Breastfeeding has many benefits for women and their children. Breastfeeding enables infants to experience nutritional and developmental advantages that enhance their health and developmental milestones.1 Breastfed babies have stronger immune systems, less diarrhoea and constipation, and fewer respiratory and ear infections.2,3 Breastfeeding is also associated with improved cognitive outcomes and children’s social and emotional development.4,5 Regarding long-term benefits, breastfeeding has also been shown to be protective against mental health problems that children may experience in adolescence.6,7 Additionally, breastfed babies grow into adolescence and adulthood with fewer risks of allergies, type I and II diabetes, and obesity. Pertaining to maternal benefits, breastfeeding aids in postpartum involution of the uterus and returning to pre-pregnancy weight and lowers lifetime risks of breast and ovarian cancers and cardiovascular disease.3 The World Health Organization (WHO) and the United Nations Children’s Fund (UNICEF) recommend exclusive breastfeeding for the first six months of life and then, introduction of nutritionally adequate and safe complementary foods at six months, together with continued breastfeeding up to two years of age or beyond.8
Despite evidence on the proven benefits of breastfeeding and international recommendations, suboptimal breastfeeding practices continually undermine achievement of maternal and child health goals globally.9 Notwithstanding breastfeeding of infants is commonly acceptable in sub-Saharan Africa10 and three decades of promotional efforts, exclusive breastfeeding rate in the region remains low (37% in 2017).11 In Nigeria, which has one of the highest rates of malnutrition among children in the world,12 the rate of exclusive breastfeeding of infants <6 months of age was 29% in 2018; the rates of continued breastfeeding at 12 and 24 months were 83% and 28%, respectively.13
There is consensus in the literature that factors such as maternal age, gestational age at childbirth, parity, education level, socioeconomic status of the mother and household, mode of childbirth, age of the child, skilled antenatal and childbirth care, and traditional beliefs influence a woman’s decision to initiate and continue breastfeeding.14–16 However, there is inconclusive evidence on the association between IPV and breastfeeding; some studies identified statistically significant associations,17–19 while others did not.20–22 A study conducted in twenty-six states in the United States of America reported that initiation of breastfeeding was less likely among women who experienced IPV in the year prior to pregnancy, during pregnancy, and during both periods. Women who reported IPV during pregnancy were more likely to stop breastfeeding by four weeks postpartum.17 A study from Brazil also showed that women exposed to severe physical violence by an intimate partner were more likely to cease exclusively breastfeeding than their counterparts.19
On the contrary, a study from the United States reported that there was no difference between the proportion of breastfeeding among women who experienced IPV and women who did not.20 A study among Swedish women showed that IPV did not influence breastfeeding prevalence or duration of breastfeeding up to twelve months.22 Other available studies examined the association between IPV and exclusive breastfeeding in the first six months of life19,23–26 and one study up to the age of twelve months.22 These, however, did not account for complementary infant feeding practices beyond six months of age. The first two years of a child’s life are very significant, as optimal nutrition at this period lowers morbidity and mortality, reduces chronic disease risk, and fosters better development overall.8
IPV can take various forms as physical, sexual, and emotional violence. If women are exposed to IPV while breastfeeding, the physical, mental and emotional consequences may impair childcare practices, including breastfeeding.27 In Nigeria, one in three ever-married women was reported to have ever experienced physical, sexual, or emotional IPV.13 In a study in Nigeria that assessed the relationship between experience of IPV and exclusive breastfeeding using data from the 2018 Nigeria Demographic and Health Survey (NDHS), IPV was found to be a risk factor for suboptimal exclusive breastfeeding.28 Our study aims to explore the relationship beyond the first six months of life. In our study, we examine the association between recent maternal experience of IPV and optimal infant and young child breastfeeding practice of children 0 to 23 months in Nigeria. The findings of this study will add to the existing knowledge base on the link between IPV and breastfeeding practice.
METHODS
Data source
We used data from the Nigeria Demographic and Health Survey (NDHS) 2018. Demographic and Health Surveys (DHS) are nationally representative household surveys that provide data on a wide range of key indicators in population, health, and nutrition.29 Standard DHSs have large sample sizes of 5,000-30,000 households and are typically collected every five years.29 The 2018 NDHS is the sixth and most recent DHS conducted in Nigeria.30 Data were collected between 14 August 2018 and 29 December 2018.13
Sampling design
The 2018 NDHS used a two-stage stratified cluster sampling method. Before sampling, the country was stratified into 36 states and the Federal Capital Territory, each categorized into urban and rural areas making a total of 74 strata. In each stratum, samples were selected via a two-stage process. First, clusters (enumeration areas) from the 1996 household and population census were selected from each stratum, with probability proportional to the size of the enumeration area. Then, in the second stage, a fixed number of households were systematically selected from every cluster through equal probability. All women aged 15-49 years in the sampled households were included in the survey. In the domestic violence module, one eligible woman in each sampled household was randomly selected.13
Study population
This study sample included all women aged 15-49 years who were interviewed in the domestic violence module, who had a singleton live birth in the two years preceding the survey and whose baby was alive at the time of the survey. We only included the most recent live birth in the preceding two years as data on breastfeeding were only collected for the most recent birth in the NDHS13 and to take into account the recommended duration of continued breastfeeding for at least two years.8 We excluded women with multiple gestations because these women usually breastfeed less in Nigeria, and this may not be related to IPV experience or other factors but just the burden of breastfeeding more than one child.28
Outcome variable
The outcome variable was ‘optimal breastfeeding for age’. Children under six months of age were optimally breastfed when the child was still being breastfed and had not had water or any complementary food on the previous day, during the day or at night. Children aged between six and 23 months were optimally breastfed if they received breastmilk (continued breastfeeding).
Exposure variables
The forms of IPV described in this study are emotional, physical, and sexual, from which the two outcome variables – any IPV and the number of IPV forms experienced - were derived. In this study, a woman was deemed to have experienced emotional violence if she reported any of the following acts by her husband/partner in the 12 months preceding the survey: (i) humiliated her in front of others, (ii) threatened to hurt or harm her or someone she cared about, or (iii) insulted her or made her feel bad about herself. A woman was classified as having experienced physical violence when she had reported any of the following from her most recent husband/partner in the past year: (i) was pushed, shaken, or something was thrown at her, (ii) twisted her arm or pulled her hair (iii) was slapped, (iv) kicked or dragged her or beat her up, (v) tried to choke or burn her on purpose, (vi) punched her with a fist or something that could hurt her, or (vii) threatened her with a knife, gun, or any other weapon. A woman was classified as having experienced sexual violence when she had reported any of the following from her most recent husband/partner in the past year: (i) was physically forced to have sexual intercourse when she did not want to, (ii) was physically forced to perform other unwanted sexual acts, or (iii) was forced with threats or in any other way to perform unwanted sexual acts. We defined any IPV as the experience of at least one of the three forms of IPV in the past 12 months. The number of IPV forms experienced is defined as the number of forms of IPV a woman experienced in the past 12 months, i.e., zero, one, two, or all three.
Covariates
Covariates in this study included the woman’s age at the time of the survey, educational level, and employment status, household wealth index, sex of the child, number of antenatal visits during the pregnancy with the child, child’s age, place of childbirth, mode of childbirth, parity, section, type of place of residence (urban and rural), and region. All covariates had been identified as factors associated with infant breastfeeding in previous studies.14–16,31–33
The woman’s age was categorised as 15–19 years, 20-29 years, 30-39 years and 40–49 years. We categorised woman’s educational level as no formal education, primary education, secondary education, and higher than secondary education. We categorised women’s employment status at the time of the survey as unemployed and employed. The relative household wealth quintile was used as provided in the DHS dataset (poorest, poorer, middle, rich and richest).
We recoded the number of antenatal visits in the index pregnancy as 0 visits, 1-3 visits, and ≥4 visits. We recoded the child’s age in months as 0-5 months, 6-11 months, and 12-23 months and categorized the sex of the child as male and female. We recoded the place of delivery as health facility or domestic setting. We expressed the mode of delivery as vaginal or caesarean delivery (15 women had a missing response to the mode of delivery, and we recoded them as vaginal births) and recoded parity as 1, 2-3, 4-5, >5. Place of residence was dichotomized as urban or rural, and the regions were North-Central, North-East, North-West, South-East, South-South, and South-West.
Data analysis
We conducted data analysis using Stata (17, StataCorp LLC, College Station, TX, USA). Individual women’s survey weights are needed in DHS analysis to adjust for multi-level cluster sampling survey design and non-response.34 As such, we adjusted for sampling weights, clustering, and stratification. We conducted a descriptive analysis of the sample, estimating the percentage of women reporting each form of IPV and the percentage of women with optimal breastfeeding practice by age of child. We then conducted a bivariate analysis using the Chi-square test to test the association between all covariates and optimal breastfeeding for age. We ran two multivariable logistic regression models to estimate the association between the experience of IPV and optimal breastfeeding for age. The first model tested the association of any IPV experience with optimal breastfeeding for age, adjusted for other covariates; the second model estimated the association between the number of forms of IPV experienced and optimal breastfeeding for age, adjusted for other covariates. All the variables associated at p≤0.25 level in bivariate analysis were included in the multivariable logistic regression models. Statistical significance of the multivariable analysis was set at a p≤0.05 and 95% CI. There were 66 participants with missing data in the variable - number of antenatal visits - and they were excluded from the multivariable analysis. There were no missing values for IPV-related variables and optimal breastfeeding for age.
RESULTS
Among the 10,678 women interviewed in the domestic violence module, 3,749 had singleton births in the two years preceding the survey and were included in this study sample. Of the women included in this study’s sample, nearly half (48.4%) were in the 20-29 years age group.,40.1% had no formal education, and 35.7% had secondary education. Two-thirds (66.5%) of all the women were employed. Over half (57.3%) of all the women had more than four antenatal visits during their index pregnancy, and 43.3% had their index childbirth in a health facility. Of the women in the study sample, the majority (97.1%) had vaginal birth in the index pregnancy. Two-thirds (34.3%) of all the women had 2-3 children, and 17.8% had one child. More than half of all the women resided in rural areas (56.5%) (Table 1).
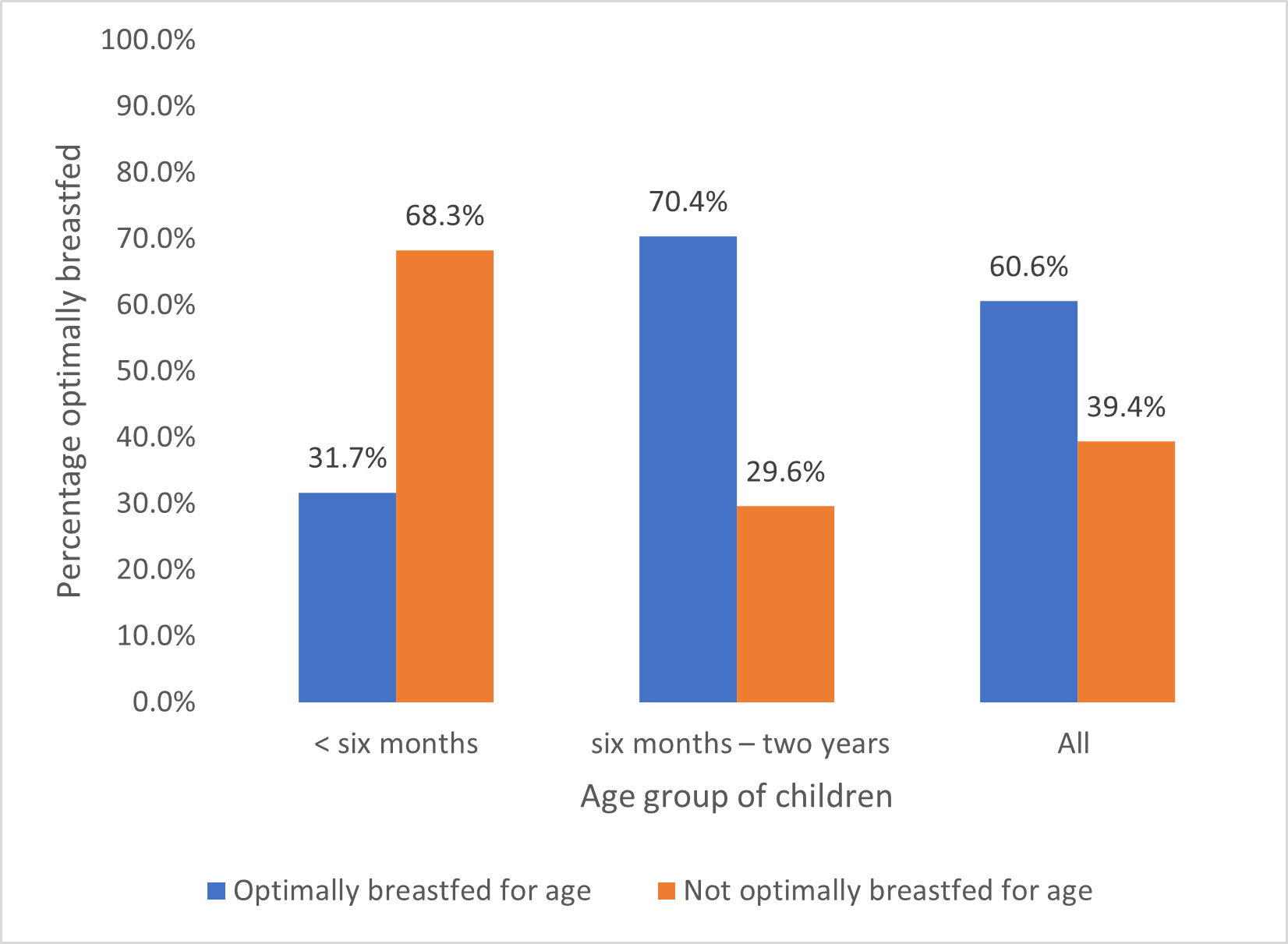
Overall, 31.1% experienced any form of intimate partner violence in the 12 months preceding the survey, and 2.7% experienced all three forms of IPV. Twenty-eight percent of women reported having experienced recent emotional violence, 13.4% physical violence, and 5% sexual violence (Table 2). Among the women in the sample, 31.7% of those with children under six months of age reported optimal breastfeeding (i.e., exclusive breastfeeding), 70.4% among mothers of children 6–23 months reported optimal breastfeeding, and 60.6% among all women reported optimal breastfeeding (Figure 1).
.png)
Bivariate analysis
Table 3 shows that for the age range 6-23 months, 65% of women who experienced physical IPV optimally breastfed their children, compared to 71.2% of women who did not (p=0.050). There were no statistically significant differences between reporting emotional violence, sexual violence, and the prevalence of optimal breastfeeding for age in both age groups, 0-6months and 6-23months. For the age range 6-23 months and all children 0-23 months, as women’s level of education increased, the proportion of children who were optimally breastfed reduced (p<0.001). Similarly, with increasing household wealth index, the percentage of children optimally breastfed declined. Sixty-five percent of children of women residing in rural areas were optimally breastfed compared to 54.1% in urban areas (p<0.001) (Table 3).
Multivariable models
In multivariable analysis, women who reported having experienced any IPV had 8% lower odds of optimal breastfeeding for age (aOR 0.92; 95% CI 0.76 – 1.14, p = 0.471), but this association was not significant. However, there was a statistically significant association between the number of IPV forms a woman experienced optimal breastfeeding for age. Women who experienced all three forms of IPV had 42% lower odds of optimally breastfeeding their children compared to those who did not experience any IPV (aOR 0.58; 95% CI 0.36 – 0.93, p=0.023). Women who experienced two forms of IPV also had lower odds of optimally breastfeeding their children, but the association was not statistically significant (aOR 0.79; 95% CI 0.53 – 1.17, p=0.238) (Table 4).
DISCUSSION
In this study, we set out to test the association between maternal experience of IPV and optimal breastfeeding for age of children 0 to 23 months old in Nigeria. We found that one in three women with children <2 years reported experiencing IPV in the 12 months preceding the survey, and less than one-third of children under the age of six months and two-thirds of children aged 6-23 months were optimally breastfed. We found no significant association between experience of any form of IPV and optimal breastfeeding for age. However, compared to women who had no experience of IPV, the 3% of women who reported all three types of IPV were 42% less likely to be optimally breastfeeding, and this association was highly significant.
In Nigeria, the most prevalent form of IPV is emotional IPV, followed by physical IPV and sexual IPV.13 In our study, 31.1% of women experienced any form of intimate partner violence in the 12 months preceding the survey, 28.1% of women experienced recent emotional violence, 13.4% physical violence, and 5% sexual violence. At bivariate analysis, for all the children, there was no association between either emotional IPV, physical IPV, sexual IPV and optimal breastfeeding for age, except for a significant association between physical IPV and optimal breastfeeding for age for children aged 6 months to 23 months.
Our findings support those from a similar study from Tanzania, which also showed that women who experienced all three forms of IPV had twice the odds of early termination of exclusive breastfeeding, indicating a cumulative effect of IPV on child breastfeeding practices.35 Women with more severe experiences of IPV, experiencing all forms of IPV – physical, emotional, and sexual – might be more negatively impacted by their experiences, which may negatively affect their breastfeeding practices. In addition, our study shows that this relationship extends beyond the child’s first six months of life.
In our study, we found no association between experience of any IPV and optimal breastfeeding for age. On the contrary, in Nepal and Timor Leste, women with experience of any form of IPV were less likely to breastfeed36 and in an Indian study, experiencing any IPV was associated with suboptimal breastfeeding practices.37 Similar to our study, a survey conducted in Midwestern United States, showed no association between previous experience of abuse or present experience of abuse (at the time of the survey) and breastfeeding.20 Furthermore, a study from Australia found that breastfeeding rates did not significantly differ between women who experienced IPV and women who did not,21 and in a study among Swedish women, mothers exposed to IPV during pregnancy or postpartum were just as likely to breastfeed as mothers who had not reported exposure to IPV.22 In our study, only a small proportion of women (2.7%) had experienced all three forms of IPV, and about 9% experienced two forms of IPV. This probably suggests that most women’s experience of IPV was not severe and, as such, did not affect their breastfeeding practice.
Policies aimed at promoting breastfeeding should include measures to combat IPV against women. Healthcare workers should screen pregnant and nursing mothers for evidence of IPV, as this can negatively impact the child’s nutrition. In terms of future research, there is a need to further explore the pathway by which IPV influences breastfeeding practice considering a possible cumulative effect. Future studies are needed to unravel whether women who have more severe experiences of IPV experience more emotional, psychosocial, or physical barriers to breastfeeding (deficit hypothesis)27 compared with women with fewer experiences of IPV, who may be more able to compensate for their experiences of IPV and thus breastfeed their babies as equal as unabused women (compensatory hypothesis).38
To the best of our knowledge, this study is the first to examine the relationship between IPV and optimal breastfeeding for up to two years of age in Nigeria; most previous studies only examined the relationship between IPV and exclusive breastfeeding.19,23–26,28,35 This study is, however, not without limitations. Due to the cross-sectional nature of the survey, causal inferences cannot be drawn between the experience of IPV and breastfeeding practices of the mother. Secondly, there may be an underreporting of IPV as women could be prone to give socially desirable answers. Additionally, women whose privacy could not be ensured were not surveyed; these might include women with the most severe exposure to IPV and controlling behaviour of male partners. Thirdly, due to the nature of the DHS, children younger than six months were categorized as being optimally breastfed for age if they were exclusively breastfed and children aged 6 to 23 months if they were currently being breastfed. This categorization did not consider other elements of optimal feeding, e.g., frequency and adequacy of breastfeeding, including feeding on demand (among <6-month-olds) and supplementary feeding practices among 6-23-month-olds. In addition, exclusive breastfeeding was assessed based on 24-hour recall. This may have introduced some bias as children may have been fed non-recommended foods before this 24-hour period.
CONCLUSIONS
The prevalence of any IPV among Nigerian women with infants younger than two years of age is very high. Efforts must be instituted to ensure that these women can be identified and helped. Concerning influence on breastfeeding, we see a cumulative effect of multiple forms of IPV, meaning that women most severely affected should be a priority. Policymakers, government and non-governmental organizations and health workers need to step up efforts to mitigate the adverse effects maternal experience of IPV can have on child nutrition and development. Community engagement with religious organisations, the civil society and trade unions can help address the high prevalence and severity of IPV, which, among other negative consequences, impacts breastfeeding practices.
Acknowledgements
We thank the DHS Program for providing access to the Nigerian Demographic Health Survey dataset. The first author (TO) wishes to acknowledge the DHS Summer course of the Institute of Antwerp, Belgium, as this paper was an output of the course.
Ethics statement
Ethical approval was not required for this secondary data analysis. The survey protocol of the 2018 NDHS received ethical clearance from the National Health Research Ethics Committee of Nigeria (NHREC) and the ICF Institutional Review Board. Informed consent was obtained from the respondents who took part in the survey. We obtained permission to download the NDHS 2018 dataset from the Measure DHS website (www.dhsprogram.com).
Data availability
The NDHS 2018 dataset is available for download from the Measure DHS website (www.dhsprogram.com) after registration and request.
Funding
This paper was funded by The Institute of Tropical Medicine (ITM) - DGD Scholarship. AA is a recipient of Research Foundation - Flanders Postdoctoral Fellowship Award (Number 1261923 N). AB-T was funded by Google and by Bill and Melinda Gates Foundation (Investment ID: INV-032911). LB was funded in part by the Research Foundation–Flanders (FWO) as part of her Senior Postdoctoral Fellowship (Number 1234820 N).
Authorship contributions
TO, AA, and LB conceptualised the study. TO did the data analysis. AA and LB supported the data analysis. TO prepared the first draft of the manuscript. AA, AB-T, MRB, IPO, OOO and LB critically revised the manuscript for intellectual content. All authors have read and approved the final draft.
Disclosure of interest
The authors completed the ICMJE Disclosure of Interest Form (available upon request from the corresponding author) and disclose no relevant interests.
Correspondence to:
Tope Olubodun
Federal Medical Center AbeokutaDepartment of Community Medicine and Primary Care, Federal Medical Center Abeokuta, Ogun State
Country: Nigeria
Email: [email protected]