
Achieving Universal Health Coverage (UHC) is a major global health policy priority.1 The World Health Organization (WHO) has defined UHC as ensuring that “all people have access to services of sufficient quality to be effective and do not suffer financial hardship paying for them”.2 Many economically-developing countries have introduced health insurance programmes in an attempt to achieve UHC.3–8 In Pakistan, efforts are underway to improve access to health care and achieve UHC.9,10
Khyber Pakhtunkhwa (KP), the North-Western province of Pakistan bordering Afghanistan, has suffered from decades of armed conflicts and natural disasters.11 The province had one of the highest out-of-pocket (OOP) expenditures on health care in the country.11 Against this backdrop, on 15 December 2015, the Government of Khyber Pakhtunkhwa (GoKP) launched a social health protection (SHP) initiative named Sehat Sahulat Programme (SSP). In six years (2015-2021), the population served by SSP grew from 2% (2015) to 100% (2020).
SSP had three stated objectives, namely: (i) improving access to health care, (ii) improving the quality of health services, and (iii) providing financial protection against health-related costs.12 The first objective of SSP, i.e., improving access to health care, is the cardinal feature of UHC.
Access is defined as the ability of people to utilise appropriate health care resources for preserving or improving their health.13 The four major aspects of access to health care are: availability (supply) of the needed services, affordability, controlling geographical barriers, and socio-cultural acceptability.13
Pakistan had a legacy mixed health system with the public, private and military hospitals providing care to people per their affiliation or ability to pay.14 The public sector, financed through annual budgets, was accessible to the general public.15 The private sector, largely financed through OOP expenditure, was not affordable for the poor.15 However, the public sector was not free either, as people had to pay for medicines and laboratory investigations.15 SSP is the first large-scale, publicly funded programme in Pakistan using a public-private mix for health care delivery.16
A key research gap relates to how this public-private mix affected access to health care in a system that predominantly worked on supply-side financing. In this paper, we describe the notion of access under SSP, present the stakeholders’ views on the access-related accomplishments and challenges of SSP and the way forward to realise SSP’s access-related objective in the broader context of its contribution toward UHC.
In a previous paper, we described SSP’s progress on the WHO’s UHC Box Framework.17 We further plan to publish our findings on two distinct dimensions of the programme in separate papers. In one paper, we will describe the role of the German Development Bank (as a policy entrepreneur) in the initiation and implementation of SSP to draw inferences for international development partnerships in promoting UHC. In another paper, we will describe the role of SSP in GoKP’s COVID-19 response and draw inferences for the potential role of SSP and similar programmes in promoting global health security.
METHODS
We employed an instrumental case study design approach. We selected SSP as an instrumental case to draw inferences for other insurance programmes launched by the Federal Government of Pakistan (Prime Minister National Health Programme [PMNHP]) and the provincial Government of Gilgit-Baltistan (Sehat Hifazat Programme [SHiP]). We selected SSP as a case study for two reasons: (i) SSP had the most comprehensive population coverage (covering 100% of the KP population), and (ii) the PMNHP and SHiP had replicated the SSP model in their respective geographical jurisdictions.
Data collection
Data sources
We used three data collection methods. First, we started with identifying and analysing the GoKP programme documents. Second, we undertook in-depth interviews, and finally, we undertook non-participant observations.
Timeline and ethics
We collected data from March 2021 to December 2021. We had ethics approvals from the University of Edinburgh (UK) and Khyber Medical University (Pakistan). We followed the ethical guidelines laid down by the ethics committees of both Universities. Written informed consent was taken from all participants, and data confidentiality was ensured.
Sampling and recruitment
We acquired the documents from the SSP head office and its official website(s) (https://sehatsahulat.com.pk/ and https://sehatcardplus.gov.pk/). The included documents were either authored or commissioned by GoKP, including Planning Commission Form 1 (PC-1) and the contracts.18,19 PC-1 is a standard template used for the planning and approval of all government project in Pakistan.
We used purposive (maximum variation) sampling for conducting interviews with stakeholders, including officials from GoKP, SLIC, SSP hospitals, patient advocacy groups and international development agencies. We recruited participants through direct (verbal or emails) and open invitations (displaying a poster at the stakeholder offices).
The maximum variation sampling was also used for collected non-participant observations. Observations were collected at the policy (meetings at the SSP head office in Peshawar) and the implementation levels (at SSP desks in hospitals). Hospitals in both sectors (public and private) at both levels of care (secondary and tertiary) were taken as case study sites. The SSP Director served as the gatekeeper and facilitated access to the meetings and the SSP desks.
Types of data captured
We used the programme policy documents to capture the chronology of events in SSP evolution and the changes in its policy parameters like the population, services and financial coverage. We used the tenants of Multiple Streams Theory (MST) to understand the problems and political discourse that led to the policy intervention in the form of SSP.20
MST informed our sampling strategy. Through stakeholder interviews, we explored the notion of access under SSP; the changes brought in access to health care, the practical implications of the changes and the future directions to harness SSPs’ role in achieving UHC. In the non-participant observations, we explored how the SSP policy decisions were made at the policy level and how they were (or were not) translated into practice at the implementation level. Topic guides were used to conduct interviews and collect observations.
Data analysis
We conducted thematic analysis of the data with the help of NVivo 12. The MST informed our initial coding framework and major themes.20 We refined the initial theory-informed coding framework and themes through repeated iterations of the data analysis. The ongoing analysis informed our ongoing data collection. We stopped data collection when data saturation was achieved. Finally, 20 documents (Appendix 1), transcripts for 62 interviews (Appendix 2 – Table 1), and 63 hours of observations (Appendix 2 – Table 2) went into analysis.
MST helped us tease out the problem and policy streams that led to SSP initiation and how SSP affected access to health care. New problems like geographical barriers and acceptability were highlighted during the policy level data collection. It led to expanding our enquiry to cover the implementation barriers and their potential policy solutions.
Reflexivity
One author (SAK) worked at SSP for a couple of years (2017-18) and left the programme to pursue his Ph.D. His previous affiliation with SSP helped us with the data collection but posed the risk of biased data interpretation. The co-authors (KC and AS) consistently reminded SAK of his potential biases and helped minimise subjectivity in data analysis, interpretation, and reporting through their constant feedback. This reflexivity enabled the primary author (SAK) to update his earlier stance of considering SSP akin to UHC and enabled us to write on the programme’s strengths and weaknesses in improving access and contributing toward achieving UHC in the province.
Strategies for validation of findings
We adopted four strategies for validation of our findings. First, we corroborated our findings by triangulation of data sources. In the findings, we have described where convergence or diversion of narratives was noticed between the programmatic documents and interviews.(133,150). Second, we generated thick descriptions during data collection (135,157), which helped the analysis. Third, we (all three authors) had regular debriefings in our group on the research process. Through these deliberations, we selected themes and concepts strongly grounded in our data and dropped findings with weaker support.(132,156). Lastly, we tried to achieve validity through reflexive writing.(132). With a clear understanding of our standpoints, we were able to highlight the strengths and the weaknesses in the programme’s evolution.
RESULTS
Description of purchaser-provider arrangements
The PC-1 underlined GoKP’s intentions for SSP to reduce OOP expenditure, protect against catastrophic health expenditure (CHE), break the disease-poverty cycle, and fulfil the state’s responsibility in ensuring access to healthcare.18 GoKP had designed SSP as an insurance programme and engaged SLIC as the insurer. The insurer had service level agreements (SLA) with public and private hospitals.19 Under the SLA, the hospitals were obliged to provide treatment to SSP patients. The hospitals having contractual arrangements with SLIC were called ‘panel hospitals’, and the processing was called empanelment. The insurer paid the providers for their services as per the package rate. The package rates were pre-defined bundled payments, including all the expenditures incurred during a patient’s hospital stay.
The SSP model was entirely different from the supply-side arrangement, where the hospitals received an annual budget in advance. Under the supply-side arrangements, patients would make an upfront payment in the private sector, OOP, to get services. The programme officials described SSP as a cashless arrangement, sharing that “money did not change hands” at the point of service. The SSP official claimed that people who used to “forgo care” could now find health care affordable.
Affordability of health care services
The PC-1 document showed every enrolled family had a financial allocation of 600,000/- Pakistan Rupees (PKR) per annum (equivalent to 2,489 Great Britain Pounds [GBP]). If admitted to a hospital, SSP covered secondary care services of up to PKR 200,000/- (GBP 830) and tertiary care services of up to PKR 400,000/- (GBP 1,659) per year. GoKP paid PKR 2850/- (GBP 12) per family per year to SLIC as a premium against this coverage. According to GoKP officials, the non-affordability of health care services was a significant access barrier; addressed by SSP:
“The primary reasons behind starting the programme was non-affordability of accessing health care…if you visit a government hospital, there are certain expenses that one has to bear”. [11: Health system strengthening specialist working at a development agency]
There was a consensus among the respondents that widespread poverty necessitated SSP. The GoKP and SLIC officials labelled the high OOP and CHE as “health shocks” that pushed people into poverty. The programme PC-1 described the disease-poverty nexus as one basis for launching the programme.
“…health risks pose the greatest threat to their lives and livelihoods…54 % of health shocks contribute to the poverty of the community”. [PC-1]
The GoKP and SLIC representatives stressed that many people incurred CHE and went into debt, noting that CHE was an important factor in impoverishment. SSP, per the GoKP officials, has broken the disease poverty nexus.
“…the Government thought, why not to insure the people against CHE. It was to improve the poverty index of the poor and the marginalised segments of the population”. [4: SLIC manager]
The developmental partners shared the view that SSP was to protect the poor and vulnerable against health costs and prevent worsening poverty:
“The basic driving force was to protect the poor from becoming ultra-poo”. [13: A senior GoKP official]
An insurance representative called SSP a “universal catastrophic health coverage”, but the advocacy groups challenged this notion as they considered treating chronic conditions on an outpatient department (OPD) basis equally catastrophic. Another insurance official called it “Universal Inpatient Catastrophic Coverage”, but a senior GoKP official disagreed because SSP spent billions of rupees on secondary care, which did not cause any CHE. Given these tensions, a senior GoKP official opined that the coverage argument of the programme was contradictory:
"Unfortunately, the programme is trying to cover a little this thing and a little that. There are no cohesive thinking or sound policy assumptions behind the programme.[14: A tertiary care public sector hospital manager]
The patient advocacy groups also viewed the programme strategy as lacking cohesion. To support their position, they referred to treatment for Hepatitis. The PC-1 and contract documents showed SSP covered Hepatitis B and C complications and liver transplant, but did not cover the primary treatment for Hepatitis.18,19 The advocacy groups criticised this “wait till it gets worse” approach.
“The GoKP recently announced it would cover liver transplants under SSP. Our argument is, why not prevent the leading causes of liver cirrhosis? Why not control Hepatitis B and Hepatitis C? That is cheaper and more effective”. [22: Representative of a patient advocacy group]
Similarly, SSP did not cover mental health illnesses. The insurance representatives claimed that mental health illnesses needed “lifelong treatment and were not insurable” medical risks. They shared that including mental health illnesses would affect their solvency. On the contrary, a hospital manager confronted the insurance representatives (as observed in a policy level meeting), positing that coverage for acute psychosis or clinical depression would not make the company [SLIC] bankrupt. He suggested that the programme should at least cover the “acute phases” of the illnesses that required hospitalisation.
Availability of health care services
The GoKP-SLIC contracts enlisted more than 1,200 medical conditions and surgical procedures covered under SSP, including liver and kidney transplants. But whether these services were available throughout the province of KP was contested. For example, a development partner shared that SSP did not sufficiently address the availability aspect of access, noting that the health system lacked trained human resources and their equitable distribution. When asked if SSP could contribute towards achieving UHC, he said:
“UHC is a big notion, entailing many prerequisites. One cannot dream of UHC by only providing the public with Sehat Sahulat Card”. [13: A senior GoKP official]
GoKP and SLIC officials suggested that SSP improved the availability of health services as it brought the private sector capacity on board. However, a public hospital manager contested the claim:
“…the entire private sector operates with the human resource from the public sector…I think the programme had brought no additional human resources and would rather make the public sector weaker while its human resources are moonlighting in the private sector”. [14: A tertiary care public sector hospital manager]
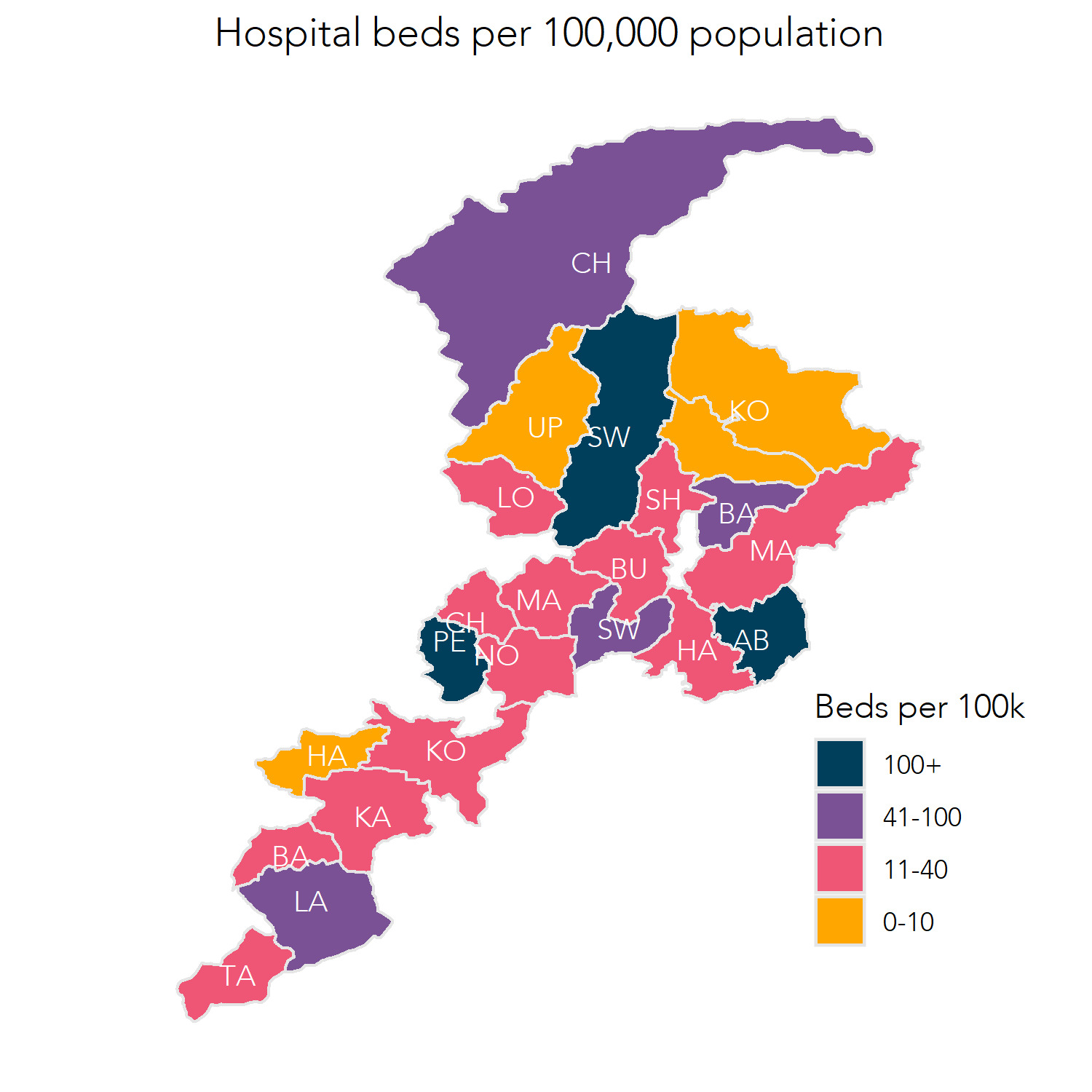
Insights into the bed-per-population ratio in the SSP panel hospitals went against the claims the programme had improved availability. Figure 1 shows the distribution of the total bed capacity of the SSP panel hospitals with the district-wise population across KP. The figure highlights a wide variation in the number of beds in the SSP panel hospitals in different districts. For example, hospital beds per 100,000 population in Peshawar and Swat were 10 times higher than beds for an equal population in remote districts of KP like Hangu and Kohistan. “Beds availability in SSP hospitals per 100,000 population” as shown in Figure 1.
Based on our analysis of the data available on the SSP website, interviews and field observations, the availability of the services had four scenarios:
1. Not available, not accessible
Despite SSP coverage, essential services were unavailable and, hence, not accessible in some areas. For example, a SLIC representative highlighted the lack of cardiologists in Kohistan, Tor Ghar, and Shangla. This lack of availability affected the utility of the financial protection SSP had conferred. Similar trends were reported for cardiac surgery:
“We got limited options in cardiac surgeries in KP. We have lots of cardiology hospitals, but surgical options are limited, so we refer patients to Lahore and Islamabad”. [5: SLIC manager]
2. Available but not accessible (kept out)
In other places, clinical services were available, but SLIC did not procure their services for cost considerations and hence not available to people. A paediatric surgeon in a private hospital shared:
“I have suggested various effective and lifesaving surgeries, like correction of biliary atresia, to the insurer for inclusion in SSP but to no avail. The rates they offered were not practical for us”.[47: a specialist surgeon from a private hospital]
In hospitals where services, e.g., paediatric surgery were available but not contracted by SLIC, untapped potential to further improve access was there.
3. Available, but not accessible (opted out)
Some hospitals reported that their senior clinicians with a good patient flow opted out of SSP. They considered the SLIC package rates incommensurate with their experience. The insurer labelled it as a matter of choice and not a fault in their service pricing:
“Dr XXX is a very expensive neurosurgeon, and it is his personal choice whether he wants to work with the insurance programme or not…We have given patients the choice of hospital, but they do not choose any individual doctor”. [6: A senior manager at the insurance company]
SLIC officials considered the senior clinicians’ opt-out a non-issue. Still, the hospital managers gave a grim interpretation, stating that the unacceptable service pricing led to mushrooming private hospitals running in rented buildings where trainee surgeons operated on the patients. However, we [the researchers] could not verify if these claims were valid.
4. Available, accessible, but not working
The programme did not work in some places due to a breakdown in the supply chain of essential medicines and implants. A cardiologist working in Hospital X reported that despite the available expertise and patients’ affordability (insurance coverage), patients could not access the needed services as they were out of stents.
“Cardiac stents and pacemakers are expensive…I used my leverage with the suppliers to provide these things on credit to the hospital for the SSP patients…Sate Life delayed paying the claims, and the hospital could not honour its word given to the suppliers. They discontinued”. [10: A cardiologist from a public tertiary care hospital]
Though the programme claimed it improved services availability, the documents did not have any indicators to back these claims. On the contrary, a development partner doubted the service’s availability for a lack of human resources for health (HRH). He highlighted that the HRH index in the province was less than 2%, against the 4.5% recommended by WHO. Therefore, he argued that people might not access health services despite having insurance coverage.
“You are creating demand by giving Sehat Sahulat Card and social protection, but what are we doing on the supply side?…You ask people to avail of the services in your empanelled hospitals…but who will ensure the availability”. [11: respondents from a development agency]
Geographical accessibility of health care services
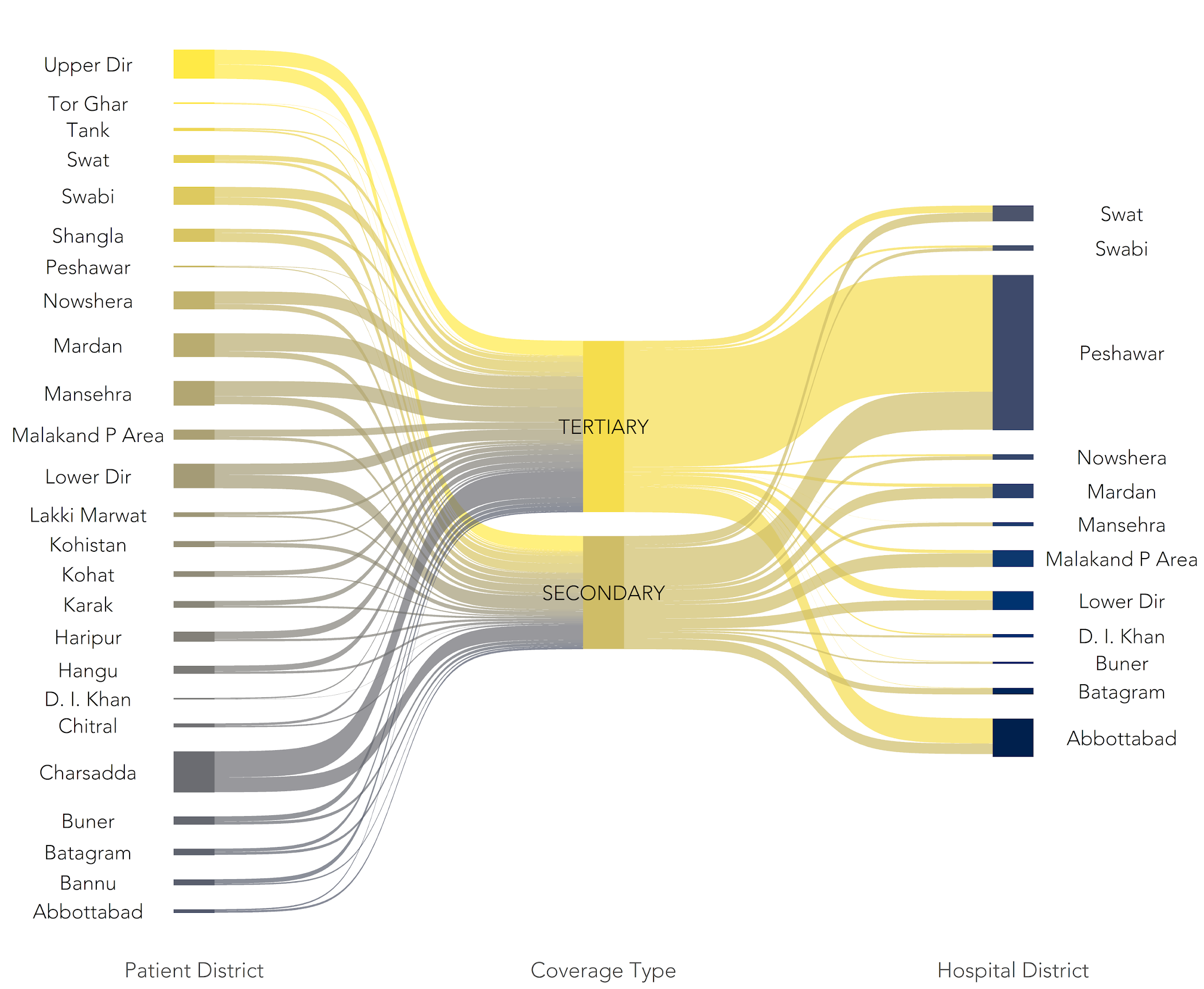
The KP health policy referred to geographical barriers as one reason for inequitable utilisation of health services. Figure 1 above shows the inequitable distribution of services’ availability. The programme officials thought utilisation would be equitable and pinned their hopes on coverage portability. Per the SSP policy, coverage was portable, i.e., patients could seek care in another district if their district did not have the facilities. There was a considerable geographical movement of patients towards a few developed districts like Abbottabad and Peshawar, “Inter-district patient movement stratified by type of services” (Figure 2). The implementation level staff reported a “worsening workload” in the receiving districts.
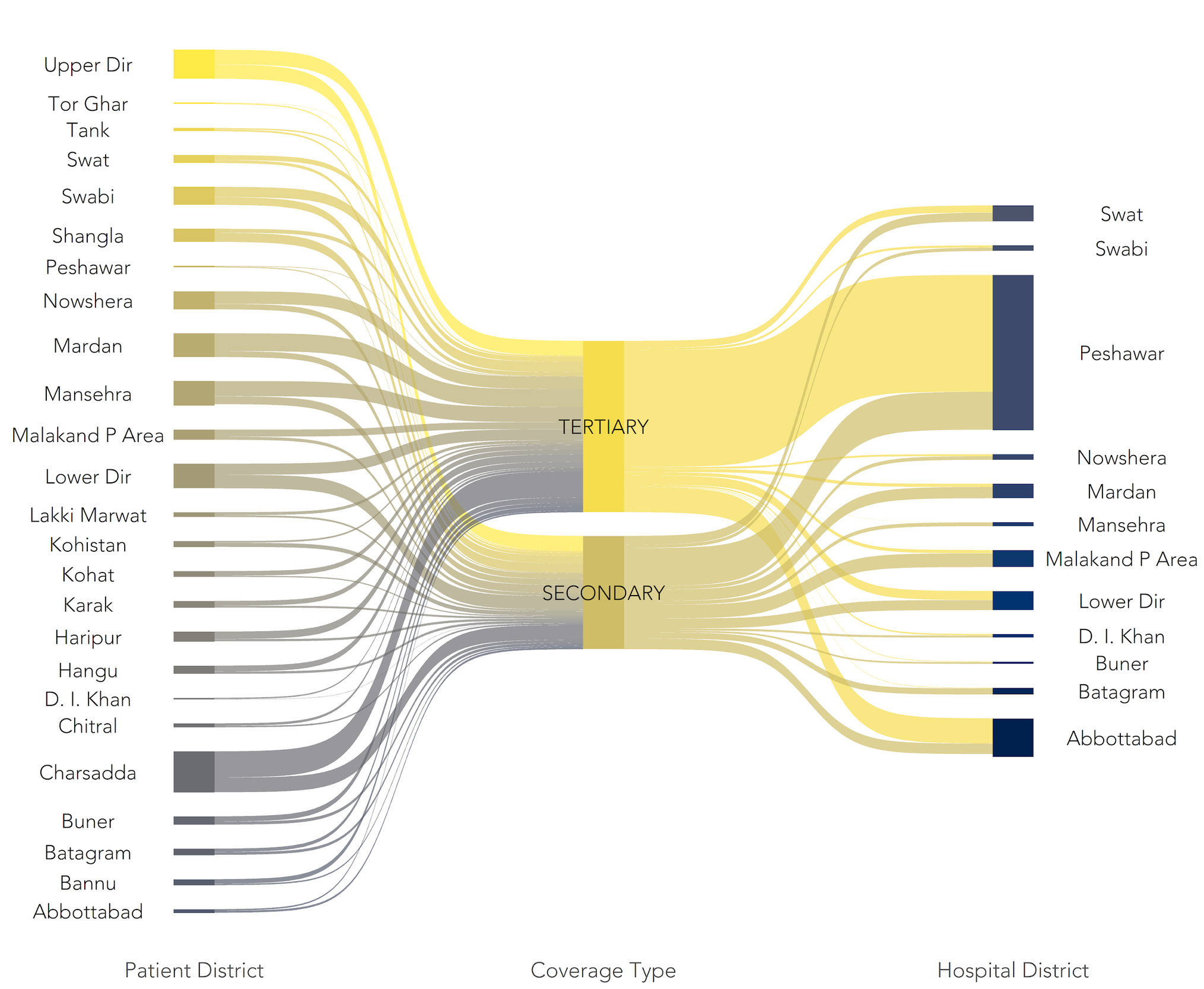
The SLIC officials suggested that Peshawar, the provincial capital, received many referred cases for lack of expertise and resources in peripheral districts. SSP officials informed that cancer care and cardiac surgeries were exclusively performed in Peshawar. The insurance staff called it “a run on the hospitals” in the provincial capital (Peshawar), because hospitals in other districts were not as developed as were in Peshawar.
“The programme has expanded faster than the health system could grow…I think the private sector has responded faster than the public sector regarding geographical coverage and availability of technology and services”. [26: SLIC representative]
There were, however, positive developments on this front. A respondent from the only cancer hospital on the panel informed their sister institutions (Pakistan Atomic Energy Cancer Hospitals) were getting empanelled and hoped to redistribute the patient load.
The programme officials informed that certain services like liver transplants were not performed in the province. So, hospitals in the federal capital Islamabad and the provincial capital of Punjab, i.e., Lahore, were considered for empanelment. Hence, the programme was perceived to have addressed the financial barriers, but geographical barriers persisted. The advocacy groups highlighted the added cost and logistical challenges of seeking distant care.
SLIC officials presented portability as a positive attribute to facilitate the patients, but some hospital respondents considered it “cost-saving efforts” by the insurer. An insurance manager had provided clues to that effect, saying that they got better prices for cardiac services in Islamabad than in KP.
“We refer patients to Islamabad. There, competition is tough between companies…Our CABG rate is PKR 400,000, and in Islamabad, it can be done within PKR 300,000 because of competition and higher patients flow. We have many cardiology hospitals, but surgical options are limited, so we refer patients to Lahore and Islamabad”.[5: SLIC representative]
Acceptability of health care services under SSP
Acceptability, i.e., the extent to which the SSP service providers and users considered it appropriate, had varied. During the interviews, the GoKP officials called SLIC the best fit to implement SSP for its financial muscle and the public sector identity. On the contrary, the advocacy groups claimed that a public sector insurance company would worsen the inefficiency of public sector hospitals. Hence, doing it through a public sector insurer, in their view, was a bad choice. Similarly, hospital managers showed disappointment with SLIC for risking the services quality, gate closing behaviour, mismanaging the public-private mix and adding complexities to the system. The issues will be further explained in the following subheadings.
1. The quality paradox
GoKP officials hoped the public-private competition would make the public sector competitive and improve service quality. The hospital officials, however, did not share this optimism. Hospital managers and SLIC officials suggested that instead of improving the public sector, private hospitals might see paradoxical deteriorations in service quality. Two possible hypotheses were given for the paradoxical changes: (i) the tertiary care private hospitals might compromise quality to stay competitive, said a SLIC official, and (ii) senior clinicians in the private sector had opted out of SSP due to low package rates.
Hospital managers suggested their senior clinicians had plentiful patients “willing to pay” their preferred fee, compared to the meagre charges offered by SLIC. The advocacy groups believed the opt-out deprived SSP patients of experienced clinicians, and a ‘for poor’ and ‘for rich’ private sectors emerged, potentially affecting the programme’s acceptability.
2. Gate-closing instead of gatekeeping
SSP counters in the hospitals were to do gatekeeping, i.e., prevent ineligible admission. The hospital managers called it “gate-closing,” i.e., preventing eligible admissions for emergency patients in the evening and night shifts:
“…The insurance staff is available from 9 am to 5 pm, and we need them from 5 pm onwards too. We can provide emergency services on the night shift if the insurance staff is deployed”. [38-a private hospital manager]
The hospitals’ managers strongly criticised the closure of SSP desks after 5 PM and demanded that they should have access to the insurance database for verifying the entitlement of emergency admissions. The insurer was not keen on providing this access, stating data confidentiality. The “gate-closing” might negatively affect the program’s acceptability, said a financing expert.
“Insurance is an experience product. If a client has a negative experience with insurance coverage, it is less likely that they would ever use it again. On the contrary, they might also discourage others from using it”. [39: A health care financing expert working at a development agency]
3. Mismanaging the public-private mix
The insurer reported that the public sector had shouldered high-prevalence and high-cost diseases like cancers at reasonable rates. The low service charges of cancer care in the public sector led to excluding the private sector from cancer care, said a SLIC official. The public sector cancer hospital likely benefited from the private hospital’s exclusion.
“This is a win-win situation for the hospital, the federal and provincial governments, and the patients. I believe this is a game-changer”. [17: A manager at the public sector cancer hospital]
Contrary to the GoKP and the insurer’s view, the private sector saw public hospitals as serving the insurer’s interests, potentially impacting the acceptability. The private sector called out the long waiting periods that served the interest of the insurer rather than the public.
“I understand the insurer’s incentive to shift cancer or renal transplant patients from the private sector to an underperforming public sector. They have to cut costs, no matter what. However, I do not understand why the government agrees to such short-sighted overtures of the insurer?” [32: A private sector representative]
A private sector representative argued that over-reliance on the public sector would negatively affect the programme’s acceptability, fearing higher infection-related mortality and deaths from cancer treatment in the public sector:
“Patients die more frequently from infections or electrolyte imbalances than the primary disease in cancer care. The public sector hospitals are the hubs for the spread of infections and treatment-related complications. Yet, all the cancer cases are sent to the public sector”. [9: A private sector representative]
4. SSP added complexities to the system
SSP made more hospitals available to the public, but it added complexities to how the hospitals operated. Hospitals, especially the public sector, had poor record keeping. Working under the SSP increased the documentation manifold.
“Our core clinical staff is required to fill the insurance forms and documentation. With their workload, they cannot meet the insurance documentation requirements.” [14: A tertiary care public sector hospital manager]
Similar views were shared by another manager whose hospital had 14,00 beds and had 400 admissions and discharges on average daily. He suggested the hospital did not have the resources to complete the insurance documentation.
“I cannot send them all the records and provide care to the patient at the same time. Therefore, patient care will continue, but the hospital will not get paid for its services”.[7: A public sector hospital manager]
This would inevitably lead to OOP expenditure, despite being an SSP beneficiary. That would affect the programme’s acceptability, said an advocacy group representative. The documentation was a burden on the private sector hospitals as well. However, their managers actively advocated for an e-claims system, whereby most of their treatment-related documents could be transmitted to the insurer from their hospital management information systems.
“I see merit in making our information systems integrated. For example, why do we need separate entries for the same patients in the hospital and the State Life systems?”[9: A private sector representative]
Additionally, several hospital managers suggested that a lack of awareness about SSP put pressure on the hospitals to provide care and educate the people. The lack of information on the benefits package and admission procedures led to the refusal of services, as was noted during the hospital-based observations, potentially reducing the programme’s acceptability among those with such negative experiences.
DISCUSSION
Summary of the key findings
In line with its objective of improving access, stakeholders suggested SSP has largely improved the affordability dimension while the availability of services was still a challenge. Geographical inequity in services’ readiness remained a major challenge. Lastly, the providers highlighted several implementation barriers (i.e., insurer’s limited working hours, excessive documentation and absence of e-claims systems) at the insurer’s end, which they considered detrimental to the programme’s acceptability.
Interpretation in view of the broader literature
The SSP objectives of access, quality and financial protection reflect the core tenants of UHC.18 WHO defines UHC as ensuring that “all people have access to services of sufficient quality to be effective and do not suffer financial hardship paying for them”.2 SSP, however, has taken a limited finance-centric approach to access and UHC. Studies have reported that affordability was important for improving access to health care but not sufficient.21
Affordability is the financial ability of people to use the services they need.20 Services are affordable if their use does not impose financial hardships.22 The SSP officials claimed they had covered CHE, but CHE on an outpatient basis was excluded. However, most of the OOP in Pakistan was reported on outpatient care.15 At the same time, SSP covered hundreds of secondary care procedures, which did not cause CHE.
In KP, each family has financial protection of up to PKR 600,000/- per annum, but how it is allocated is important. The population needs and epidemiological profile should determine the financial allocation and the benefits package.21 For example, in Pakistan, 4.8% of the population has Hepatitis C, making it the second-highest prevalence globally.23 Instead of providing coverage for direct antiviral therapy, SSP offered liver transplants. Here, politics had overridden an economically sound policy approach, as one of the study participants shared. Like Seguro Popular in Mexico, translating financial coverage into effective utilisation remained a challenge for SSP.24
The programme officials claimed that SSP improved service availability by adding private sector hospital beds. Availability exists if the inputs like buildings, equipment and personnel required to produce these services are in place.22 Availability is gauged by indicators like the number of physicians or hospital beds for a potential user population.20 The programme did not report on standard availability matrices like the HRH index or physician-to-population ratio. Overall, the national HRH density is very poor, with only 0.9 physicians (compared to 1.5 in Iran and 5.4 in the UK) and 0.6 nurses and midwives (compared to 1.6 in Iran and 9.8 in the UK) per 1,000 population compared to 0.8 at the national level.25 Without HRH, the affordability dimension might not translate into effective coverage.26
Access to services had a large geographical gradient under SSP. This geographical barrier might affect the patients’ willingness to seek care. Geographical accessibility is the fit of spatial or geographical relationship between the health care provider and users. The availability and geographical barrier might also affect the programme’s acceptability.22
Acceptability is the population’s willingness to seek care.22 It is determined by the ease at which a patient could visit a health care facility.13,20 We have seen that people had to travel long distances for tertiary care under SSP. Acceptability is the users’ attitude towards the service providers and vice versa.20 Considering the senior clinicians’ opt-out, it could be assumed that SSP patients were not acceptable to them. On the other hand, many patients had forgone SSP coverage to get treatment from their preferred specialists. The programme needs to investigate these developments further.
Acceptability is based on the users’ perception of the quality and effectiveness of the services and other socio-cultural considerations like religion, sex and ethnicity.22 Studies suggest that patients were satisfied with services provided under SSP.27,28 However, many who could not get services under SSP for various implementation barriers might have different views.27 Patients who incurred OOP while using SSP had affected their acceptability for the programme.27 The insurance company’s pricing, claims processing, limited working hours and gatekeeping approaches were reported as very off-putting by the hospital managers.27
The implementation barriers reported around SSP and the PMNHP were not unique to Pakistan. Similar problems have been reported with the Pradhan Mantri Jan Arogya Yojana in India.29 This could be due to the common roots of the health system in Pakistan and India. In Pakistan, the health insurance programmes have marked a transition from the supply (Beveridge) to the demand side (Bismarck) financing model.14,30 In this transition, the gatekeeping model should be changed from policing to a handholding approach. This could enhance the programme’s acceptability and improve access to health care as envisioned under SSP.27,31
Strengths and limitations
The qualitative nature of our enquiry, theoretically informed sampling and using multiple sources of data were the key strengths of our study. We were able to use the programmatic documents and interviews in a complementary manner to understand the access-related achievements and challenges facing SSP. The qualitative nature of our work enabled us to include more participants once we realised in the policy level interviews that access-related challenges were reported with the hospital-based implementation of the programme.
The qualitative nature of our enquiry had limitations as well. For example, our study highlighted the inequitable distribution of health care resources in KP, but we could not ascertain if it resulted in inequitable utilisation [geographical, age or specialty-wise differences]. We did not find any work done by other researchers on this aspect either. Future studies should leverage the SSP utilisation data to see if the inequity at the input level contributed to inequity at the output or outcome levels.
CONCLUSIONS
If taken in a narrow affordability-centric approach, SSP has considerably improved access to health care. However, much needs to be done in broader terms of availability, geography, and acceptability. Improving access to health care is the core objective of SSP, but the programme lacks sensitive and specific indicators to measure its progress. Therefore, SSP and other programmes working in other provinces of Pakistan need to adopt or adapt standard, internationally comparable indicators for measuring its impact on improving access.
A key lesson for policymakers at home and abroad is that interventions like SSP alone should not be expected to improve access. These initiatives could make services affordable. But first, services need to be made available, within geographical reach and acceptable to people. Therefore, while introducing demand-side interventions in mixed health systems, it is imperative not to ignore the supply-side elements. Instead, health care financing reforms should go hand-in-hand with other health systems strengthening interventions.
Taking affordability akin to access poses the risk of taking attention away from essential health system strengthening activities. While counting on initiatives like SSP to contribute towards UHC, it is imperative to employ systems thinking. Piecemeal thinking means the overall goals of access and UHC remain elusive.
Acknowledgements
We acknowledge the SSP Director for supporting our work and thank Mr Raheel Shahab for developing the figures used in the paper. We also thank the publisher for fully waiving the article publication charges.
Disclaimer
Our work does not include any potential identifiers of our participants, and we had the consent of the participants to publish our work based on their participation. We did not use any copyrighted material in this paper.
Ethics statement
We had ethics approval from the Ethics Committee at the University of Edinburgh and local ethics approval from the Khyber Medical University. We have complied with the ethics regulation of the approval bodies at all stages of the research and have maintained a written record of informed consent for the study participants.
Data availability
The datasets used and analysed during the current study are available from the corresponding author on reasonable request.
Funding
The work was made possible through a PhD funding from the Higher Education Commission of Pakistan. The funder did not influence the study design, data collection, analysis or reporting.
Authorship contributions
SAK developed the research plan and led the data collection, analysis and write-up. KC and AS contributed to refining the study design advised on the data collection, analysis, and interpretation, and helped refine the manuscript. All authors read and approved the final document
Disclosure of interest
The authors completed the ICMJE Disclosure of Interest Form (available upon request from the corresponding author) and disclose no relevant interests.
Additional material
The appendices are attached as online supplementary documents.
Correspondence to:
Sheraz Ahmad Khan
Usher Institute, the University of Edinburgh,
Teviot Place, EH8 9AG, Edinburgh.
Email: [email protected]
Phone: (+92) 333 9233 757.
(+44) 0745 99694083