interpret the true reasons for the pandemic’s negative effect on maternal and child health as follows.
Failure of service utilisation
Public transportation services were closed during the nationwide lockdown, which limited patients’ ability to reach health services. Emergency ambulance services were also closed (17-80%) for the first few weeks of lockdown due to fear of contamination.8 Fear of transmission to pregnant women also led to the decreased utilisation of available services. Increased domestic violence during the pandemic, which remained an issue both globally and in Nepal,19 affected women’s access to institutional services.
Closure of services
There were fewer ANC visits during the lockdown periods. According to governmental data, 25-80% of referral centres closed their ANC service for several days.8 Maternity services were closed in remote settings (36–80%), and emergency medications and drugs necessary for delivery were out of stock (20–100%). Over 50% of birthing centres (BCs) and basic emergency obstetric and neonatal care (BEONC) facilities were closed for delivery services.8 Nepal is highly dependent on midwifery services in its remote areas.20 The decreased activities of midwives during the lockdown halted the MSC programme initiated by the government to decrease MMR and maternal morbidity. Within the MSC programme, three 600 mcg misoprostol tablets are provided to women at 8 months of pregnancy by a Female Community Health Volunteer (FCHV). This programme is targeted towards pregnant women who are in remote areas and might deliver at home. The tablets are to be taken orally just after the delivery of the baby but before the placenta expulsion with proper counselling.21 After its implementation in 2009, MSC was found to be effective in reducing the incidence of postpartum haemorrhage.22 However, halting the programme due to the pandemic contributed to the increase in MMR, as a major cause of maternal mortality during the lockdown was postpartum haemorrhage.9,23
Globally, decreased utilisation of available services and closure of maternity services were reported during the COVID-19 pandemic.24 Communication with the pregnant mother via telephone to dispel misinformation, provide reliable information, and remind the patient about ANC visits was adopted by many African countries as a measure of service continuity and received a positive response.25,26 An international non-governmental organisation, Partners in Health (PIH), worked in several low- and middle-income countries (LMICs) to combat the fall in maternity services during the pandemic.27 PIH mainly worked by increasing the workforce, training midwives, training local female healthcare workers, delivering communication campaigns, supplying medical equipment, making new guidelines for treatment, and providing PPE to health workers in coordination with the local and central governments of LMICs. Due to these actions, many positive changes were seen in maternity services.28
The Safe Motherhood Programme of Nepal can provide easy ambulance access for mothers in remote areas and health services to improve institutional delivery rate. The Aama and the Newborn Programme, introduced in 2007, can also be encouraged to distribute medicines and supplements like iron, calcium, misoprostol, and folic acid door to door. Moreover, upgrading maternity service facilities in local and primary healthcare centres can also decrease the MMR. To ensure safe deliveries and evaluate maternal mortality risk, the FCHVs can be trained and encouraged to work in adverse conditions. To prevent maternal and neonatal infections, delivery rooms can be isolated for safe deliveries and neonatal care. During future pandemics, it is necessary to set up different guidelines targeting the specific region and patient population in coordination with national and international health organisations like the WHO, UNICEF, UNESCO, and UNDP. Existing guidelines in geographically different areas may not be as effective.29
Transportation, as the most affected sector, and the closure of health services greatly impacted public health during the COVID-19 pandemic. Public transport should be continued while implementing stay-home policies, minimising the transmission of infection by using sanitisers, distancing in the vehicle, and urging the public not to use public transport unless for medical or emergency reasons. Targeted patient-specific public vehicles can be managed by the local government so that it is easy for patients to visit the hospital. The government of Nepal should make it a priority to build an oxygen plant in hospitals, resulting in an independent oxygen supply. Separating COVID and non-COVID patient wards with adequate infrastructures and, if possible, dividing the healthcare workers dealing with the COVID and non-COVID patients could also yield the best services without resulting in their closure.
The national immunisation programme may promote itself by providing services during the pandemic by recruiting an efficient workforce in remote areas. Safety assurance of the vaccination staff, protective equipment against COVID-19 transmission, maintaining reliable data of missed immunisations, and addressing these missed doses should be performed during future pandemics.30 Immunisation registration is necessary for catching up on missed immunisations in children according to their age group.
CONCLUSIONS
There have been many issues during the implementation of stay-home policies due to the pandemic in Nepal. It has been noticed that Nepal lacks the basic infrastructure for fighting against the pandemic. The pandemic severely impacted maternity services and the child immunisation programme, though child immunisation recovered within 3 months after the lockdown. Serious concerns from the government and helping organisations like the WHO and UNICEF in Nepal should be considered to reduce loss in future pandemics.
Funding
None
Authorship contributions
SG wrote the manuscript. DB, CY, TZ and MT contributed to conception and design of the study. All authors contributed to critical revision of the paper and approved the final manuscript.
Competing interests
The authors completed the ICMJE Declaration of Interest Form (available upon request from the corresponding author) and declare no conflicts of interest.
{kind=link}