_flow_diagram_o.tiff)

Diabetes is a major crisis affecting the United Kingdom (UK), with type 2 diabetes mellitus (T2DM) constituting for 90% of cases.1 Diagnoses have doubled in the past 15 years, and are projected to affect 1 in 10 adults in the UK by 2030.2 This has incurred an increasing burden on society, with costs to the National Health Service (NHS) reaching £10bn a year and 40% of patients reporting diminished psychological wellbeing.3 However, those of south-Asian (SA) background, the largest ethnic minority group in the UK,4 are 2-6 times more likely to develop T2DM5 and report a higher complication and mortality rate than other population groups in the UK,6–8 making them a population of interest. It is therefore valuable to understand the SA-specific factors contributing to these increased rates to combat the rising epidemic.
T2DM is a chronic disorder characterized by persistent hyperglycaemia due to impaired insulin secretion or impaired insulin sensitivity at peripheral tissues.9 The chronic hyperglycaemia causes damage to other systems over time, leading to the development of disabling and life-threatening complications such as peripheral artery disease, renal disease, and retinopathy, as well as a significantly increased risk of cardiovascular disease.9 Optimal glycaemic control is therefore vital in preventing complications. Most commonly diagnosed in middle-aged people via blood glucose tests,10 symptoms of T2DM include polyuria, polydipsia, fatigue and weight loss.11 Risk factors of T2DM involve a complex interaction between genetic, metabolic and environmental factors12 with the latter being of interest in combatting the disease due to its modifiable nature. Unhealthy diet is a key risk factor of T2DM with a role in both perpetuating the illness and its development.13 Lifestyle changes and structured education surrounding healthy eating are therefore central to diabetic healthcare and prevention.14
Much of T2DM prevention and management is centred around lifestyle behaviour. Those at-risk as well as those diagnosed are encouraged to lose weight by reducing caloric intake.15 Emphasis is placed on both the quantity and quality of food, with low-fat foods, healthy carbohydrates such as fruits, vegetables, pulses and wholegrains, and a reduction in red and processed meat being advised.16 Such lifestyle interventions can reduce the risk of developing T2DM by 50%,17 as well as lowering blood glucose levels and improving insulin sensitivity in those already diagnosed. Post-diagnosis, such lifestyle advice therefore forms first-line treatment.14 It falls upon the health professional to offer advice and treatment while taking the patient’s concerns, lifestyle and cultural beliefs in to account to ensure adherence and optimal disease management in the long term.
The term ‘south-Asian’ refers to people of Pakistani, Indian and Bangladeshi descent,18 who currently constitute 50% of the UK’s ethnic minority population.19 As they are known to have up to sixfold the risk of T2DM than the general UK population5 and a higher mortality and complication rate,6–8 they represent a population of interest in combatting the diabetes epidemic, preventing its rising burden and protecting the wellbeing of the public. Therefore, it is vital to understand the SA-specific factors that make them particularly vulnerable. Categorizing individuals by ethnicity such as this relates them to common cultural traditions20 which can be assessed in relation to T2DM. The definition of culture has been argued for decades however, definitions show consensus in that culture is a learned phenomenon shared by and transmitted amongst a group of individuals, encompassing norms, values, behavioural patterns, beliefs and knowledge.21 SAs exhibit significant cultural differences from European people, many of which manifest to affect behaviours related to diabetic prevention and management,22 making them of relevance to tackling the diabetes epidemic. With eating behaviours having a major role in the prevention and management of T2DM, an understanding of such cultural influences on SAs is crucial in encouraging health-related behaviours within the community and combatting their disproportionately high T2DM risk, complication and mortality rates.
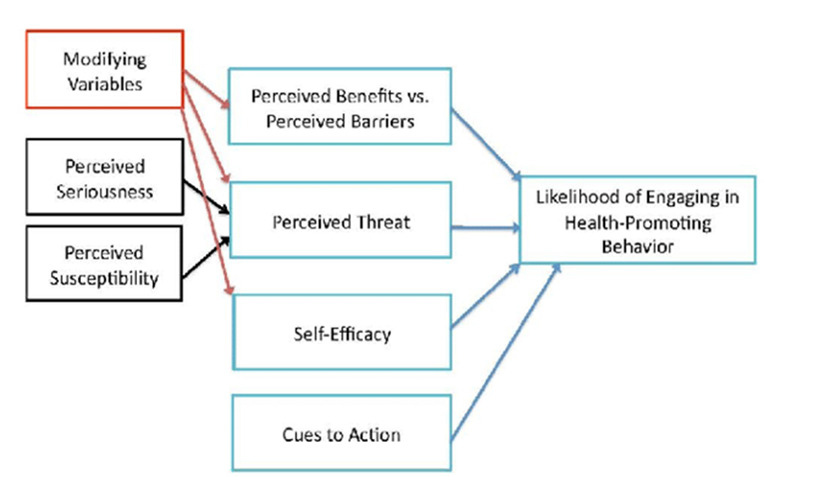
The effective management of T2DM is largely dependent on one’s ability and initiative to perform the relevant health-promoting behaviours, such as healthy eating. With SAs showing low compliance with such behaviours,23 it is of importance to understand why so they may be better encouraged. Behavioural models are often used to increase understanding about factors influencing health behaviours. The health belief model, shown in Figure 1, is a well-validated model used in explaining individuals’ decisions in health behaviours. It conceptualizes six independent dimensions which influence patients’ motivation in undertaking health behaviours; perceived susceptibility in acquiring illness, perceived severity of illness, perceived benefits of action, barriers to action, perceived capacity to act, and cues to action.24 As health-related behaviours form a major role in diabetic control,25 this model effectively encapsulates the factors affecting the management and prevention of T2DM. As such, the relevant dimensions will be applied to explore the cultural influences on SAs eating behaviours regarding T2DM and suggest how they may be encouraged to reduce risk and optimise management following diagnosis.
This literature review aims to identify and critically examine the cultural factors influencing eating practices in the risk and management of T2DM of SA adults in Britain. Specific objectives were to (i) identify, evaluate and critically assess the cultural factors influencing British South-Asians’ eating behaviours in T2DM; and (ii) use the findings to suggest strategies to better enable and support healthy eating behaviours amongst South-Asians, and identify further research areas.
METHODS
The SPIDER (Sample, Phenomenon of Interest, Design, Evaluation, Research type) protocol26 (Table 1) was used to define the key research question – what cultural influences affect British SAs’ eating practices in their risk and management of T2DM?
Search strategy
Initial searches over several academic databases were performed to identify the most appropriate databases; PubMed, Scopus, Applied Social Sciences Index & Abstracts (ASSIA) and International Bibliography of the Social Sciences (IBSS). These searches also allowed potential inclusion and exclusion criteria and filters to be identified. Going forward, all keywords were applied to the title and/or abstract of papers. Narrowing it to the title was too limiting as it excluded those with topical and unclear titles while the restriction of the abstract ensured the keywords were a strong focus of the search papers. Adding individual countries of the SA region as keywords as well as the term “south Asia” and variations of the word “ethnicity” guaranteed all papers studying the appropriate target population would be found. Variations of the word “diabetes” acted as filters to ensure results were relevant. Keywords denoting the UK were also used. The search was restricted to articles published in or after January 2000 as the dynamic, ever-changing nature of culture27 required papers to be recent. Filters limiting the results to certain types of articles were not used to allow a wide range of studies to be displayed, from which systematic reviews could be used for “snowball sampling” of primary studies. Overall, the niche focus of the review meant searches were kept liberal and inclusive, with few keywords, from which papers could then be excluded via double screening and according to inclusion and exclusion criteria.
Data extraction
The literature search took place between 20th and 31st January 2022, with a final updated search on 30th December 2022. Table 2 summarises the total number of searches found in each database.
A total of 1379 papers were identified. Next, a two-stage screening of papers was performed. Firstly, the titles of papers were screened to identify those exploring factors affecting SAs’ eating behaviours in the risk and management of diabetes. Many of these articles explored the effects of physiology, genetics, environmental factors and quantitative factors. Such measures would not adequately explore the role of cultural factors. Therefore, in the second stage, abstracts and full texts were screened according to inclusion and exclusion criteria shown in Table 3. Systematic reviews were used for reference searching, papers from which were also screened according to criteria. Mixed-methods studies were also used with a focus on qualitative data. After the screening, 32 papers remained of which 19 were used in the synthesis after duplicates throughout the four databases were removed. The full screening process is depicted in Figure 2.
_flow_diagram_o.tiff)
Data synthesis and analysis
An iterative approach allowed empirical data to be identified for a thematic analysis in which themes could be described without the bias of predetermined ideas.
RESULTS
Study characteristics
The 19 studies were conducted in England (n=16) and Scotland (n=3). This is near reflective of the settlement patterns whereby SAs constitute almost three-fold more of the English population than the Scottish population.28 Studies conducted in Wales and Northern Ireland were not found. Participants (n=591) were of Indian, Pakistani and Bangladeshi descent. 63% (n=12) of studies included patients diagnosed with T2DM, while 21% (n=4) involved those at risk of diagnosis and 21% (n=4) contained interviews of the general South-Asian population. All papers explored certain aspects of diabetes, from facilitators and barriers of healthy eating to risk perception and understanding of T2DM. This built a holistic overview of how cultural factors shape SAs’ eating behaviours. Table 4 summarises the study characteristics from which the reference numbers will be used as citation numbers within the text.
Perceptions of T2DM
Understanding of T2DM
A simplistic perception equating diabetes solely to blood glucose levels was common throughout SAs29–35 to the extent that interviewees often referred to being diagnosed as ‘having sugar’. While this is not incorrect, the emphasis on blood glucose undermines the full pathophysiology of the disease, as evident by a lack of understanding regarding long-term consequences of T2DM.29,34–36 This is strengthened by the high prevalence of T2DM amongst the SA community and the subsequent construction of it as a norm, leading to a reduced perceived severity of it.30,35,37,38 Despite its prevalence, stigma of the disease was openly voiced by interviewees, with illness being regarded as a ‘weakness’ and ‘embarrassing’.30,32,39 Such fear of stigma hinders access to healthy eating behaviours as SAs try to hide their illness. This highlights the need for greater education surrounding T2DM in the community.
Causes of and factors affecting T2DM
South-Asians’ understanding of the illness is evident in the causes they attribute to it. Seven papers found interviewees noted genetics and family history as key factors in causing T2DM.29,31,33,34,37,38,40 While T2DM is known to have a strong hereditary component,41 this attribution of it as a predominant cause moves their focus away from modifiable causal factors such as diet and physical inactivity.
“…I’ve not eaten sweet foods or fatty foods… and I’ve still got it that means it were genetic because both my brothers’ got it.”38
Furthermore, it was believed that the colder climate of the UK, as opposed to the hotter temperatures of the Indian subcontinent, also played a role in the onset of disease.29,31,36,40,42
The focus on these factors by SAs is worrying as it represents a failure to recognise the role of individual behaviours such as diet as key causes of T2DM, and thereby externalises the responsibility of health away from the self. This is further reinforced by religious factors, and the belief that health is pre-ordained by God/Allah.31,34–38,40 In such cases, it was believed that T2DM is decreed by God and so its onset is inevitable, “no matter how well you are or how healthy you are”.36 The dismissal of lifestyle factors in the development and management on T2DM was a common theme found across eleven papers.29,31,33–38,40,43,44 These fatalistic beliefs and the acceptance of T2DM being out with individual control diminishes self-responsibility in preventing and managing the disease, hindering motivation in undertaking healthy eating behaviours. Therefore, it is vital to promote education of the disease and its risk factors to increase effective prevention and self-management within the SA community.
It is important to note such beliefs were often found to be held by older/first generation interviewees, with second generation and younger interviewees being more likely to mention diet as having some importance.29,30,36–38,45,46
The role of cultural norms
Food culture
A strong theme identified throughout the papers was the role of food culture within SA communities. Hospitality to guests in the form of rich food offerings was commonly associated with social status and affluence, and so to not oblige was seen as a shameful act which would invoke gossip and social rejection.33,36,37,40,44,46 The social importance of food in maintaining relationships therefore promotes rich foodstuffs, high in fat and sugar, as the norm for occasions and dinner parties, making it difficult for interviewees to fulfil healthier food choices.
“We cook special foods in compliance of Bangladeshi society’s expectation. … These foods are cooked for the fear of public scandal.”37
This was problematic for the host, and the recipient also, as interviewees talked of the cultural pressure to oblige in accepting such offerings.30,32,36,39,44,46 Fear of offending their hosts meant interviewees would find it difficult to decline foodstuffs they knew to be unhealthy for them. This was exacerbated by the fear of appearing “different at parties”32 and the pressure to hide their illness due to stigma.
“…people feel that you have a very dangerous kind of disease… it is really embarrassing.”39
Furthermore, food culture is also interlinked with religious factors, further ingraining it within the SA community. Studies focusing on the Sikh population highlighted excessive eating and drinking as a part of Sikh male identity,33,44 while other papers mentioned the rich foods associated with religious festivities as a hindrance to healthier food choices.29,39,40,44,46 A minority of papers found interviewees were able to effectively assess the social significance of rich foods and weigh this against the consequences for their health, and so were able to compromise and eat in moderation at social gatherings.30,36 This demonstrates that, if empowered with the correct knowledge regarding diet, SAs can bypass cultural obligations and fulfil healthier choices, highlighting the need for greater education amongst the community.
The south-Asian diet
A preference for the south-Asian diet they have known since childhood makes it difficult for SAs to adopt healthier changes in the name of preventing and managing diabetes. Traditionally, the everyday diet includes curries cooked in large amounts of ghee and oil; rice and chapattis high in carbohydrates form staple components, while sweets high in fat and sugar are of strong cultural importance at social events.30,32,34,36,37,40,46 While many interviewees recognised their diet as consequential for health, making changes proved to be difficult. The alternative “western” diet was unappealing to many who described it as “bland” and “tasteless”. Using alternative cooking methods with less fat were seen as unsatiating in comparison to the oil-rich foods they were used to. This would then lead to feelings of lethargy and inability to fulfil their daily activities, reinforcing their tendency towards traditional foods.
“If you eat something boiled or lighter, then you feel hungry after a short time…But if you eat fried food more time will pass until you eat next, you don’t feel hungry.”46
The assumption by SAs that they must adopt a Western diet in order to be healthy, as well as the idea that healthier food is unsatisfying, suggests a lack of culturally appropriate advice regarding diet is the underlying cause of SAs inability to make healthier changes in a sustainable method. This was identified by many interviewees who struggled to relate dietary advice given by health professionals to their own food choices.32,40,46–48
“I don’t find enough research about our own foods… and this leads to lack of knowledge about our foods.”32
This is reinforced by Penn et al47 who, when studying the perspectives of Pakistani women attending dietary advice counselling, found that tailored information regarding the use of oil and salt in curries was well received, empowering women to make healthier choices for themselves and their families.
The social roles of the genders
Social expectations of the genders are ingrained within SA culture and present barriers to healthy eating behaviours. SA men were shown to be dependent on others for their diet as the responsibility of cooking resided with females in the household.29,31,32,35,37,38,40,44–46,48 A minority recognised this as beneficial as the involvement of family made fulfilling healthier eating habits easier,29,48 However, the consensus was that this removed males’ control over their diet, leading to reduced awareness and influence over what they were eating and limited ability to make healthier choices.32,35,38,46 This consequence was also reflected in females who struggled to improve their diets due to having to cook according to their family’s eating habits.32,35,38,40 These ingrained gender roles must be considered when tailoring approaches to increase their accessibility to healthy eating behaviours.
DISCUSSION
The literature review extracted cultural influences on SAs’ eating behaviours in T2M. The findings will be used to suggest policy recommendations to support SA’s uptake of health-promoting behaviours, and inform further research. Using Becker’s Health Belief Model (1974); the key themes identified by the review can be separated into three categories; perceived susceptibility and severity, perceived benefit of action and perceived barriers of action.
The high prevalence of T2DM amongst their community diminishes SAs’ perceived severity of the condition as they dismiss it as a novel disease. This is reinforced by a poor understanding of the long-term systemic consequences of T2DM as found to be evident in several papers. SAs, particularly older participants, attribute their risk to unmodifiable factors. This attribution means those who exhibited unfavourable lifestyle behaviours, such as poor diet, do not consider themselves to be at any greater risk because of them, skewing perceived susceptibility. Therefore, greater efforts to educate and spread awareness of the role of health-promoting behaviours and the seriousness of T2DM are needed, to mitigate these established misconceptions.
Due to their attribution of T2DM to unmodifiable factors, SAs show little initiative to engage in health-promoting behaviours to prevent its onset. Some studies found however that, following diagnosis, those who understand the benefit of healthy behaviours are more empowered to fulfil them, for instance, by eating in moderation at social events. The increased willingness to fulfil healthy behaviours after diagnosis may be due to an increased awareness of the benefits of action, having been advised by healthcare professionals. It is also described by the sixth dimension of the Health Belief Model, cue to action, in which specific triggers such as exposure to a health campaign can impact individuals’ actions.49 Therefore, adequate education surrounding the consequences and benefits of diet in T2DM may be effective at mitigating the effects of the deeply ingrained food culture in the SA community and so efforts should focus on increasing such awareness both before and after diagnosis. It also highlights a high regard given to healthcare professionals by SAs as they may adopt their advice in defiance of cultural dietary practices. Healthcare professionals are therefore key actors in supporting health eating behaviours in the SA community.
Cultural norms act as barriers to healthy eating behaviours, demonstrating a complex value hierarchy with culture being placed above leading a healthy life. Barriers involving SAs’ roles within their household were identified, such as men having little influence over their diet and women putting their families first. With these norms, a collectivist ideology oriented to duty and relationships is seen. Collectivism contradicts the theory of identity capital, in which people invest in themselves to thrive,50 and so it follows that SAs dedicate little time to self and to pursuing health behaviours. Due to this collectivist nature of SA communities, recommendations include delivering healthcare in an inclusive manner by working with the family to allow awareness of and facilitate healthier behaviours for all. Building a bigger picture of the patient’s life in this way may help to counteract many of the barriers pertaining to the involvement of family members in fulfilling healthy behaviours and may be done via health consultations with the family rather than with individual patients, subject to patient consent. Discussing healthcare with patients as well as their family provides health professionals with a more holistic idea of patients’ lives, encapsulates their socio-cultural context, promotes advocacy, and improves decision-making for the patient.51,52 Considering the barriers the family-oriented nature of SA culture presents, this would allow healthcare advice to be better suited to the patients’ family dimensions. Implementing this would require reform of the current consultation system to emphasise and facilitate family consultations, using alternative means where necessary to accommodate this, such as the use of video consultations where family members are unable to attend in-person.
Stigma is also a major barrier, not only as stigma of the disease and the desire to hide it, but also in the stigma attached to not keeping in line with cultural norms. This is seen in the expectations of food culture. The importance given to dietary practices and the desire to conform is explained by Goody53 who notes the significance of food in creating identity amongst groups of people and therefore, to refuse it, is to lose identity. As such, the practice of hospitality and indulging in rich diets forms a part of SA identity and creates belonging within the community from which individuals hesitate to sway. However, the stigma and judgement in nonconforming demonstrates a need for better education and awareness throughout the community as well as the normalisation of healthy behaviours. Community-based education programmes are recommended to achieve this. Grace et al37 found enthusiasm amongst religious leaders in using places of worship and their own respected status to deliver lifestyle messages surrounding T2DM. It is therefore of interest to involve such key members of the SA community and use their social capital, the influential power created by social connections,54 to promote healthy living ideals to SA individuals en masse.
Making healthy behaviours more accessible is also necessary to their normalisation. Concerns involve the unavailability of advice tailored to SA diet. Therefore, if the problem is truly to be addressed, wider factors of adapting healthcare advice to cultural needs is necessary. Penn at al47 found dietary instructors of SA descent were able to offer dietary and other lifestyle advice due to their insights as SAs, suggesting empowering community members to act as role models is also effective.
The recommended strategies discussed to support healthy eating behaviours in the South Asian community have been summarised in Figure 3.

Strengths and limitations
This study provided a holistic overview of the cultural influences on eating risk behaviours of T2DM in the adult British SA population. Analytical differences amongst papers meant some data interpretations were restricted to pre-defined themes. Qualitative research also removes access to raw data and primary interview transcripts, limiting the reviewer to the authors’ interpretations. Furthermore, participants’ interviews are dependent on self-reporting and recall of their own behaviours which may be subject to inaccuracies and falsification. Lastly, studies were limited to England and Scotland, although this may reflect the small SA population of Wales and Northern Ireland and subsequent complications of performing such studies in those countries.
Despite these limitations, this study holistically identified a variety of cultural influences on the T2DM eating behaviours in the SA population and so is valuable in developing initiatives to improve healthy eating. The duplication and double screening of results improved search rigour as well as the use of “snowball sampling” as a secondary method of searching. The strong agreements in the findings amongst papers further adds to their quality and the inductive thematic analysis of primary data allowed examination and analysis of original perspectives without the restrictions of pre-defined themes.
Implications for future research
Studies were only found from England and Scotland. This raises questions in the relevance of the study in targeting the SA population in Wales and Northern Ireland as contextual differences may make its findings inapplicable. Therefore, further studies should be conducted analysing the behaviours of SAs in those areas before any efforts to improve them are made. Similarly, regional studies would allow for a deeper insight into the variation between SAs depending on local healthcare services and the demographic, allowing interventions to be context-specific rather than generalising with a nation-wide approach. Furthermore, the suggested strategies have been devised to target the main issues identified by the review, however full background research would need to be conducted to evaluate their efficacy and applicability before introducing them in real-life situations. Lastly, the studies also highlighted the significant roles of language and social support networks in the health behaviours of SAs. As modifiable factors, these influences of the social context should be further explored to identify how they may be improved to support positive health behaviours.
CONCLUSIONS
The findings of this review made apparent the nuances of culture and key areas of improvement, as well as areas of further research, and allowed the development of multi-level strategies to improve health behaviour uptake amongst SAs. Inadequate knowledge regarding T2DM skews SAs’ perceived susceptibility and severity of the illness, and resultantly reduces their perceived benefit of action as the onset and progression of the disease are attributed to factors beyond individuals’ control rather than to lifestyle behaviours. Cultural norms and ideals within the SA community present many barriers to action in the pursuit of healthy eating in the form of gender roles in the household which restrict individuals’ control over their diet, and expectations of rich foods. These strong cultural influences on eating behaviours then clash with those of the western society, hindering effective healthcare delivery. This was seen in the irrelevance of health professionals’ advice to the SA lifestyle.
It is important to acknowledge the facilitators of healthy eating as they may be useful in increasing their uptake. Appropriate education of the importance of diet empowered some SAs to eat responsibly at family occasions. Meanwhile, dietary instructors of SA background enabled healthy behaviours to be championed within the community in a tailored and relevant way. The interaction between the dimensions of influences, from personal knowledge to community norms, to healthcare, emphasises the need for a multi-level, multi-interventional approach. Community-wide education is vital to promote healthy eating via increased awareness and to mitigate the stigma surrounding such behaviours in the community. Health professionals should be made more aware of the cultural challenges facing SA patients, with healthcare advice being adapted to their lifestyle and greater accommodation of family consultations to enable a fuller understanding of their context. With SAs representing a key population of interest in the UK’s rising diabetes epidemic, this will be one step closer to improving the burden of diabetes on the UK economy.
Acknowledgements
This study was conducted as part of an undergraduate research project at the University of Edinburgh, UK. I would like to thank my supervisor Dr Suriyah Bi for her invaluable support, encouragement, and guidance throughout the project.
Funding
None.
Disclosure of interest
The author completed the ICMJE Disclosure of Interest Form (available upon request from the corresponding author) and discloses no relevant interests.
Correspondence to:
Sobia Iqbal
Edinburgh Medical School, University of Edinburgh
47 Little France Crescent, Edinburgh EH16 4TJ
United Kingdom
[email protected]