Self-care refers to the ability of people to promote their own health, prevent disease, maintain health, and cope with illness and disability with or without the support of a health worker. In fact, most healthcare being implemented across the globe is self-care, and not, as often assumed, medicalized care. It is estimated that 65%-85% of health care is provided by the individual or the family without professional intervention using traditional, non-allopathic or allopathic means.1 Self-care interventions include drugs, devices, diagnostics and digital tools that support self-care. With evidence-based normative guidance, an enabling environment in which they can be used, and with appropriate linkages to health systems, self-care interventions provide the possibility of greater self-determination, as well as a means of increasing healthcare access and coverage.
Recognizing laypersons as active agents in their own health care, the World Health Organization (WHO)'s global normative guideline on self-care interventions2 recommends people-centred, holistic approaches to health and well-being for sexual and reproductive health and rights (SRHR), with consideration of the environment in which people live and their individual circumstances, needs and desires across their life course. Examples of such interventions include: self-monitoring of blood glucose and/or blood pressure during pregnancy; self-administration of injectable contraception; use of ovulation predictor kits; pregnancy self-testing, for contraception and fertility care; self-management of medical abortion for safe abortion care; self-collection of samples to self-test for sexually transmitted infections (STIs), human immunodeficiency virus (HIV); or human papillomavirus (HPV) for, respectively, reducing sexually transmitted infections, knowing HIV status and improving, cervical cancer screening; and lubricants for sexual health and well-being.
This WHO guideline supports the provision of self-care interventions to increase people’s options about when and how to seek healthcare. It offers flexibility in the choice of interventions and in the degree and manner of engagement with health services. The guideline also considers the needs of all people across the gender spectrum, recognizing that there may be differences in the barriers that individuals and communities face accessing quality interventions, in their needs and priorities, in the nature of support required, as well as differences in preferred points of access. The guideline is informed by a conceptual framework that includes key enablers such as health literacy, which is crucial as access to correct health information and the capacity of people to use it effectively shapes self-care patterns. Ultimately, understanding how well SRHR outcomes are advanced through the use and uptake of self-care interventions requires implementation research under real-life conditions.
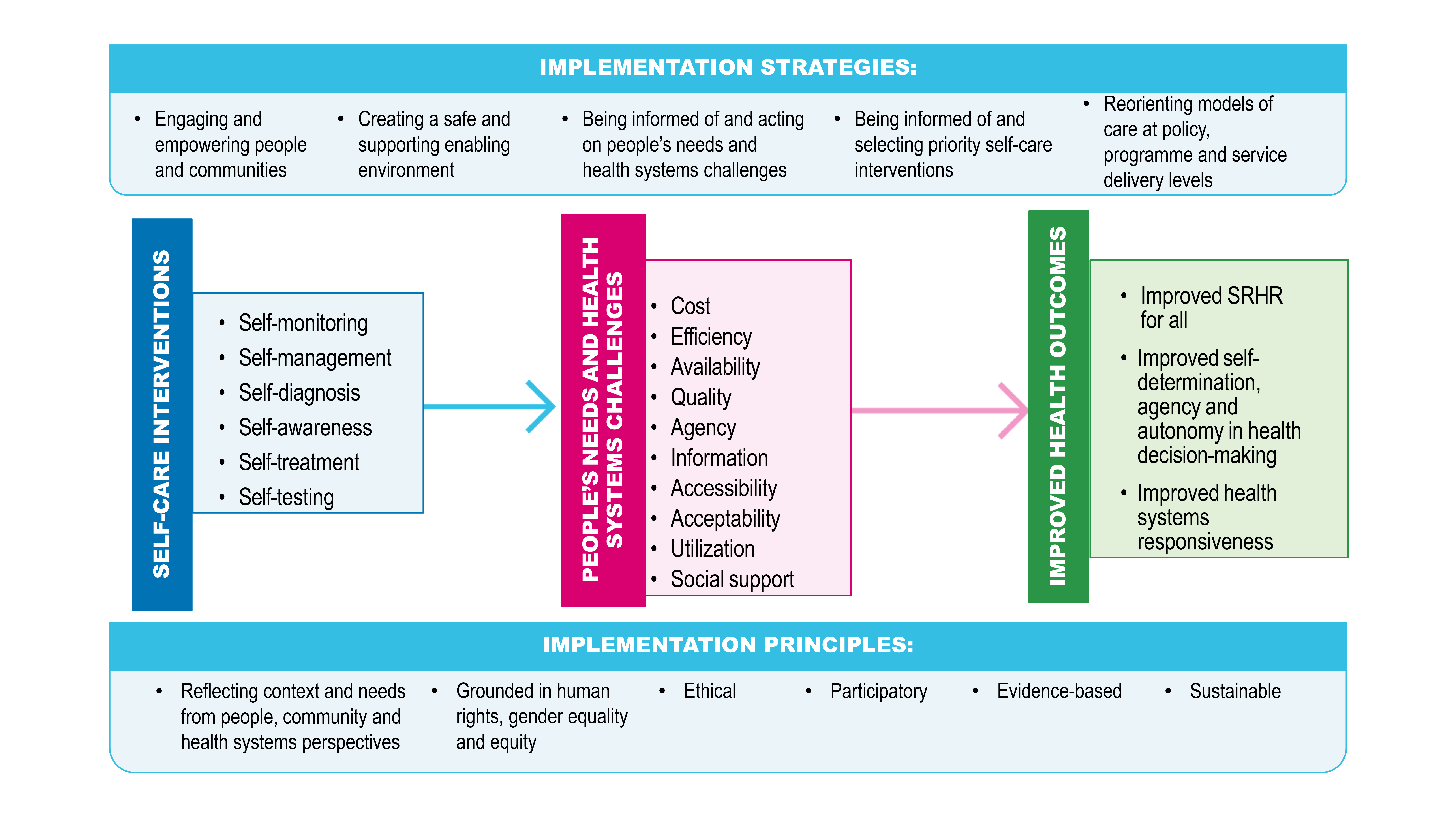
In this paper, we present a new conceptual framework for the implementation of self-care interventions for SRHR (Figure 1) that considers both people-centred and health systems factors to support sustainable change in health care.
.png)
Implementation considerations for self-care for sexual and reproductive health and rights
Studies across different countries, using a variety of research methods, have consistently shown that self-care is the most dominant form of care in high-, low-, and middle-income country contexts.2
As outlined in the WHO conceptual framework for self-care interventions that informed the guideline, the ability of individuals and communities to self-care depends on the availability, accessibility, affordability and acceptability of a range of quality, evidence-based self-care interventions. In alignment with this, the WHO classification of self-care interventions3 for health takes a people-centred approach, describing what self-care means in all its dimensions and presenting a standardised language to support dialogue between public health practitioners working in key areas, including analysis and synthesis of evidence and research. Building on previous studies and aligning with the classification scheme, we describe key implementation considerations, including: agency, information, availability, utilization, social support, accessibility, acceptability, affordability, and quality. These considerations form the foundation of a model implementation framework that was developed using a general ecological health systems approach, highlighting the interaction between micro-level (e.g., agency), meso-level (e.g., social support) and macro-level (e.g., availability) dynamics.
It is important to note that the key considerations informing this implementation framework reflect overlapping and interacting elements that do not exist in siloes.
Agency: How people relate to each other and how they value diverse self-care interventions is shaped by socio-cultural norms and values.4 For instance, in many settings, lesbian, gay, bisexual, transgender, queer and intersex (LGBTQI+) and other marginalized individuals and communities, such as indigenous peoples experience devaluation in health care settings. This mistreatment may motivate LGBTQI+ persons to seek out self-care interventions to mitigate systematic and chronic stigma, discrimination and violence experienced in social and health systems.
In another example, stigma surrounding adolescent and pre-marital sex may present barriers for women’s access to and use of oral contraceptive pills, due to disclosure concerns. In Ethiopia, informants preferred to use emergency contraception (EC) to prevent becoming pregnant, because having sex was infrequent and unplanned, and EC allowed for discrete use that allowed clients to take the pill and throw away the packaging.5 Among young Canadian women from different socio-cultural groups, misconceptions about ECs as an abortifacient, the moral (self)judgement regarding use, and a lack of information about both access points and certified pharmacists to prescribe ECs were the biggest barriers to their use.6 In Bangladesh, women who engaged with “menstrual regulation” (the local term for an abortion) and in turn were targeted by a health intervention to increase contraception uptake experienced significantly higher intimate partner violence than women in the control group.7 After a training in Mozambique, women with sufficient bargaining power in their relationship were able to convince their partners to use female condoms as protection against HIV infection, while the least empowered women continued to have unprotected sex.8
Information: Misinformation and the mistrust and misuse of information may present challenges for correct understanding and use of self-care interventions. Providing user-centred knowledge, via channels that are user-sensitive and tailored for age, cultural, gender and sexual diversity,9 including digital health interventions10 to improve health literacy, can help to overcome this challenge. Pharmacy- and community-based delivery models are also promising avenues to information provision.11
People’s uptake of self-care interventions is also shaped by their education and knowledge regarding SRHR, including notions of risk. Studies on low acceptability of male condoms in South Africa, for example, point to a prevailing concern that blocking the flow of bodily fluids is bad for health.12 Moreover, young women’s resistance to contraceptive uptake in some settings is linked with worries that using a pill every day to prevent pregnancy will cause infertility.13,14 Post-coital methods may be preferred because women can choose to keep or terminate a pregnancy when menstruation is delayed.15,16 Such risk perceptions and pragmatic considerations need to be addressed when promoting engagement with effective self-care interventions.
Availability: Several inefficiencies can hamper availability of care. These include poor planning and coordination among health sectors and services; inefficient transportation; poor (timing of) availability of services, products and/or health workers; and a delayed provision of care. Delivery or follow-up infrastructures are often unreliable or lacking, in remote areas, in fragile and humanitarian settings, or among marginalized communities for many SRH commodities, and this is even more of a challenge for newer options such as self-care interventions.17,18 Commodities may also be only available for selected self-care interventions for SRHR within short-term research interventions in limited settings and geographies, such as self-injectable contraception in Morocco.19
Utilization: The diverse SRHR needs of people across their life course means that they can use self-care interventions to fulfil short-term needs and goals and/or over longer periods across their life. People might turn to self-care for positive and health promoting reasons, which include convenience, cost, empowerment, a better fit with values or daily lifestyle, or because the intervention provides the desired options and choice. People may also opt for self-care to avoid engaging with the formal health system because of a lack of quality care (e.g., stigmatization by health workers) or a lack of access (e.g., humanitarian settings or geographically remote areas).20 By examining common self-care practices, such as the use of fertility tracking apps21 or the use of gender-affirming hormones,22 health policy makers can gain insights in prevailing SRHR needs. For instance, self-care may be the only option for SRHR needs that are not met by formal health services, such as widespread self-management of medical abortion bought over the counter in pharmacies in countries with restrictive abortion laws and/or low access to contraceptive and/or abortion care.23
People affected by conflicts, climate change, and emergencies may need STI prevention, abortion and post-abortion care, post-rape clinical management, and HIV prevention and care. Data are scant in fragile and humanitarian settings where affected individuals may particularly benefit from the increased opportunities for privacy, confidentiality, and access that self-care interventions for SRHR may offer compared to services offered in often overstretched health systems.24
Social support: Self-care interventions are affected by social roles, including marital, family and intergenerational ties – all of which are gendered,25 and other social relationships extending to friends and other social networks such as peer-groups and patient organizations. Social networks can be empowering, facilitating access to knowledge and resources to benefit from self-care approaches, including access to information from healthcare workers.26 Conversely, when they are not supportive or enabling, social relations and communities can pose barriers to accessing and engaging with self-care options.
Inequitable gender norms can reduce sexual decision-making power in intimate partnerships and in turn reduce agency to engage with self-care approaches, particularly in contexts of intimate partner violence. In crowded living conditions with family, lack of privacy can also produce barriers to engaging in self-care for SRHR due to fear of unwanted disclosure (e.g., adolescents accessing over-the-counter contraception at pharmacies). In-depth understanding of local webs of social relationships is therefore critical to enabling access to self-care interventions for SRHR for all. In Uganda, a training program for sengas (father’s sisters) was developed to provide sex education to adolescent girls. This innovative sexual health programme resulted in improved HIV protection practices (use of condoms) by young girls.27 High levels of community engagement and mobilization can increase the implementation potential of self-care interventions by signalling locally relevant solutions.
Peer support networks reveal that people feel comfortable learning and sharing experiences with peers where there is a level of shared trust. Peer-sharing of experiences and information may be particularly relevant to communicate knowledge regarding what can be expected when using self-care technologies. A woman preparing to take abortion medication without assistance might prefer to read users’ narratives rather than a bullet point list of side-effects, as peer support can provide insights regarding social implications and embodied experiences.
Peer support is especially important for marginalized communities, such as transgender people. Qualitative studies reveal the ways in which peer networks share information on hormone use for gender-transition and affirmation, information on pharmacies where hormone pills and injections can be bought over the counter, and places where injections can be administered.5,28 Peer networks also distribute hormones from countries where they can easily be obtained over the counter (e.g., Thailand, India) to people in other locations lacking access.5
Accessibility: Accessibility may be compromised by the limited availability and physical proximity of services, but also by socio-cultural barriers such as inequitable gender dynamics, stigma and discrimination.29 For instance, access to condoms can be a problem for women in contexts where health workers may not provide them to women without their husband’s explicit permission.30 In such cases, not only is there a need for better access to affordable quality self-care, but also for policy change alongside the self-care interventions.
In some settings, where people’s sexual health needs are highly stigmatized, relatively anonymous access routes (e.g., pharmacies for emergency contraception) could improve users’ abilities to self-manage—although at times pharmacists may play a ‘reluctant’ gatekeeper role.31 Access to contraceptives and HIV prevention tools can, for example, be increased by making them available at offices, children’s and /or family care facilities.32 This expanded access to self-care technologies could mitigate disclosure in social networks. While self-vending machines have been proposed for HIV self-testing kits, concerns have been raised regarding the confidentiality of such machines if located in a public area.33
Acceptability: Acceptability at the local level requires people to be properly informed about alternative means of delivering and accessing care. For instance, self-care interventions for SRHR must be accompanied by a) accurate, understandable and actionable information, in accessible formats and languages, about the intervention itself and how to link to relevant community- or facility-based healthcare services, and b) the opportunity to interact with a health worker or a trained peer supporter to support decisions and the use of the intervention. Effective use of self-care technologies requires skills, self-efficacy, access to non-judgmental care, and in some cases, partner engagement. Thus, intervention approaches for enhancing capacity for effective use could include behavioural counselling and rights-based approaches for advancing empowerment of marginalized populations, including and extending beyond women’s rights, sex worker rights, and LGBTQI+ rights.9
Affordability: Although evidence on the costs, cost-effectiveness and financing of self-care interventions is limited, various economic considerations present challenges to the implementation of self-care interventions. These include lack of effective and continuous resource allocation and of insurance policies.34 Lack of funding for health workers or pharmacists to provide counselling and health promotion regarding correct usage of self-care interventions (e.g., pre-exposure prophylaxis, EC) also present challenges.35 Importantly, costs may be transferred from the health system to end-users; the affordability of products and services may present concerns for potential beneficiaries of self-care interventions. This includes out-of-pocket costs of accessing health services (e.g., transportation costs), days lost to work, food, and payments required for diagnostic services.36 Although self-care often means self-financed, data suggest that self-care could reduce indirect user or patient costs and the risk of financial hardship for a household; but equity must be integral to the economic assessment of self-care in terms of costs, benefits, and financing.37
Quality: In settings where health care functions well, personal relations of trust between health workers and their clients provide a foundation to support self-care in the community.38 However, there has been little focus on capacity development of health workers to support their clients’ self-care effectively and safely. Many health workers are poorly equipped and trained (and sometimes unwilling) to support client self-care and health systems often prioritize clinic-based over person-delivered care. A competency framework for health workers with minimum standards for self-care interventions may give clarity to expected behaviours, delegation of tasks and task-sharing, training needs, curricular development, and supports the clinical governance of safe, quality integration of self-care practices and interventions into health workers’ practice.39
A framework for implementation of self-care interventions for SRHR
The framework for implementing self-care interventions for SRHR (FIS-SRHR) (Figure 1) is proposed to guide national efforts to strengthen health systems and people-centered care. This framework draws on published literature, WHO normative guidance, and international agreements such as the Declaration of Astana to advance Primary Health Care (PHC) The framework is not intended to provide a one-size-fits-all approach, but describes an operational approach which can be used to guide and inform national planning processes and decision-making for the implementation self-care interventions for SRHR. Acknowledging the wide range of socio-economic settings, health status of communities, and health system capacity, the FIS-SRHR is intended to be applicable to a wide range of countries. It comprises the nine implementation considerations described above, for a range of self-care interventions which may facilitate sustainable change in healthcare.40
As mentioned previously, the components of this framework reflect overlapping elements. For instance, a critical element of any strategy to implement self-care interventions is the presence of enabling environments to improve SRHR outcomes and equity. In countries where reproductive rights are not respected, there may be a need for advocacy, political will, leadership, and multi-stakeholder partnerships that can ensure the creation of enabling environments. This can include a supportive regulatory environment (i.e., laws and guidelines, ethical and human rights frameworks, avenues for accountability) such as regulatory changes to move from prescription-only to over-the-counter availability of medicines. Policy changes may also be needed which may include, for instance, promoting self-care behaviours among communities, ensuring access to affordable self-care commodities, and/or developing health worker competency-based training. The use of the FIS-SRHR to introduce or scale-up self-care interventions should therefore be informed by a robust evidence base, both local (for example, the social, economic, and environmental situation and trends in the country, the disease burden, and the strengths and weaknesses of the health system) and global (for example, what has been shown to work or not work in improving PHC), as well as by the values and preferences of a diverse range of stakeholders.
Research remains essential to maintain a robust evidence base and equitable approaches. Implementation studies can therefore examine regulatory and health policy factors to better understand why interventions work in some settings but not in others. Implementing self-care interventions for SRHR and adapting based on evidence from further research, has the potential to improve impact and health efficiencies. Table 1 describes published research pertaining to each implementation consideration carried out in a range of settings. Standardized implementation science approaches, such as the consolidated framework for implementation research (CFIR), could guide research on contextual factors shaping the effective roll-out of self-care interventions for SRHR.41
We hope that this FIS-SRHR for implementing self-care interventions can be applied using a range of methodological tools in a variety of global contexts across myriad self-care strategies for SRHR, to help generate a robust evidence base of much needed implementation research to advance SRHR for all. As this nascent field develops, understanding how implementation can be tailored to meet population, context, and SRHR-strategy specific needs can inform future roll out and scale-up of self-care interventions for SRHR in ways that advance health and rights. The evidence resulting from such studies can also serve to inform the development of WHO implementation guidance for self-care interventions and future guideline considerations. This FIS-SRHR can help guide generation of insights from the multitude of self-care interventions that are being used globally, which in turn can help expand the implementation of WHO’s recommendations on self-care interventions on the ground. The successful expansion of self-care interventions for SRHR will depend on innovative implementation research that can effectively close the ‘know-do gap’ and have impact far beyond the confines of pilot testing sites.
Disclaimer
The named authors alone are responsible for the views expressed in this publication and do not necessarily represent the decisions or the policies of the World Health Organization (WHO) or the UNDP-UNFPA-UNICEF-WHO-World Bank Special Programme of Research, Development and Research Training in Human Reproduction (HRP).
Funding
We gratefully acknowledge financial support of The Children’s Investment Fund Foundation (CIFF). The funder played no part in the decision to submit the article for publication, nor in the collection, analysis and interpretation of data.
Authors’ contributions
The manuscript arose from discussions between MN and AH following the publication of the WHO guideline on self-care interventions in July 2019. MN and AH developed the first draft of the self-care implementation framework which was then discussed during an implementation research planning meeting in Amsterdam in November 2022 with CL, JH, MA, WJ and ES. MN and AH wrote the first draft of the manuscript which received substantial input from CL and JH. The final revision was sent to all authors who also provided support to formatting and referencing. All authors provided input to the manuscript and the submitted version has been approved by all authors.
Competing interests
The authors completed the Unified Competing Interest form at http://www.icmje.org/disclosure-of-interest/ (available upon request from the corresponding author), and declare no conflicts of interest.
Acknowledgements
Emma van Dalen and Hayley Murray reviewed the illustrative case-studies.