The ongoing armed conflict in the English-speaking Northwest and Southwest regions of Cameroon, referred to as the “Anglophone crisis”, can be traced back to 1961 when the country as we know it today was formed by the unification of the British and French territories.1–3 Since then, the differences between the co-existing British and French systems of education, law, policy, and general schools of thought have been a constant argument, which developed into a violent protest in 2016 and later progressed into an armed conflict in 2017.1 This human-made humanitarian crisis, as with any armed conflict, has led to the loss of lives and property, internal displacements of the population from remote villages to major cities and out of the region, a disruption of the healthcare and educational systems, and a deterioration of the conditions of living and well-being of the populations affected. Since the onset of the Anglophone crisis in these two regions, 1 million people have been internally displaced and approximately 74,000 of them have sought refuge in neighboring Nigeria.4 According to United Nations Office for the Coordination of Humanitarian Affairs (OCHA, 2022), 80% of schools and health facilities are non-functional, approximately 3000 people have lost their lives, and nearly 4 million people need humanitarian aid.4
In the context of a humanitarian crises, especially due to armed conflict, there is usually increased vulnerability to poor sexual and reproductive health (SRH) outcomes.5 These include unwanted pregnancies, unsafe abortions, maternal death, rape and gender-based violence resulting from reduced access to SRH services and supplies, weakened health systems, depleted human resources, increased exposure to sexual violence, and increased impoverishment and related risk-taking.6 These unmet SRH needs and risk factors are particularly evident among youth who are displaced or idle as a result of the crises.7–9
Adolescents and youth, defined by the World Health Organization (WHO) as individuals aged 10 to 19 years and 15 to 24 years, respectively,10 constitute a vulnerable population with unique and specific health needs that have been receiving increasing attention in recent decades.11 In transition from childhood to adulthood, youth are in a stage of rapid physical, cognitive, social, and emotional development,12 and this development process results in new behaviors that can affect short and long-term health outcomes,13 especially their sexual and reproductive health. Young people often have difficulties in accessing health care services due to a lack of knowledge about health and health services, the inability to travel to access these services, restrictive laws and judgmental attitudes of health care workers,14–16 and lack of privacy and confidentiality coupled with a greater fear of embarrassment and being perceived negatively by parents and others.15 These factors place youth at increased risk of poor SRH outcomes, creating the need for youth-responsive health care services and interventions. In conflict zones, youth’s sexual and reproductive health has been shown to be particularly affected. A recent review17 of studies in Africa found that knowledge about, access to, and availability of SHR services among displaced refugee girls and young women was limited. Youth affected by conflicts and other humanitarian crises are also vulnerable to sexual violence and associated consequences of psychological trauma, sexually transmitted diseases, unplanned pregnancy, and unsafe abortions.5,17–19
In Cameroon, general observations and media reports indicate that the crisis has had a significantly negative impact on the health of the populations in these regions, especially among vulnerable groups such as women, children, and adolescents. As with many conflict zones in Africa, there is very limited data on the overall impact of the crisis on the sexual and reproductive health of adolescents and youth in conflict-affected regions.17 Therefore, there is a need to raise awareness on SRH risks associated with regions with armed conflicts and to provide more evidence for the development of interventions and policies to improve adolescent and youth SRH.
Organizations such as Youth-2-Youth have been working to identify and address the sexual and reproductive needs of youth in the northwest region of Cameroon. To obtain baseline data, this organization conducted qualitative group interviews and forums, and administered a survey to understand the overall effect of the crisis on the sexual and reproductive health outcomes of adolescents and youth through a community centered approach. This paper presents the findings from the analysis of those data with the aims of: (1) describing the effects of the crisis on adolescent sexual and reproductive health; and (2) identifying stakeholder recommendations for strategies to address the SRH of youth in their crisis-impacted communities.
METHODS
Design and setting
This study involved analysis of data obtained through a multiple-methods study with quantitative and qualitative arms, conducted by the organization Youth-2-Youth Cameroon, a youth-led organization in the Bamenda, Northwest region, Cameroon, under their Adolescent SRH Project from May to July 2020. The data were collected as part of a community-based advocacy family planning project that sought to evaluate the impact of the ongoing crisis on the SRH and wellbeing of adolescents, assess community perspectives on adolescent’s use of contraceptives, and identify urgent health needs in the community and propose appropriate solutions. This project began with a community action cycle approach,20 a model that promotes individual and collective actions to address health program goals and related outcomes. The design consisted of organizing community discussion forums with the following community stakeholder groups: Parents, Youths, Religious leaders, Neighborhood leaders, Secondary school teachers, Health professionals, Pharmacists, local drug vendors, Media representatives, and NGO representatives. During the forums, participants completed a questionnaire and participated in a discussion on youth SRH, specifically knowledge, perceptions, availability of and access to resources, and recommendations for next steps for addressing the gaps identified.
Sampling and recruitment processes
Stakeholders were approached and invited to participate in the project by Youth-2-youth community engagement officers. A representative number of participants were invited from the three subdivisions in Bamenda. A purposive sampling was initiated, focusing specifically on the recruitment of individuals from the various stakeholder groups.21 Within each group, convenience and snowball recruitment technique were used.22 Each of the 316 individuals recruited participated in one of 12 forums held. Separate sessions were conducted for each of the 10 stakeholder groups. At each session, participants were also asked to complete a survey. Table 1 presents the distribution of participants per forum and stakeholder group, and the surveys completed. All participants resided in Bamenda, Northwest Region of Cameroon, since the onset of the crisis.
Data collection processes
The discussions were led by two researchers (MB, JK) with experience in SRH. Prior to the sessions with each stakeholder group, an anonymous survey comprised of 16 questions was administered to obtain general demographic information (age, region of residence, profession, and level of education) and assess the participants’ knowledge and perceptions on family planning and contraceptive use. Discussions were semi-structured, including questions about predefined topics related to the impact of the crisis on adolescent SRH, urgent health needs, and proposed solutions to identified needs. Each discussion session was conducted in English and Pidgin English and recorded using an audio recorder with the consent of all attendees, and detailed notes were also taken to capture key points raised by the participants.
Data analysis
The analyses for this paper are focused on the qualitative data from the forums (survey data are presented elsewhere). The community discussion forum data was uploaded into Dedoose (Version 8.3.47, 2020) qualitative data management software and analyzed using conventional content analysis for inductive category development,23 wherein three coders read the transcripts repeatedly and independently to derive codes, discussed discrepancies of the emerged codes, and resolved any disagreements. Moreover, codes were grouped into categories, which were then used to identify key themes and patterns. Coding and interpretation of data was conducted collaboratively with members of the Youth-2-Youth team (JF, JN) and researchers from the University of Yaoundé 1 [MB] and the University of Rochester (AA, AG).
Ethical considerations
Ethical approval was obtained from the Northwest Regional Ethics Committee for Research Involving Human Subjects, Cameroon, and the University of Rochester Research Subjects Review Board.
RESULTS
A total of 316 stakeholders participated in the discussion forums, consisting of groups of 5 to 41 participants (Table 1). Of these, 54.5% were female and 53.2% were married. Most of the participants were aged between 25 and 35 years (43.5%) and had completed or were currently completing a university education (66.5%). The ages of the participants ranged from 12 to 73 years (Table 2).
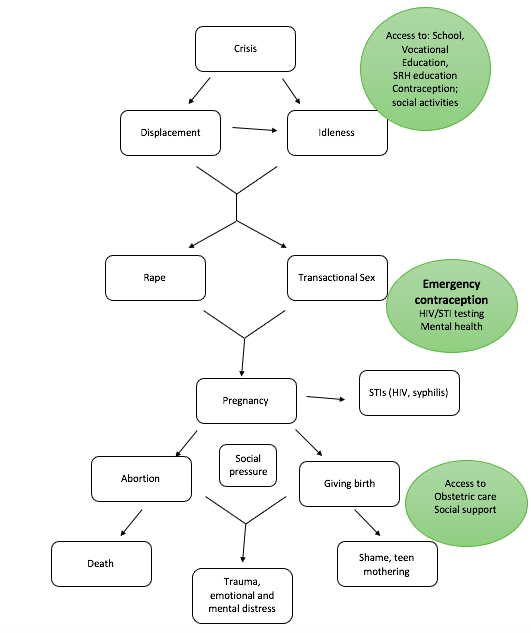
Several themes and sequential patterns emerged from the forums. First, the crisis led to the displacement of youth and idleness. These social and economic situations made the youth more vulnerable to sexual violence and forced them into transactional sex, which resulted in unplanned and precocious pregnancy and sexually transmitted diseases. Pressured by social norms, pregnant youth were either influenced to have the baby or forced to terminate the pregnancy. Consequences included cases of death during childbirth, unsafe abortion (given that abortion is illegal in Cameroon), or the socially derived shame and burden of mothering out of wedlock in a region of crisis, all of which were traumatic and led to emotional and mental distress (Figure 1).

Secondly, the need to assist these youth was highlighted in the stakeholders’ group forums. The main themes discussed in all the forums were spreading information about SRH and rights (SRHR), providing services for SRHR, and addressing issues of idleness and parental negligence.
Effects of the crisis on youth
Displacement as a result of the Anglophone Crisis most often was from a village or a city to a major city and settling with a host family. The most common destination was Bamenda, but there were cases where youth resettled in Yaoundé, the capital city of Cameroon. Many adolescents chose to flee the dangers of their communities and to seek refuge in cities. However, the majority was urged or forced to leave by parents (whether natal or host) concerned about the youth’s safety. A few female adolescents who had become pregnant were forced out of their communities following parents’ anger or rejection.
Whether they were displaced or still living in the crisis zone, idleness was prevalent among the youth. Most schools in the crisis region were closed, and those who left their communities dropped out of schools. A schoolteacher explained:
“So, when this crisis began, those students had to drop… wait for some time, were thinking that this crisis will stop and then school will begin again. After that, they became frustrated, the crisis was going on.” - Schoolteacher
There were two main consequences of displacement and idleness associated with the crisis: transactional sex and sexual violence. There was a co-occurrence between transactional sex and displacement, which included cases of girls officially designated as Internally displaced youth (IDY) as well as those reporting having been ousted from their family’s home. Engagement in transactional sex was economic, with influences from peers (‘bad friends’) and often from family members who encouraged or forced their adolescents into the sex trade to support the family. An NGO staff reported that:
“They had to give out to have a means of survival. So, these means of survival, that’s our interest now: what has the crisis done to adolescents? The crisis has pushed them to prostitution, and what are the consequences of prostitution? It’s rapes, STIs, HIV and AIDS, abortions, unwanted pregnancies…” - NGO staff
Moreover, a youth reported that
“University students who come to school and can’t go for holidays due to the insecurity in the villages. Thus, they are forced to stay in their hostels and with time when they ran out of resources, they get into transactional sex as a means for survival.” - Youth
Indeed, transactional sex had significant physical and emotional consequences on the adolescents. Sexual violence, specifically rape, occurred more often among displaced youth. Participants described cases of girls stranded on the streets after being sexually assaulted. There were 72 cases of rape described in the youth and community forums (Table 3). The most cited perpetrators were military or unspecified armed groups or militia. There were some reports of incest, primarily male members of host families raping IDY, and some cases of rape by other youth (< 18 years old).
There were some noteworthy commonalities about the instances of sexual violence described. The majority of victims whose age was known/specified was teenagers (13–19 years old). There were nine reported instances of victims aged 20 to 24 years, five instances of victims who were 10 to 13 years old, and seven were younger than 10 years old. A common thread across the stories of sexual violence was that rape was not always taken seriously and/or often not addressed in their communities. Even mothers of many of the victimized adolescents, for example, were described as having been dismissive of their daughters’ grievances and reports of being raped. The legal system in this crisis zone did not follow-up on the few instances actually reported officially. In sum, there were no consequences for the perpetrator and no assistance for the victimized adolescent.
Sexual violence and transactional led to many unplanned pregnancies, leaving adolescent females faced with illegally ending the pregnancy or having a child to care for in an already dire situation. The outcome depended on the amount of social support from family, friends and/or the man responsible for the pregnancy. Those who kept their pregnancy most often had some form of social support to assist with the responsibility of caring for a child, in many cases friends, a mother or other relative, and sometimes from the man responsible for the pregnancy. The youth and community members described emotional consequences of having a child, namely the burden of a youth caring for a child in an already difficult environment, and, in some cases (e.g., rape), the adolescent’s resentment towards the infant.
Having an abortion was often the result of the girl recognizing that she could not care for the infant, that she would have to face the shame of pregnancy at a young age and outside a committed relationship (e.g., marriage), and/or pressure from her entourage to end the pregnancy. In some cases, pressure to abort came from family members who did not want the shame and/or the responsibility of helping raise a child. A youth reported that:
“for fear of family rejection, she went for abortion after having gotten pregnant from transactional sex.” - Youth
Informants described multiple instances when family members (natal or host) pressured the girls to have an abortion, or, out of anger, forced them out of the family home. The girls would find themselves having to terminate a pregnancy in a new environment, without support.
For other girls, having an abortion was a response to threats from clients who did not want the responsibility of being a father, or from the perpetrators who did not want any evidence of their sexual abuse. Several girls reported having abortions on a regular basis. Becoming pregnant, terminating the pregnancy or having a child were largely not the choice of the girl. NGO staff described their encounter with these adolescents who felt shame and grief from being sexually abused yet felt they had no way or space to express their pain.
“The teenage girls, they are not able to communicate whether they are being raped or sexually violated because people don’t understand them, and so they tend to shy away. It’s very difficult to get any information, they hide information.” - NGO stakeholder
Regardless of the cause (forced, transactional or consensual sex) or the outcome of the pregnancy (giving birth or aborting), a range of psychosocial and biological health consequences were described. Health providers and youth described recurring infections, trauma, and distress resulting from sexual abuse, abortion or birthing. One known case of abortion led to the death of the pregnant adolescent. HIV and syphilis were two infections identified during the discussions. Trauma was reportedly severe, with cases of adolescents having suicidal thoughts and/or thoughts of infanticide. For example, some victimized adolescents reported feeling so distressed towards their infant that they thought about starving them to death or abandoning them on the side of the road. Emotional distress was fuelled by the shame from being violated, becoming pregnant and having to face rejection from family, and not being able to share their plight.
Stakeholder recommendations and proposed strategies
Stakeholders provided several recommendations for addressing adolescent SRH in the region, from preventing sexual violence and its consequences from occurring in the first plan, intervening immediately after victimization, and intervening on long-term consequences like pregnancy or sexually transmitted diseases. The recommendations are directed towards the youth (including those who have become parents), their parents, and the communities (Table 4 and Figure 1).
The community stakeholders interviewed recognized the strong link between the crisis, idleness, and sexual violence. Idleness resulted from poverty and was exacerbated by displacement and the lack of social support. Recommendations were to ensure that interventions are directed specifically to the socio-economic conditions that make sexual violence possible and transactional sex seems necessary. Therefore, a key theme in many of the solutions proposed to address idleness involved developing a strong social support for the youth. For example, taking advantage of traditional networks like njangi groups can help youth connectedness and can be a source of financial and psychosocial support. Njangi is a group of peers who meet during weekends for relaxation, to share a common meal, drink, sing and dance, contribute money to support one another through thrifts and loans or offer social support in case of birth, death, or a promotion. These natural groups could be leveraged for the promotion of SRH.
Other recommendations included raising awareness of and access to SRH services through social programs, such as sporting activities, skill-building workshops, health clubs in schools, and social digital forums. Health clubs, for example, can serve a medium of providing comprehensive education on SRH. Health clubs in Cameroon are student-led groups in secondary schools that focus on raising awareness on health-related topic and carrying out health promotion activities to benefit other students. In addition to being channels for improving SRH, these social activities could further develop youth’s interpersonal networks and occupy them, reducing idleness and chances of falling victim to or committing sexual violence.
Participants found it important that youth be well informed about SRH services. Youth should be aware of the different contraceptive methods, and SRH services should be made readily available on an ongoing basis as well as in emergency situations resulting from sexual victimization, for example. Knowledge of what is available and where it can be accessed is key for those seeking SRH services including contraception, emergency contraception, testing for STIs, and perinatal care. It is also important that SRH care providers engage with their surrounding community, building relationships in order to reduce hesitancy in seeking treatment. Engagement could entail making their services particularly welcoming to adolescents and developing good relationships with community-based health workers. This is particularly important for displaced individuals for whom finding social connections and health services is critical.
Finally, the community members recommended that the long-term trauma and emotional effects of sexual victimization be addressed as a community through grassroots and faith-based organizations, in addition to health care institutions’ services.
DISCUSSION
Displacement and idleness resulting from disruptions in school, economic and legal systems, and insecurity from the Anglophone crisis in Cameroon have created the unfortunately ideal situation for increased sexual violence, transactional sex and related physical and psychosocial consequences. These themes have been identified in multiple studies from conflict-zones in Africa and beyond. A study conducted among post-conflict communities in eastern Uganda reported that idleness was prevalent among displaced persons in IDP camps.24 Abera et al. (2021) discuss the high rates of sexual abuse among high school girls in Dire Dawa, Ethiopia, resulting from factors like being geographically far from their parents.25 The health consequences of rape among the high school-aged adolescents victimized included unplanned pregnancy, STIs, and abortion.
Few studies have explored idleness with respect to conflict and sexual violence. Logie et al. (2021) is one such study that found that frustration from being in a dire situation resulted in inactivity and idleness among young persons, creating an environment prone to violence and displacement.26 Another important point from their study is that power dynamics between host family and vulnerable internally displaced persons (IDP) further exacerbated idleness-related violence. In our study, forum participants also explained the vulnerability of internally displaced youth dependent on their hosts for their survival. This power dynamic was described in the context of pressures the young IDPs were under to satisfy the wishes of their hosts, whether being subjected to sexual abuse by a member of the host family, being forced to bring in income through transactional sex, or any decision-making related to their sexual and reproductive health (e.g., terminating a pregnancy or not). The occurrence of transactional sex has mainly been attributed to the broader need for economic and social survival. Studies from Malawi27 and South Sudan28 report that transactional sex was widespread among adolescents in situations of financial hardship and displaced youth. Some parents encouraged displaced youth to engage in transactional sex in order to help provide for the family’s basic needs.27,28 When the adolescents became pregnant as a result, in our study and others,28,29 they faced additional pressure from parents/families, clients and/or perpetrators to terminate the pregnancies. Since abortion is illegal in Cameroon, the pregnant youth are subjected to unsafe abortion, causing infections, psychological trauma and even death. The consequences of unsafe abortions are well known.29–31 On the other hand, the pregnant youth who had their child, either by choice (e.g., for religious reasons) or due to lack of access to abortion, faced the financial burden and resulting psychological and social challenges of caring for a child without the needed social and economic support.
The social and economic pressures that led to transactional sex was parallel to the high instances of sexual abuse among displaced youth. Rape and other sexual assaults are commonly reported in armed conflict zones globally and often seen as another weapon of war. Whether military, militia or other armed rebel groups, the politics of rape are unfortunately common throughout history, and sexual violence continues to serve as another weapon of destruction of lives, especially of women, youth and children. Tunamsifu (2015) examined the conflict in the Democratic Republic of Congo (DRC) and explains that when the national army is unable to protect the population, women’s vulnerability is further exploited to weaken moral and emphasize defeat of the community, region or nation.32 Based on our findings, the Anglophone crisis is no different as rape was frequent, and most rapes reported were in relation to either the military or the militia occupying the region.
Until the crisis is resolved and peace returns to the region, it is important that the economic, physical and psychosocial effects be addressed. To prevent STIs and pregnancy resulting from youth sexual activity (consensual and transactional), knowledge about and access to SRH preventive services (e.g., access to contraception, STI preventive methods, testing and treatment) are essential for the displaced youth in this crisis zone of Cameroon. Community stakeholders recognized the need for SRH awareness-raising campaigns and the availability of social and health services for the youth. Further, they called for the involvement of community organizations, including faith-based and non-governmental institutions, to help raise awareness among parents/adults in the region, addressing the detrimental effects of familial and social pressures on vulnerable youth.
The need for psychological support for adolescents’ survivors of sexual violence, forced abortion and other associated traumas were not emphasized but are important to consider for future interventions in the region.
Study limitations and strengths
To our knowledge, this is the first study highlighting the consequences of the Cameroonian Anglophone crisis on youth’s sexual and reproductive health. Donatus et al. (2018) published a study on pregnancy among adolescent schoolgirls in the same conflict-afflicted Northwest region of Cameroon, however, their study is not placed in the context of the crisis.33 Our study adds to the conversation about conflict-related sexual violence and its effect on youth. The involvement of a large sample of multiple stakeholder groups is a strength of this study, highlighting the concerns of the community as well as giving voice to their proposed solutions for youth SRH in the region.
Limitations of this study include recruitment bias, which may have been derived from the convenience sampling, and social desirability, which may have influenced the responses of participants during the forums. To help reduce the potential for responses guided by social desirability, we ensured that each stakeholder group were homogeneous and were able to triangulate data. For example, healthcare providers and NGO representatives expressed that SRH was easily accessible to adolescent, whereas adolescents interviewed and Youth2Youth’s community assessment identified access to SRH was a problem.
CONCLUSIONS
The ongoing armed conflict in the English-speaking Northwest and Southwest of Cameroon has had a devasting effect on the SRH and wellbeing of youth living in these regions. In this study, we found that the crisis created a hostile socio-economic environment that led to internal displacements and idleness among the youth, making them more susceptible to sexual violence and transactional sex. The consequences included unplanned pregnancies, acquisition of STIs, unsafe abortions, trauma and psychosocial distress. Moreover, the community stakeholders involved in this study suggested that raising awareness about SRH, providing services for SRH, and addressing issues of idleness and social norms are vital to improving adolescent and youth SRH outcomes in these conflict-hit regions. The findings of this study highlight the importance of raising awareness on SRH risks of adolescents and youth in regions affected by armed conflicts and the necessity of adopting a community approach in developing interventions and policies to improve adolescent and youth SRH. Analysis of our forum discussions revealed a clear link between the displacement of adolescents and youth from their homes to host families and the need and/or pressure to engage in transactional sex in the crisis region.
Acknowledgements
We would like to thank all the youth and community members who shared their experiences, perceptions, and suggestions for addressing the issues faces by youth in this time of crisis.
Funding
The initial project conducted by Youth 2 Youth that eventually led to this study was funded under the Rapid Response Mechanism grant provided by Family Planning 2030.
Authorship contributions
M.E.B and J.N.F conceived the research idea. M.E.B, J.N.F, and J.C.N contributed to data collection. A.P.A, A.G, and D.A.T contributed to analysis and interpretation. M.E.B, J.N.F, A.P.A, A.G, and D.A.T contributed to preparing the first draft of manuscript. M.E.B, J.N.F, A.P.A, A.G, J.C.N, and D.A.T reviewed and edited the manuscript. All authors approved the final version of the manuscript.
Disclosure of interest
The authors completed the Unified Competing Interest form at http://www.icmje.org/disclosure-of-interest/ (available upon request from the corresponding author) and declare no conflicts of interest.
Correspondence to:
Micheal Ebangha Besong, MD
Youth2Youth, Cameroon
The Biotechnology Center, University of Yaoundé 1, Yaoundé, Cameroon
Email: [email protected]
Tel: +237 676 896 732