As of May 2023, the COVID-19 pandemic has affected over 766 million people, and about 7 million deaths are recorded (0.9%). While the recovery rate, estimated at 94.6%, is encouraging,1 an unprecedented level of burden was laid on public health resources during this pandemic.2,3 The greatest challenge was, not just finding a cure/prevention for this viral disease, but dealing with the aggressive host response and long-term sequelae.4–8 Complementary medicine, especially individualized medicine (such as homeopathy) focuses on optimization of the host response during infection, and therefore may be required in the fight against the COVID-19 pandemic.9,10 Homeopathy is a system of therapeutics that approaches the concept of treatment with an individualized remedy for each patient. It recognizes the existence of an all-governing defense mechanism in every individual, whose function is to keep the organism alive.9 Homeopaths consider disease an expression of the defense mechanism’s helplessness to maintain health, analogous to a compromised state of existence, in order to continue living.9 This effort (disease and symptoms) is highly individualistic and the treatment, therefore, is tailored to each person.9 There are definite rules and principles that govern life, disease and health which homeopathy adheres to. The homeopathic principle is about applying highly potentized medicines whereby the crude drugs, sourced from all naturally available resources, are subjected to serial dilutions and a succussion process, for the achievement of gentle, deep and lasting resolution of the disease.11
This therapy has benefited many chronic and acute diseases, including epidemics.10 The same was expected in the COVID-19 pandemic as well. While many countries do not have specific regulations and guidelines about the use of homeopathy to treat COVID-19, some do. India, for example, a country that has adopted homeopathy into the National Healthcare System, issued a directive that homeopaths may provide immune-boosting remedies to the public and may administer adjuvant homeopathy with conventional drugs in probable, suspected and/or confirmed cases.12 At this time, pandemic readiness has been questioned in many settings, and deeper introspection on our healthcare policies is needed. During the lockdown, with heavy congestion at hospitals, in most countries, homeopaths’ advice was sought using telephone/video calls, and the remedies were administered remotely.
Homeopathy cannot be assessed as a single system of therapeutics, as the approach to the application of the principles of practice varies greatly. Many ‘schools of homeopathy’ have propounded their own approach for COVID-19 treatment, which may or may not conform to the core principles.13 Classical homeopathy is the practice of homeopathy as originally laid down by the founder C F S Hahnemann M.D., where the effectively proven principle of individualization and single remedies reign in every scenario, including epidemics.11
With a background of diversity in the comprehension and application of homeopathic principles, we sought to curate data on cases treated with classical homeopathy. Our aim was to bring clarity in terms of the approach and to have sound data to plan future studies and inform policymakers on using classical homeopathy in COVID-19 treatment. The secondary objectives were to identify the remedies that helped, the main symptoms that were presented and the factors associated with the disease severity.
METHODS
Study design
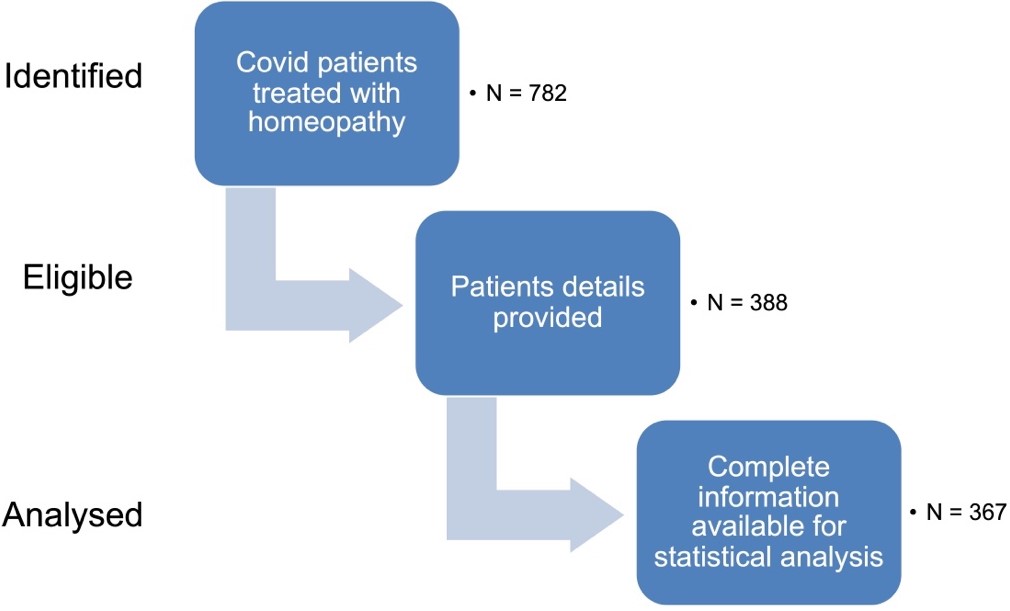
This was a retrospective observational study. We retrospectively investigated cases already treated by homeopaths, and where patients had volunteered to take classical homeopathy for the COVID-19 symptoms. No control group observation was included. The process of identification, recruitment and inclusion of cases is represented in Figure 1.

Data sources
The project was executed by an international team of homeopathic physicians who specialized in the classical approach and belonged to the scientific committee of the International Academy of Classical Homeopathy in Greece. The data were carefully and transparently curated to ensure reproducibility. Classical homeopaths who were ‘diplomates’ of the International Academy of Classical Homeopathy (IACH) were asked to provide details on cases they treated by filling out a standardized questionnaire (Online Supplementary Document).
Participants
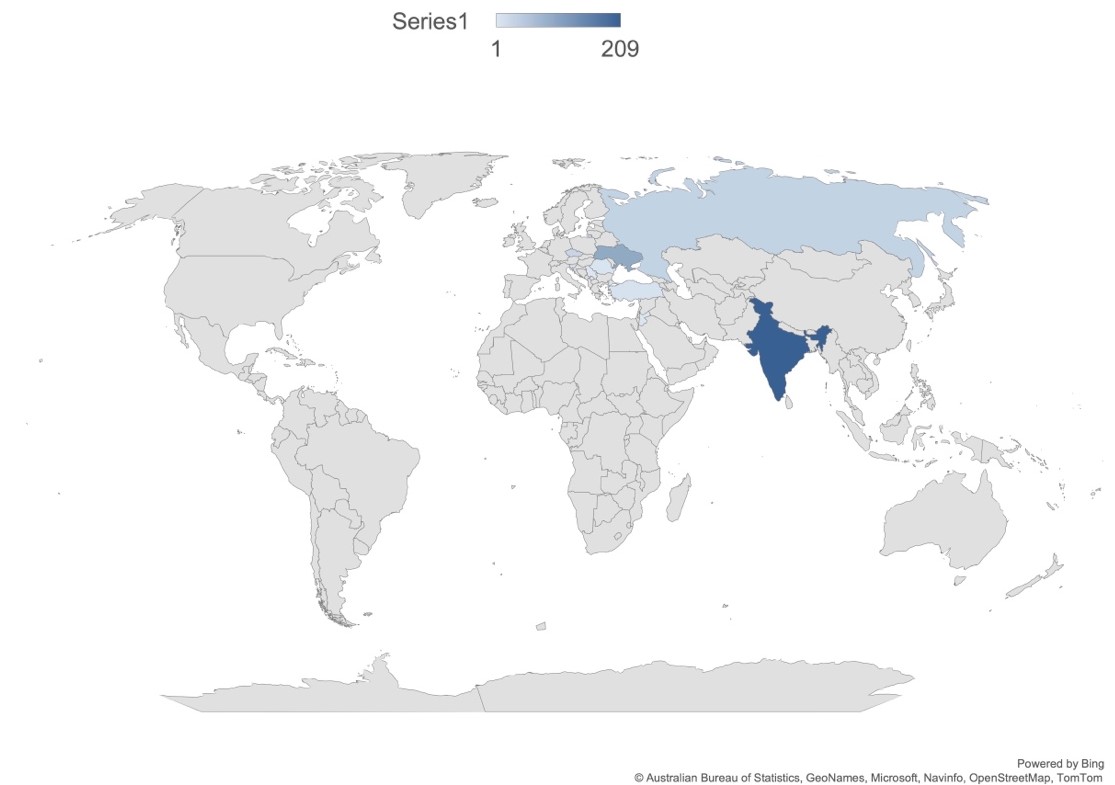
We included patients diagnosed with COVID-19, of any age, sex and geographical location, diagnosed as suspected/probable/confirmed case, as determined by reverse transcription polymerase chain reaction (RT–PCR) or antibody tests for S antigen or nucleocapsid antigen, or clinically diagnosed according to the WHO parameters (Online Supplementary Document). The details of the cases were collected consecutively as the treating homeopaths sent them, irrespective of outcome. Cases were sent in anonymized form to investigators by IACH diplomates from 9 countries (Figure 2). Case reports that did not furnish complete participant and treatment details or contain an accurate diagnosis were excluded.

Intervention
We considered patients treated with classical homeopathy either (i) stand-alone or (ii) combined with conventional therapy for COVID-19 according to the provisions in each country. We did not distinguish the two types at this point. Patients were followed up until they were free of symptoms, or a negative PCR test was available.
Outcomes
Primary
Primary outcome of the study was improvement in COVID-19 disease status under classical homeopathy – classified as ‘improved’, ‘not improved’ or ‘progressed’ post-treatment. ‘Improved’ implies symptomatic, general and/or laboratory investigation improvement, with details provided on the response and time taken for said improvement. ‘Not improved’ refers to no improvement in the above parameters. Progressed refers to the progression of the disease to severe disease or the development of complications of the disease. For mild to moderately severe disease, recovery in 7 days was considered to be “improved”. Recovery after 7 days was considered to be “not improved”. For severe disease, up to 15 days to recovery was considered to be “improved”, and over 15 days was considered to be “not improved”. This time limit was based on the observations published by researchers to date on the time course for recovery under conventional treatment.14–16
Secondary
The secondary outcomes of interest were (i) number of homeopathic remedies required for improvement in each case; (ii) main presenting symptoms and other symptoms; (iii) factors associated with severity and complications – fever (yes/no) and fever temperature if available, age and sex, geographical location, time period of infection (wave), comorbidities.
Analysis
Data set fields
The data were gathered under the field headings as seen in Table 1.
Considering potential variability in the individual physician’s case-taking style and bias regarding the response to treatment, we provided a standardized data collection form (Online Supplementary Document) and requested that the physicians furnish data irrespective of the outcome. Uniformity was achieved by excluding case reports that did not adhere to this format, deeming them incomplete forms.
Case reports validation
All the case reports were independently internally audited by a three-member committee of the scientific team to maximise validity of the treatment effect and ensure the reproducibility and completeness of data. The data gathered were plotted on an Excel sheet, and basic statistical analysis was carried out on the cases that provided complete data to obtain an initial impression. For nominal variables we conducted Cramer’s V and Pearson’s correlational analysis. We analyzed the attributability of improvement to relevant parameters through a multinomial logistic regression model. This analysis, however, is not projected to be of any scientific importance yet, as the data at this stage could be confounded and biased in many ways.
Ethics clearance
This study was approved by the Centre For Classical Homeopathy Institutional Ethics Committee (PP/AS/01/19-20). The informed consent was waivered as the data was gathered after anonymising the information at source. The homeopaths sent the data without any patient identifying features. The patients had volunteered for classical homeopathy during the episodes, most of the time online or by telephone due to movement restriction imposed at that time. The treatment was mostly adjuvant, and no claim was made as an alternative to conventional medicine, by any of the homeopaths. The investigators had no direct contact with the patients.
RESULTS
In the cases considered for statistical analysis (N=367), with males and females being 166 and 201, respectively. The mean age of the participants was 42.75 (± 17.03) years, . The mean follow-up period was 6.5 (standard deviation, SD=5.3) days, with a median of 1 remedy used.
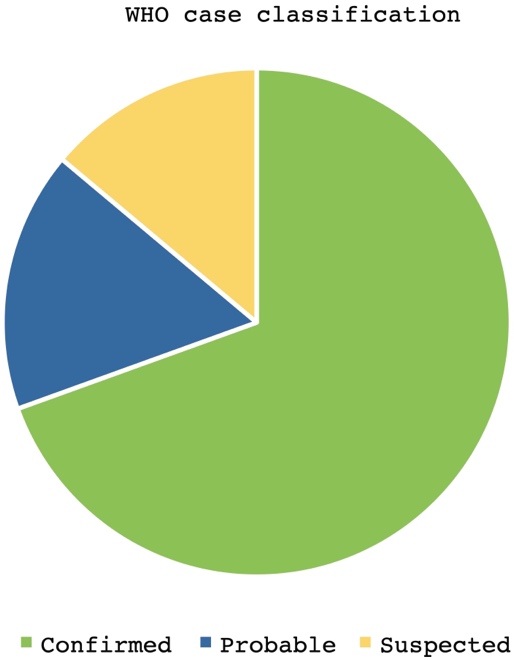
A total of 192 patients were diagnosed by RT–PCR, 111 by the WHO clinical criteria and 64 via retrospective antibodies. According to the WHO criteria, 255 were confirmed cases, 61 were probable cases, and 51 were suspected cases (Figure 3).

Primary outcome
Improvement under classical homeopathy
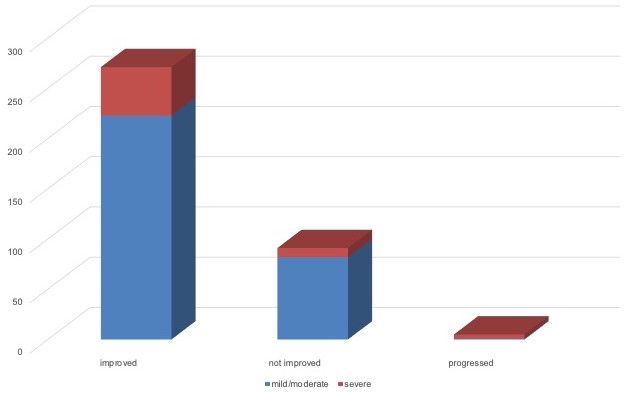
Overall, 271 (73.8%) of the reported cases improved under homeopathic treatment, 91 (24.8%) did not improve, and five cases (1.4%) progressed to become complicated. No deaths while under their care were reported by any homeopath. However, this is probably because most of the serious cases were in the ICU, and not accessible for homeopathic treatment. Severe disease was seen in 61 of the 367 (16.6%) cases. Of these, 48 people improved under homeopathic treatment, 9 did not improve, and 4 progressed to become complicated (Figure 4).

We assessed the correlation between improvement with homeopathy and severity of disease using Cramer’s V correlation between two nominal variables. The improvement status with 3 levels (disease progressed, no improvement and improvement) and disease severity with 2 levels (mild/moderate and severe) were factored in for the correlational analysis. The Cramer’s V value was 0.220 (P<0.01), indicating that there exists a significant moderate positive relationship between improvement status and disease severity. This indicates that improvement was more common among patients with severe symptoms than among those with mild symptoms (Table 2).
Secondary outcomes
Most common remedies used, and association with improvement in COVID-19
We plotted the frequency table for the most frequently used remedies (≥10 cases) (Table 3). It was observed that the most commonly used remedy was Arsenicum album, with a total of 103 cases treated with it. The second most commonly-used remedy was Bryonia, with a total of 100 cases and the third most commonly-used remedy was Pulsatilla, with a total of 48 cases. 200C was the most commonly-used potency for all these remedies (Table 3). The point-biserial correlation computed between the status of improvement and the number of remedies, showed the Pearson correlation coefficient to be -0.387 (p < 0.01). This indicated that as the number of remedies prescribed increased, the level of improvement decreased slightly among patients (Table 2).
Main symptoms at presentation
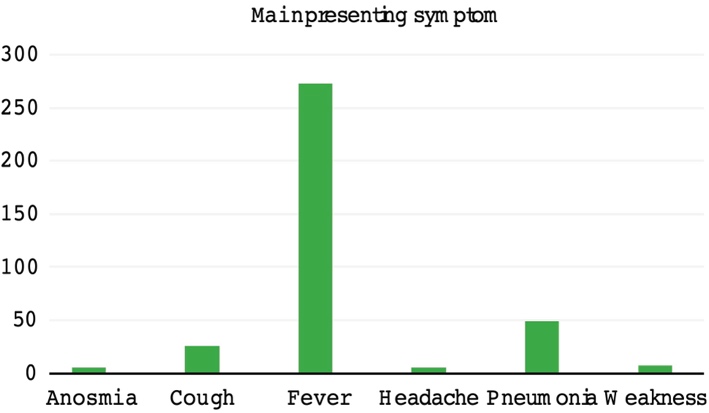
Fever was the most common symptom at presentation, with 273 (74.4%) patients presenting with fever. Forty-nine patients directly presented with pneumonia, detected on radiological imaging. Where fever was absent, the main symptoms at presentation were cough in 26 cases, weakness in 7 cases, anosmia/ageusia in 6 cases and headache in 6 cases (Fig 5).

Factors associated with severity of COVID-19
Fever: Presence of fever was the prime focus of our analysis. For cases with known body temperature at presentation (N = 339), we calculated the Cramer’s V correlation between two nominal variables, namely, improvement status with 3 levels (disease progressed, no improvement and improvement) and presence of fever with 2 levels (absent and present). The Cramer’s V value was found to be 0.167 (P <0.01), indicating that there exists a significant weak positive relationship between the improvement status and the presence of fever. This indicates that improvement was slightly more common among patients with fever than without (Table 2). Further, we analyzed fever according to four categories of temperature, to assess the correlation between improvement and temperature range. Fever temperature categories and the number of cases in each range are provided in Table 4. The correlation of improvement with fever temperature range was assessed as the Cramer’s V correlation between two nominal variables, namely, improvement status with 3 levels (disease progressed, no improvement and improvement) and intensity of fever with 4 levels of temperature ranges. The Cramer’s V value was 0.100 (P>0.05), indicating that the improvement status is not influenced significantly with intensity levels of fever (Table 4).
Age and sex: Sex was not associated with any significant difference in response to treatment. It was, however, observed that the Pearson correlation coefficient for age was -0.146 (P <0.01), indicating a significant negligible negative relationship between the improvement status and age (Table 2). This means that as the age of the patients increased, the possibility of improvement decreased.
Factors associated with improvement under homeopathy
Using the insights from the correlational analyses, a multinomial logistic regression model was constructed for the nominal data with improvement status as the dependent variable, and the significantly correlated variables, such as the number of remedies, presence of fever and disease severity, as independent variables to predict improvement status. The model fitting criteria value was 57.664. The significance value was less than 0.01, indicating that the final model fit well. The goodness of fit for the model was calculated, and the Pearson value was 20.679 (p>0.05). The significance value was 0.541 (>0.05), thus indicating that the model was an adequate fit. The pseudo-R square values were calculated for the regression model. The Nagelkerke value was 0.311, which means only 31.1% change in improvement status could be attributed to the number of remedies, presence of fever and disease severity. Therefore, the studied independent variables (number of remedies, presence of fever, and disease severity) are not sufficient to predict improvement status.
When computing the likelihood ratio for the regression model, it was observed that the number of remedies (P <0.01), disease severity (P <0.05) and presence of fever (P <0.05) significantly contributed to improvement status. Parameter estimates for the regression model were not taken into consideration, as the data representations across the three categories of improvement status were not comparable. The comorbidities, time period of infection (wave of pandemic), and geographic location were not uniformly available and thus could not be used for analysis.
DISCUSSION
Many databases have been created and are actively collecting data on the new pandemic.17 There are also many reports on the use of traditional and complementary medicine for COVID-19, including homeopathy.18,19 India has pioneered many research projects on both prophylaxis and treatment of COVID-19 with homeopathy.20 However, a database dedicated to this therapy is novel and will go a long way in providing material for investigation in the future.
The preliminary data collected from nine countries have shown some interesting outcomes. The average age of participants and the influence of age on the severity of the infection are slightly different (younger) from those seen in other studies thus far.21–23 This is probably due to the trend of patients opting for homeopathy being in this age range, compared to the general population.
The primary outcome of interest was improvement under homeopathic treatment. This was seen to be significant, especially in severe cases (Figure 4, Table 2). The mean time required for improvement was 6.5 days. While no deaths were reported, this could be due to the hospitalization of most severe cases and cessation of homeopathic treatment under such conditions, although favorable direction was seen in the few severe cases who continued with homeopathy. The most common remedies used were Arsenicum album, Bryonia and Pulsatilla (Table 3), which have been recommended by other studies as well.21 However, it must be noted that contrary to popular belief among homeopaths, no single remedy (serviceable as prophylaxis and/or treatment) emerged as a “genus epidemicus”. We investigated other parameters associated with improvement under homeopathic treatment as secondary outcomes of interest. Fever was the main presenting symptom/condition in most cases (Figure 5), as corroborated by many other studies.21 The stochastic model of symptom progression also corroborates fever as the first symptom that may arise in COVID-19,24 which seems to be the stage at which homeopaths were approached by patients. In the absence of fever, cough, and a clinical/laboratory image of pneumonia (without fever) were seen to dominate. Fever was of special interest as fever is conventionally suppressed during infections,25 whereas homeopathy promotes a high fever during infection as a part of the efficient acute inflammatory response.26,27 Studies have hitherto shown that the presence of fever may be associated with better outcomes during infection although the evidence is still lacking in certainty.25,28,29 In our database, the presence of fever was indeed associated with better prognosis (Table 2). However, the temperature range did not influence the clinical outcome in the cases presented here (Table 4). In previous studies, sepsis and COVID-19 were influenced by the temperature trajectory during the sepsis,30,31 and it would be interesting to investigate whether the temperature trajectory can influence the clinical outcome of COVID-19 in a similar manner.
The number of homeopathic remedies required was strongly correlated with improvement (Table 2). This is in keeping with the homeopathic principles of levels of health.27 Healthier patients present with stronger and clearer symptoms for homeopathic prescription, and their response is quick and in the right direction. Less healthy patients require a few more remedies in the right sequence to bring them up to the same level of efficient response. If a homeopath makes mistakes in identifying the remedy, the response is delayed, and the number of remedies required will also increase. In either case, improvement is inversely correlated to the number of remedies required.27
In this project, the biggest advantage was the uniformity of practice among the homeopaths, despite practicing in different geographical regions. This is of importance because there are no strict rules governing the adherence of practitioners to the established scientific principles of homeopathy. Differences in practice approach, dissimilar to the practice approach in conventional medicine, can change the outcome of treatment in homeopathy. There is a definition of what is considered true improvement when rules are adhered to. If these rules are not followed, there is no direction for a physician and the interpretation of results can be fraught with confounders and biases. In this study, all the practitioners were Diplomates of a specific diploma program, and they adhere to the rules as described above. If data was gathered from disparate practice methods, the data could not be uniform or reproducible.
In this database, not enough information was available regarding the comorbidities in the patients. Hence, we could not analyze the influence of comorbidities on the clinical outcome. This lack of complete information is attributable to telephone consultations, which accounted for the majority of consultations during COVID lockdowns. It will be essential to collect this information for future cases, as studies have shown that comorbidities have an adverse effect on improvement in COVID patients,5 and it will be necessary to evaluate this in any future homeopathic treatment scenarios.
At this juncture, only the presence of fever, number of remedies required, age, and severity of disease could be identified as significant contributors to the improvement status under homeopathic treatment. The impact of other parameters (temperature range, comorbidities, geographical location, period of infection - wave) on improvement under homeopathic treatment are yet to be determined.
The objective of this database was to provide a reliable data pool for those interested in further research. There are simply too many confounders to account for in such a scenario, and the authors suggest a thorough study of this database to account for these confounders in their research plans. Some confounders that were apparent to the authors in this database that need to be considered in future data collection plans are discussed below.
Mode of data gathering: The homeopaths gathered data via telephone consultations and in-person at varying times, which may lead to overemphasis or neglect of certain information. Therefore, a distinction needs to be made with regard to the mode of case taking, and a comparison needs to be made about the completeness obtained with these modes.
Geographic location: While COVID-19 seems to affect patients similarly globally, there could still be differences in how it affects different geographic locations.
Time period of data collection: Each genetic variant of the virus has been affecting the population in a different manner and depending on which time the data were collected the predominant infecting variant may be different. The symptoms and treatment response will likewise vary. Hence, it will be helpful to make a distinction about these. There was a major constraint in some cases in this project that the dates of the first consultation were not provided. Collecting these data will be important for research studies.
Data on temperature trajectory: A lot is being said about the importance of fever in infections. The authors recognize that the presenting temperature alone is not sufficient, but that the course of the illness better depicts the immune response. This information needs to be collected for future cases.
Laboratory parameters: Although the lab parameters suggested for COVID-19 cases are similar globally, the availability of such records to patients and homeopaths varies from country to country. This can be overcome by requesting the parameter measurements and meticulously recording them.
Comorbidities: As outlined before, the method of case taking influences the completeness of the data, and most cases did not detail the comorbidities. This must be overcome, as it is a simple matter of inquiry.
Limitations
This dataset relies heavily on the reporting by homeopathic physicians, which introduces a reporting bias, as it is possible that the physicians may not report cases that did not improve or progressed to complications as readily as they report successful cases. Efforts were made to brief all the participating physicians in advance on the importance of unbiased reporting to minimize this bias. Secondly, the difference in the national health policies of the participating countries makes it difficult to attain real uniformity and is a limitation that cannot be overcome. This introduces a selection bias, as those with mild or moderate symptoms from some countries may seek homeopathic treatment, while in others, there is homeopathic treatment for patients in any condition. Some countries had no prohibition on patients seeking homeopathic treatment as stand-alone treatment, while in countries such as India, it was regulated to be given as an adjunct therapy. There was also some bias introduced due to the incompleteness of data in over half of the case reports sent in. This was mainly attributable to the telephone/online nature of homeopathic consultation in most cases. These were identified as potential biases and challenges for future studies aimed at investigating the effect of homeopathy in COVID-19. The greatest confounding effect is that of conventional medicines taken along with homeopathy, and at this point, this remains an insurmountable challenge. The aim of this study was to provide data for studies in the future, and a prospective design may help overcome these limitations.
Future direction
Despite the confounding and bias, the data we compiled are impressive. We strongly urge governments to consider providing free reign to medically trained homeopaths to deal with COVID cases. Similar appeals have been made by investigators previously.19 The severe cases will, by default, be hospitalized and will not be under homeopathic care, but the burden from mild and moderately severe cases can be significantly alleviated by including homeopaths in care delivery.32 Many other epidemics, including viral ones, have responded well to homeopathy since the days of Hahnemann10,19,32–39; therefore, there are grounds to reconsider homeopathy in the National Health Systems now. Many investigators have made observations and have already registered protocols that need the support of governments to succeed.40 In the future, as homeopaths are being permitted to treat populations during pandemics, an intensive and refined study design should be applied to overcome the confounding and bias that exist in this database. Randomized controlled trials (RCTs) are difficult, as patients may not like being deprived of conventional therapy with such a risky pathology. Therefore, a prospective observational study is the best option for homeopathy, and a comparison study can be established with adjunct conventional treatment as well.
A greater cooperation between homeopathic organizations may be designed to obtain sufficient evidence. The evidence can be further fortified through exercise of uniformity of practice, through conforming to the established scientific practice rules of classical homeopathy. A more elegant study can be devised to obtain evidence of the “genus epidemicus” for homeopaths. Using the levels of health model of Prof. Vithoulkas,27 a retrospective analysis of remedies indicated in the healthiest COVID patients may be analyzed, and evidence towards the possibility of one or few such remedies may be obtained. However, obtaining adequate information size will again be a challenge for such a study, and cooperation among homeopaths will be of utmost importance. COVID-19 seems to attack the immune system more than any other viral disease encountered thus far,41 and homeopathy, being a system capable of enhancing immune efficiency,10 must be given a chance to show its efficacy with an appropriate infrastructure in place.
CONCLUSIONS
This study indicates that classical homeopathy was associated with improvement in SARS-CoV2 infection. The improvement was even more significant for severe disease. Presence of fever, as expected by homeopathic principles, was associated with better chances of improvement. An increase in the number of remedies required and an increase in age were associated with non-improvement. Though this database is fraught with many confounders, which must be taken care of in future studies, it provides ground for scientific investigation of the role of classical homeopathy in SARS CoV2 infection.
Acknowledgements
The authors acknowledge the help of Dr Harshitha Narayanaswamy, Dr Vishrutha M, Dr Pooja Dhamodar and Dr Amritha Belagaje for their technical help. They are also thankful to Akshaya Periasamy for statistical help rendered. The authors also thank Ann Sorrell for English language correction of the manuscript. The list of IACH COVID Collaborators is included in the Online Supplementary Document.
Ethics statement
Centre For Classical Homeopathy Institutional Ethics Committee approved this study (PP/AS/01/19-20) without informed consent as the patient data was not collected. Only de-identified details of the COVID infection and response to treatment were retrospectively sent by primary physicians who treated them. The investigators were not given any patient identifying details nor did they have any contact with the patients directly.
Data availability
All data and supplementary material are available as Online Supplementary Document
Funding
This study received no funding.
Authorship contributions
PH conceived the idea and curated the data along with SM, who also wrote the manuscript and performed the statistical analysis. The ICC are all the physicians who volunteered to send the data for the database, and GV is the guide, auditor and guarantor of the work.
Disclosure of interest
The authors completed the ICMJE Disclosure of Interest Form (available upon request from the corresponding author) and disclose no relevant interests.
Correspondence to:
Centre for Classical Homeopathy,
10, 6th cross, Chandra Layout Vijayanagar,
Bangalore, India – 560040
Email: [email protected]