Adolescence is a critical period when many people initiate sexual activity, but a large proportion of the global burden of diseases arises from sexual and reproductive health (SRH) complications during this period.1 Each year, about 21 million adolescent girls between 15–19 years in low and middle-income countries (LMICs) become pregnant, with most pregnancies unintended.2 About 26% of these pregnancies result in unsafe abortions.3–6 Complications during pregnancy and childbirth are among the leading causes of death among adolescent girls aged 15-19 years in LMICs.6 Adolescent pregnancies are more likely to result in gender-based violence, discontinuation of schooling, and other negative socioeconomic and health consequences,2,7,8 some of which extend to their children, as evidenced by a higher burden of perinatal mortality and low birthweight.4,9
Modern contraceptives are the most effective methods for preventing unintended pregnancies10,11 and reducing pregnancy-related complications responsible for the high maternal and neonatal mortality rates among adolescent girls.12,13 However, coverage of modern contraceptives in LMICs is low, despite universal access to SRH services, including modern contraceptives, being a key target of the Sustainable Development Goal 3 (SDG3).3,12–15 In sub-Saharan Africa, the modern contraceptive prevalence rate among adolescents (percentage of all females 15-19 years who are using a modern contraceptive method) is estimated to be about 15.6%.16 In West and Central African, countries such as Democratic Republic of Congo, Guinea, Mozambique, Niger, Nigeria, and Senegal, only 10% of the demand for contraceptives by adolescent girls in need of pregnancy prevention is satisfied by modern methods.17
Sierra Leone has one of the youngest populations globally, with more than half of the country under the age of 18 years. However, almost 28% of adolescent girls get pregnant between the ages of 15 and 19 years, one of the highest rates worldwide.18 In 2013, the Government of Sierra Leone intensified its commitment to reducing adolescent pregnancies by launching the first national policy document “the National Strategy for the Reduction of Teenage Pregnancy in Sierra Leone”.19 This policy document continues to guide programs aiming at reducing adolescent pregnancies, for example, “Let girls be girls, not mothers”, through improving access to quality SRH and educational services for adolescents.19 Despite this, the use of modern contraceptives among sexually active adolescent girls remains low. A recent nationally representative study by Labat et al., found that over 40% of adolescents in Sierra Leone used neither condoms nor other modern contraceptives at their last sexual intercourse, indicating a high risk of unintended pregnancies and STI/HIV exposure.20
Factors which hinder modern contraceptive use among adolescents in sub-Saharan Africa include limited knowledge of modern contraception, low perception of pregnancy risk from unsafe sex, fear of side effects, religious prohibitions, and low education to understand the benefits and mechanism of modern contraceptives.3,6,21–25 In Sierra Leone, factors such as a female adolescent’s capacity to demand safe sex (i.e., male condom use), secondary or tertiary education level, and living in urban and wealthier households were associated with higher use of modern contraceptives.20,26 Little is known about the factors that have influenced the uptake of modern contraceptive use among adolescent girls in Sierra Leone over the years. Such evidence would guide the designing of effective interventions and strategies for increasing modern contraceptive use among adolescent girls.
The main goal of this study was to analyse the trends in modern contraceptive prevalence rate (MCPR) and modern contraceptive use among sexually active adolescent girls, 15-19 years in Sierra Leone using data from three nationally representative DHS surveys conducted in 2008, 2013, and 2019. Additionally, we aimed to identify factors that influence modern contraceptive use among this population by analysing data from the earliest (2008) and most recent (2019) surveys. A secondary objective was to assess the unmet need for family planning among adolescent girls 15-19 years in Sierra Leone across the three surveys.
METHODS
Data source and study design
We used data from 2008, 2013, and 2019 Sierra Leone Demographic Health Surveys (SLDHS). The DHS are nationally representative population-based cross-sectional surveys. In Sierra Leone, DHS is conducted by Statistics Sierra Leone with technical support from ICF International and provides crucial information on key health indicators such as contraceptive practices and fertility-related outcomes.26 DHS data collection mostly takes place every five years, and the most recent SLDHS was undertaken between May and August 2019.24 The SLDHS was collected using a stratified two-stage cluster design with primary sampling units (PSU, meaning geographic clusters) based on selected enumeration areas generated from Sierra Leone population census frames.26 Stratification was achieved by separating districts into urban and rural areas in the first stage. The enumeration areas were selected by probability proportional to the number of households in each province. The provinces were defined as Eastern, Western, Northern, and Southern in the 2008 and 2013 surveys but in 2019, the Northern province was restructured into the current Northern and Northwestern provinces. In each selected household, all females aged 15-49 were interviewed; the variables used in this paper are based on their self-report (of sexual activity and contraceptive use) or that of the head of household (household assets).
Study inclusion and exclusion criteria
The study population was defined as adolescent girls aged 15-19 years at the time of the survey who were residents in sampled households. The study samples consisted of 1,263 adolescents on the 2008 DHS, 4,051 on the 2013 DHS, and 3,460 on the 2019 DHS.
Study variables
Dependent variable
The dependent variable for this study was the use of a modern contraceptive at the time of the survey. Modern contraceptives included emergency pills, pills, female condoms, male condoms, diaphragm, injections, lactational amenorrhea, implant/Norplant, and intrauterine devices (IUDs).26 We defined the MCPR as the percentage of all adolescent girls aged 15-19 who reported using a modern method at the time of each survey. Unmet need for family planning was defined as the percentage of all adolescent girls 15–19 years who did not want to be pregnant not using a contraceptive at the time of the survey, in line with the DHS definition.26 The variable used to calculate unmet need for family planning in this study was v626, which is included in the individual recode dataset of the DHS surveys. Modern contraceptive use among sexually active adolescent girls was defined as the percentage of adolescent girls who reported sexual activity in the 12 months preceding each survey using a modern contraceptive at the time of each survey.
Independent variables
Independent variables for this study included sociodemographic factors and contextual/community factors. Four media sources (radio, television, newspapers or magazines and SMS) were used to assess the scope of exposure to family planning messages via mass media in the last month. This was grouped in terms of the number of media sources: none, one, two, three, and four. We also explored the most frequently used media sources, which we grouped as no media source, radio, television, newspapers or magazines, and SMS. SMS as a source was only in the 2019 SLDHS. The major sources of modern contraceptives are categorised as government/public health facilities, or pharmacy/private health facilities or other unspecified sources. This is inline with the DHS is defined as the most recent source of modern contraceptives among adolescents currently using modern contraceptives,26 except for adolescents on lactational amenorrhea method (LAM) which had no source, but a self-reported current use of LAM. Individual and contextual factors selected based on a review of the literature22,25,27 and the availability of variables on the 2008 and 2019 SLDHS are described below.
Individual factors
We considered the following individual characteristics of adolescent girls at the time of the survey: age in years, marital status (not married/separated/divorced or married/living with a partner), and the highest level of education (no education, primary level education and secondary or tertiary level education). Religion was coded as Christian or Muslim/others. We also categorized respondents’ ethnicity into Mende, Temne, or others, and time since last sexual intercourse into never had sex, less than 30 days, or more than 30 days. Adolescent girls who reported ever having had sex were grouped by the number of sexual partners in the past 12 months into: none (no sexual activity in the 12 months preceding the survey), and one, or more than one sexual partner. Parity had three categories: nulliparous, one child, and more than one child. An adolescent’s occupation was grouped into three categories and coded as: not working (includes studying), engaged in agricultural labour, and sales or other occupations.
Contextual factors
The place of residence was categorized as rural or urban, and into provinces (Western, Eastern, Northern, Northwestern, and Southern) as captured by DHS. We also used the household wealth quintile, which is a relative measure provided by the DHS and derived using Principal Component Analysis based on ownership of household possessions, type of housing, and water and sanitation facilities.26 Distance to the nearest health facility being a problem and permission to seek health services as self-reported by the respondent was coded as no problem, not a big problem or a big problem. In the context of DHS, the measurement of distance to the nearest health facility is subjective and prioritises the participant’s experience of the distance rather than an objective measurement. In the 2008 and 2019 surveys, however, there were just two options for distance to the nearest facility and permission to seek health services: no problem and a big problem.
Statistical analysis
Data were analyzed using Stata 17.0 (College Station, TX: StataCorp LLC, USA). Descriptive analysis of participants’ individual and contextual characteristics was first performed independently for each survey year and presented as proportions with their respective 95% confidence intervals (95%CI) or means with standard deviations. We calculated percentages and 95% confidence intervals (CI) for the MCPR, modern contraceptive use among sexually active adolescent girls, and unmet need for family planning, and produced a line graph for their trends across the three surveys, as well as a t-test to determine the difference between the surveys. We further examined the sources and method mix of the modern contraceptives used by adolescent girls.
Then, for the earliest and most recent surveys (2008 and 2019), we performed a bivariate logistic regression to examine the relationship between each independent variable and modern contraceptive use among sexually active adolescent girls, defined as having had sexual intercourse in the previous 12 months. The results were presented as crude odds ratios with associated p-values and 95% confidence intervals. Finally, for both surveys, we ran a multivariate logistic regression to see if the factors linked with current contraception use among sexually active adolescents changed over time.
Before fitting the multivariable logistic models for the two surveys, we used the variance inflation factor (VIF) method to assess multicollinearity within the independent variables. Variables with VIF ≥ 2, indicated multicollinearity28 and were excluded from the final model. We also performed a likelihood ratio test (LRT) for independent categorical variables with more than one category to identify the final model variables. A variable with an LRT P -value of ≥0.05 suggested evidence of a difference between the models with and without the variables, which were subsequently not included in the final model. Similarly, to examine the goodness of fit for our models, we employed the Hosmer-Lemeshow test to determine how well the independent variables fitted into the final logistic regression model. The Hosmer-Lemeshow test P values were ≥ 0.05, which was interpreted as our model being a good fit. All the analyses were performed at a 5% threshold and both crude odds ratio (cOR) and adjusted odds ratios (aORs) were reported with their 95% confidence intervals (CIs). The analysis of the data took into consideration the sample weights, stratification, and clustering inherent in DHS sampling by using the svyset and svy command packages in Stata 17.
RESULTS
The analysis sample included 8,774 adolescent girls aged 15-19 years in Sierra Leone from the three surveys (2008, 2013, and 2019 SLDHS). Table 1 summarizes the individual and contextual characteristics of the sample by survey. In all three surveys, almost 20% of the adolescents had one or more children. The percentage of adolescent girls who were married or living with a partner at the time of the survey declined from 27% in 2008 to 14% in 2019. Furthermore, most respondents reported having full autonomy in selecting whether to seek healthcare, with little to no constraints. However, several reported having problems with long distance to the nearest health facility. In terms of education, the percentage of adolescent girls who received no education declined steadily over time from 31% in 2008 to 16% in 2019. About 60% of the respondents in all three surveys had had sex in the year before the survey, with one-third of them reporting sexual activity in the preceding month; less than 6% on any survey had more than one current sexual partner. Knowledge of at least one modern contraceptive method increased from 65% in 2008 to 93% in 2013 and 95% in 2019. However, between 2008 and 2019, the number of adolescent girls who reported difficulties obtaining permission to seek healthcare increased by 17%.
Levels and trends in modern contraceptive prevalence over time and across regions
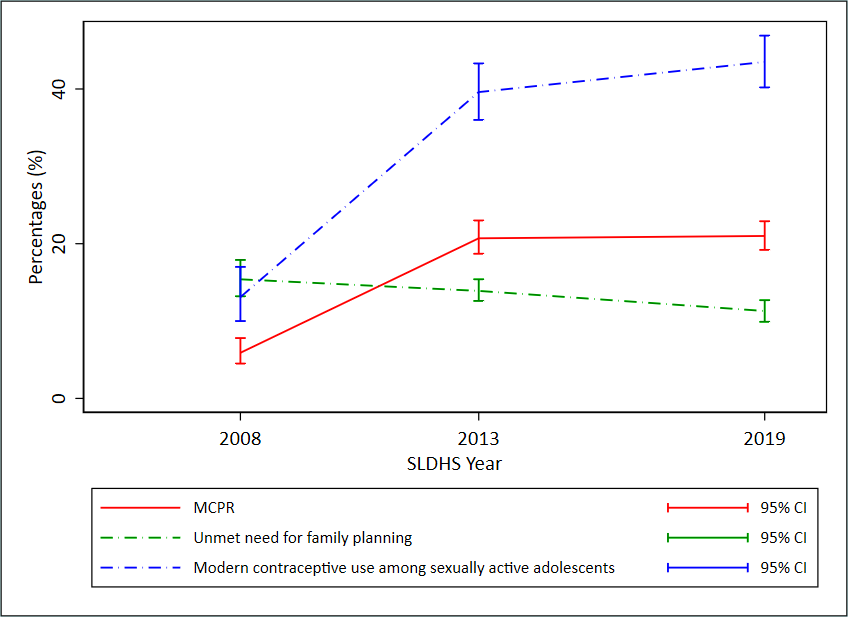
Since 2008, there was an increasing trend in the use of modern contraceptives (MCPR) among adolescent girls in Sierra Leone (Figure 1 and Table 2), P<0.001 between 2008 and 2013, but no evidence of a statistical difference between 2013 and 2019. There was a four-percentage point decline in the percentage of adolescent girls with unmet needs for modern family planning among all adolescent girls between 2008 and 2019, from 15.4% to 11.3%, and this change was statistically significant (P<0.001). The prevalence of modern contraceptive use among sexually active adolescent girls increased from 13.1% (95% CI=10-17.0) in 2008 to 43.5% (95% CI=40.2-46.9) in 2019, but notably stalled after 2013.
_and_unmet_need_for_family_planning_among_adolesc.png)
Modern contraceptives source and methods mix
Injectable contraceptives and implants/Norplant were the most popular modern methods among adolescent users of family planning in the 2013 and 2019 surveys, a notable change from 2008 when pills and condoms were much more common (Table 2). In 2019, 39% and 48.8% of adolescent girls reported using injectable contraceptives and implants/Norplant, respectively, compared to 2008 when 18.7% used injection contraceptives and none reported using implants/Norplant. A growing percentage of modern method users obtained their contraceptives from government health facilities (from 43.1% in 2008 to 82.8% in 2019). Contraceptive information via mass media mostly came through a single medium, with radio being the main media communication source across all the surveys. Most adolescents lacked access to media sources of contraceptive information and their exposure appeared to drop between 2008 and 2019.
Determinants of modern contraceptive use among sexually active adolescent girls in Sierra Leone
Table 3 provides a summary of the bivariate and multivariable logistic regression analysis of the association between modern contraceptive use among sexually active adolescents and several independent variables, for the 2008 and 2019 surveys. The bivariate analysis between parity and modern contraceptive use showed decreasing odds of contraceptive use with increasing parity in both the 2008 and 2019 surveys. In the 2019 survey, the adjusted odds of using modern contraceptives also decreased with increasing parity. The odds were lower for adolescents who had one child, aOR=0.62 (95% CI=0.45-0.85, P =0.003) and further decreased for those who had two or more children, aOR=0.43 (95% CI=0.20-0.94, P=0.034), when compared to nulliparous adolescents. This contrasted with the 2008 survey, where the adjusted odds of using a modern contraceptive method increased with increasing parity. However, the adjusted odds were not statistically significant, and the confounding was mainly due to effects of marital status and education level. This means that parity was not significantly associated with modern contraceptive use in 2008 but was significantly and negatively associated with the outcome in 2019. In both surveys, adolescent girls who were either married or living with a partner had lower adjusted odds of using modern contraceptives compared to those who were not married or cohabiting at the time of survey, aOR=0.38 (95% CI=0.26-0.55, P<0.001) in 2019. On the contrary, the adjusted odds of using a modern contraceptive were more than double among adolescent girls with two or more sexual partners compared to those with only one sexual partner, aOR=2.06 (95% CI=1.15-3.69, P=0.015) in 2019, and aOR=2.38 (95% CI: 0.91-6.23, P=0.077) in 2008.
In 2008, adolescent girls with secondary or tertiary education had approximately 8 times higher adjusted odds of using a modern method compared to those without any formal education. This disparity reduced in 2019; adolescent girls with primary education had aOR=1.03 (95% CI=0.63-1.70, P=0.902) higher adjusted odds of modern contraceptive utilization compared with those with no education, and those with secondary or tertiary education had twice higher odds of contraceptive use aOR=2.24 (95% CI=1.47-3.43, P<0.001).
There was evidence in 2008 but not 2019 that adolescents who accessed mass media information from one or more sources had higher odds of using modern contraceptives compared to those without access to any media. An adolescent girl’s occupation, region, and place of residence, religion, ethnicity, distance to the nearest health facility, permission to access health services and level of household wealth had no evidence of association with modern contraceptive use among adolescent girls 15-19 years (Online Supplementary Document).
DISCUSSION
This study estimated the trends of modern contraceptive prevalence rate (MCPR), and unmet need for family planning among all adolescent girls, and modern contraceptive use among sexually active adolescent girls in Sierra Leone. We further assessed the method mix and factors associated with modern contraceptive uptake among adolescent girls. MCPR nearly tripled between 2008 and 2019 from 5.9% in 2008 to 21% in 2019 but stalled after 2013. Similarly, there was little decline in unmet need for family planning among all adolescent girls, and less increase in modern contraceptive use among sexually active girls. We found that the method mix among users changed dramatically, from oral contraceptives being the most common method in 2008 to implants and injectables in 2019. Government health facilities have doubled the share of provision between 2008 and 2019 and were serving 8 in 10 of all modern method users in 2019. Multivariable analysis revealed that adolescent girls were less likely to use a modern contraceptive method if they were married/living with a partner or had one or more children. Adolescent girls who reported having sexual partners, were not married, or had attained a secondary or tertiary education level, on the other hand, were more likely to use a modern contraceptive method.
Our findings are consistent with studies from countries such as Guinea and Ethiopia which also experienced an increase in modern contraceptive use among adolescent girls across the DHS surveys.29,30 Nevertheless, countries such as Ghana instead had a decline in modern contraceptive use among adolescents for example between 2003 and 2014.31 The increase in modern contraceptive use across the three survey years are most likely a result of strong government and civil society push to end teenage pregnancy in Sierra Leone following the launch of a presidential initiative towards the same.19,32 Additionally, the 43.5% prevalence in modern contraceptive use among sexually active adolescents in Sierra Leone in 2019 is much higher than observed in other West African countries like Mali (17.1%) and Senegal (7.9%), and likely the highest in the region.
The improvement in modern contraceptive use is nevertheless still low and urgently needs to be further scaled to protect adolescent girls from unwanted pregnancies with its associated consequences. Given >95% of respondents knew at least one modern contraceptive method in 2019 and this knowledge increased dramatically from 65% in 2008, this can be leveraged upon to promote modern contraceptive methods use. Further efforts to delay the early marriage of girls and address cultural values and norms reported in past studies in Sierra Leone that act as barriers to modern contraceptive use among adolescents are urgently needed.20,33,34 Notably, the prevalence of the use of modern contraceptives has stagnated between 2013 and 2019. The limited progress made in reducing teenage pregnancy rates in Sierra Leone could be related to insufficient funding from the government, which could be partly due to the diversion of funds towards the Ebola pandemic response from 2013 to 2016.19 The pandemic had a devastating impact on essential health services, including contraceptive access, leading to a suboptimal implementation of the National Strategy for the Reduction of Teenage Pregnancy in Sierra Leone in subsequent years.19 An integrated approach that leverages funding from all sectors to promote health and wellbeing of adolescents could help address the funding gap.
The finding that married adolescent girls were less likely to be using a modern contraceptive method is consistent with a survey in Guinea and in the Democratic Republic of Congo which found that ever-married women were less likely to use modern contraceptives compared to those who have never married.29 This finding is not surprising, since married adolescent girls or those living with partners could be under various social or family pressures to have children soon after marriage, and thus low need for pregnancy prevention.35 We noted in this study a 17% increase in the number of adolescent girls having difficulty obtaining permission to seek health services indicating a reduction in autonomy. Structural factors such as poverty, and sexual coercion in Sierra Leone are known to limit adolescent girls’ autonomy in deciding when to get pregnant.20,33,36 Our finding nevertheless differs from surveys from Ghana, Zambia, and Uganda where adolescents who were married had a higher likelihood of using a modern contraceptive method.27,31,37
Adolescent girls with more than one sexual partner had higher odds of using modern contraceptives as compared to those with one sexual partner. This could be because adolescents with sexual partners could have a greater desire to prevent pregnancy alongside sexually transmitted infections/HIV thus using contraceptives. Additionally, the sexual partners could play a role in encouraging adolescents to use contraceptives, for example through financial support for purchasing contraceptives compared to the unmarried, as well as provide condoms.6,37 A similar finding was shown in a study conducted among adolescents in Nigeria.38
Adolescent girls with secondary or tertiary education had higher odds of using modern contraceptives than those with lower levels of education. Higher education status is associated with modern contraceptive use in other studies.3,30,37 This could be because women who have had secondary or tertiary schooling likely get more exposure to reproductive health information, and thus have more autonomy in making informed decisions about fertility choices, including the use of modern contraceptives.39 Although exposure to mass media was strongly associated with the use of modern contraceptives among adolescent girls in 2008, this was not the case in 2019. This is likely because just 27% of adolescent girls had access to mass media information in 2019 compared to 53% in 2008. Also, possibly the government could have reduced passing contraceptive information through the media, or fewer adolescent girls were accessing media sources such as radios and televisions. Better digital health solutions are needed to reach adolescents who may not be accessing mainstream media information.
Study limitations
This is the first study in Sierra Leone to analyze the trend of modern contraceptive use among adolescent girls aged 15-19 years. The utilisation of nationally representative data provided an opportunity for the generalization of our findings to all Sierra Leone adolescent girls aged 15-19 years. However, the cross-sectional nature of the DHS data limits analyses of causal relationships between the independent variables and modern contraceptive use.40 Additionally, most of the factors were based on self-reporting whereby we cannot rule out recall and social desirability biases.41 Also, besides marital status, all the independent variables associated with modern contraceptive use in this study had very high odds ratios and wide confidence intervals, which was likely a result of imprecision in the measurement due to small sample sizes. A further limitation is that we assume that adolescent girls who are not using modern methods but do not want to get pregnant have “unmet need” which may not be the case.42 Lastly, some variables such as the number of provinces and media sources have changed over time, making cross-year comparison impossible.
CONCLUSIONS
This study found that the modern contraceptive prevalence rate among adolescent girls 15-19 years in Sierra Leone more than tripled between 2008 and 2019, but it has stalled since 2013. There was no corresponding decline over time in unmet need for family planning. Adolescent girls were more likely to use a modern contraceptive if they had a sexual partner but were not married or living with a partner and or had attained secondary or tertiary education. Future interventions promoting modern contraceptives among adolescents should be holistic targeting sexual partners, primary schools, and communities to address barriers to modern contraceptive use. Interventions including increasing awareness and accessibility to modern contraceptives are urgently needed, particularly for adolescent girls without a formal education. Enhancing the provision of community-based and school-based contraceptive services could improve the use of modern contraceptives among underserved adolescent girls.
ACKNOWLEDGEMENTS
We acknowledge the Demographic and Health Surveys Program for availing the DHS data for this study, and further appreciated the adolescents in Sierra Leone who participated in the survey. We are further grateful to the organisers of the Institute Tropical Medicine, Antwerp DHS Summer Course in 2022, which was attended by the first author, and all the course organisers and coordinators for their guidance during the course.
ETHICS STATEMENT
A high standard of research ethics is observed throughout DHS surveys with further ethical approval sought from the country where the survey is conducted. Furthermore, informed verbal consent is also obtained for all respondents before data collection is conducted. Since the SLDHS is an openly available data source, no further ethical clearance was needed for this analysis except permission from the DHS programme team. The data set used for this study was obtained from the MEASURE DHS website.26
Availability of data and materials
The data set used is available upon permission from the MEASURE DHS website (URL: https://www.dhsprogram.com/data/available-datasets.cfm).
FUNDING
No funding was accessed for this study.
AUTHORSHIP CONTRIBUTIONS
EO conceptualized this study, conducted the data analysis, drafted the methods, and drafted the results section. FMG guided the data analysis and read through all the manuscript drafts. Also, LN and RN wrote the first draft of the background and discussion section, while DM, QS, CN, EI and LB reviewed all the drafts and made substantive contributions that helped reshape the manuscript. All authors contributed to and approved the final version.
COMPETING INTERESTS
The authors completed the Unified Competing Interest form available upon request from the corresponding author and declare no conflicts of interest.
CORRESPONDING AUTHOR:
Emmanuel Olal MBChB, MSc, [email protected] , Yotkom Medical Centre, Awich Road, Kitgum-Uganda, Orchid: https://orcid.org/0000-0003-3841-5896