Drinking alcohol is very common in most cultures in India. Alcohol use in India is on the rise. India’s per capita alcohol consumption was 2.4 litres in 2005; it increased to 4.3 litres in 2010, to 5.7 litres in 2016 and is estimated to be 7.9 litres by 2025.1 According to the National Institute of Health and Family Welfare, alcohol use varies between 23 and 74 % in men across the various states of India.2 WHO estimates it to be around one-fourth to one-third among the male population.1 Historically and in the present context of increased consumption of alcohol by men, the health and lives of families in India are negatively impacted.
It is widely acknowledged that alcohol use disorder is a disease of the entire family. Rightly so, as it is not only the men who consume alcohol who bears the brunt of the disorder but the entire family, especially women in these families.3–5 Besides, owing to the deeply entrenched patriarchal norms and traditions, most women in India do not enjoy their rights and opportunities fully. A culture of male dominance that values women as subordinate has been in practice for generations, and thus gender discrimination is deep-rooted in the fabric of Indian society. Most women are cloistered as children, married off at an early age and deprived of education, health facilities and access to information, social networks and other resources. These disadvantages become acute and critical while living with an alcohol-dependent partner. Thus alcohol use disorder and problems in the family are a common pairing that goes hand in hand. Riddled with stigma and lack of support from family and society, leaving an abusive relationship or remarriage is also not an easy option for many women. Women are thus forced to continuously face myriad of immediate to long-lasting challenges.6
The existing literature examined shows that there is a large body of significant work done on alcohol use disorders and the consequences for the individual, which include health concerns, lack of productivity and financial difficulties. Studies from across the globe and a meta-analysis from 10 countries7 reported that AUD is also linked to numerous consequences for the women of AUD partners like stigma,8 social isolation,9 neglect,10 marital conflicts,9,11,12 health concerns,9–11 injury12,13 and violence9,12,13 and financial difficulties.9,11 Further, women had to abandon their dreams and self-care, overloaded with the care of family and had to maintain the family.14,15 Although addiction treatment has been around for many decades, it largely focuses on the person with AUD and neglected family members. There is documented evidence of the importance of involving a family in treatment16 to engage and treat the individual, involve the family in the treatment, and provide support and services to family members during the crisis. However, a scoping review in 2018 highlights the gaps in support and services rendered to women of AUDs16 when they needed it the most.17
Often, de-addiction centres across India involve women to help husbands progress to a sober lifestyle but overlook exploring or addressing their challenges.6,16 To date, few studies have utilised the phenomenological design to explore women’s perspectives and experiences in the Indian context. Substantial gaps remain in our understanding, and this study design can elucidate in-depth perspectives to understand women’s experiences and inform future intervention studies.
This study explored the lived experience of women cohabiting men diagnosed with alcohol use disorder, within the context of phenomenology.
METHODS
Rooted in a constructive ontological position, a qualitative inquiry using the phenomenological lifeworld approach described the richness of human experiences.18 The lifeworld approach constructs the essence of a phenomenon by exploring it from the perspective of those who experienced it.19 This approach was used to explore and describe how the women experienced their lives and interpret how they made sense of their world in the context of their partner’s alcoholism. An in-depth literature review was not undertaken early in the research.
Role of researcher
The researcher used etic or outsider view in this study. The researchers role, firstly, stemmed from the assertion that lived experiences of women need to be constructed as they manifested or unfolded19; secondly, that data are mediated through the human instrument, the researcher, not through scales or inventories; and finally, acknowledging researchers own bias, assumptions and perceptions of the behaviour of persons with alcohol use disorder (AUD), using bracketing or epoché.18
Study location
The de-addiction clinic of the Institute of Liver and Biliary Sciences, New Delhi, India, which is a tertiary-level hospital for liver, biliary and pancreatic diseases.
Participants’ selection
Participants were women with AUD partners who accompanied their partners for receiving intervention at the current alcohol treatment facility and were thus offered participation. Purposive criterion sampling was used to select women who had experienced the phenomenon (information-rich informant) cohabitating for more than one year. Women included were over 25 years old and were free from substance use or psychiatric disorders. As this study was cross-sectional and the problems in family life cannot be solely attributed to alcohol use, women were screened for any other stressful life event using Social Readjustment Rating Scale (SRRS) and included if scores were below 150. Women excluded were whose husbands had a history of other substance use disorders (except smoking and chewing tobacco), medical illness (other than liver diseases) or psychiatric disorders and were liver recipients. Further, women were excluded if they were liver donors to their husbands. This sampling helped to create a pool of participants who had a rich experience of the phenomenon.
Instruments
i) AUD, as per DSM-5, was identified if a minimum of two of 11 criteria was present20; ii) SRRS by Holmes-Rahe was used to check for other stressors that happened over the last year on 43 life events; each event was assigned a score ranging from 11 to 100.21 A score of less than 150 meant a low amount of life change and score above 150 implied a major stressful change; iii) Demographic profiles of women and partners; iv) In-depth face-to-face interview with audio recording and field notes. Interviews were structured around a guide of open-ended questions to elicit detailed answers in a standard sequence,19 lasting 30 to 40 minutes each. Developed by the researcher, the guide included seven central questions (Table 1) and a few probing questions for use when needed, reviewed by five qualitative experts and revised. The researcher was trained in the methodology and interview techniques. Pilot interviews were tried on three women.
Data collection
After administrative and ethics clearance, the researcher identified AUD patients at the de-addiction clinic and enrolled women who consented and met the criteria. One-to-one interviews were conducted in privacy and comfort, making participants relax and share their experiences. Interviews were in-depth to gain rich data and audiotaped with field notes to supplement the recordings. Data was gathered to saturation or until no new information was forthcoming, i.e., till interviews of 11 women, over three months.
Data abstraction and synthesis
Data from recordings was transcribed verbatim for an unbiased experience description. Each encoding was marked by an alpha-numeral (P for participant and numeral 1, 2, 3 … for the sequence of recruits). Field notes were referred to, incorporating behaviours like smiling, sighing, stammering, crying, silence or pausing. Transcripts were returned to women to verify the correctness of their views (member checking) and elaborate on their responses. With feedback incorporated, transcripts were translated into English and validated by back translation. Thematic analysis was done manually using six steps22: data familiarisation, data coding, developing sub-categories and categories, theme generation, revision and write-up. The first step was getting to know the data or immersion in data by intensive reading. Significant statements in the raw data were identified, extracted into meaning units and labelled with short descriptors, thus generating codes. Two coders independently coded the entire data set, which was compared and finalised (a total of 192 codes) after discussion. Codes were then examined for patterns and interrelationships, combined to develop clusters of similar challenges of alcohol use and the various forms of coping into sub-categories. While working back and forth reading the data, sub-categories were grouped into categories. Following the categorising, some common features identified helped generate two themes. Audit trails starting from coding to forming themes were reviewed along with the log of activities and preserved. As the analysis ended, data was organised into a structure where the pattern of lived experiences of women became evident. In the final step, the write-up provided a “thick description” to understand women’s lived experiences cohabiting with an AUD.23 To enhance data quality, many strategies were used. Audio recording ensured accuracy and back translation of transcript language validation. Bracketing biases from data gathering and analysis assured data accuracy. Member checking or respondent validation ensured the data’s validity and maintained the phenomenon’s objectivity. Inter-coder agreement (94%) for coding enabled dependability or trustworthiness. The auditable trail of the entire process provided transparency and ensured confirmability. Transferability was ensured in the thick description.
Ethics
Institutional Ethics Committee clearance was obtained vide No.:F15(2/2.25)/2017/HO(M)/ILBS. The participant information sheet provided details about the study, procedures, purposes, voluntary nature and procedures to protect confidentiality. Written informed consent forms were taken from the women for participating in the study and audio-taping the interview. Women could withdraw from the study at any time without penalty, all data gathered were treated in confidence, and their identity was not revealed in the study.
RESULTS
Women were between 30 to 46 years, belonged to both joint and nuclear families and were married for more than a year to over 16 years (Table 2).
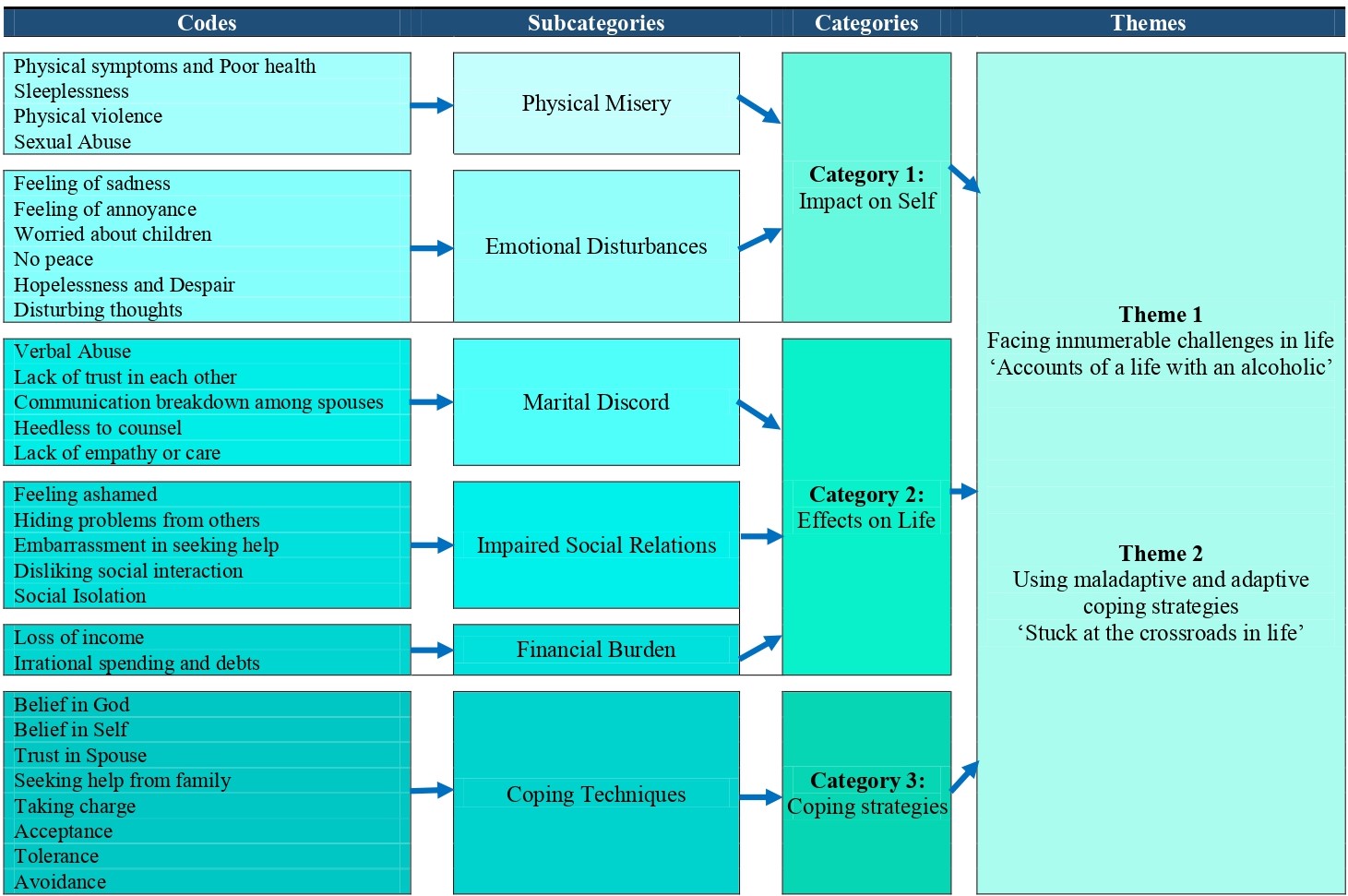
Figure 1 displays the codes, sub-categories, categories and themes generated from the data. The women’s tales predominantly exhibited sadness, frustration and hopelessness.

The first theme was, faced with innumerable challenges, ‘Accounts of a life with an AUD’ which was developed from two categories: impact on self and effect on life. The first category developed from sub-category like physical misery and emotional disturbances was impact on self.
Physical Misery. The drinking behaviour of husbands brought many problems for women. Once drunk husbands were not in their senses and displaced their anger on wife and children. Extracts showed that women experienced physical discomfort like "… pain in the hands and feet (P1,3,4,9,10), suffering, unable to perform daily activities “I cannot walk longer” (P1,4), "….fights and arguments till late at night (P2,3,4), “…felt giddiness, sickly…” (P3), “.. tired (P2,8,9), weakness (P9)”, “…I had headaches (P7), my health goes bad” (P2,7,8), felt anxiety, "I am tensed (P7,10), cannot even eat food (P3,7,8,9) … my weight has reduced (P2)…". These symptoms were clustered into the code physical symptoms and poor health.
Inability to get some shut-eye was one of the major problems faced by the women of AUDs “I cannot sleep at night (P2,3,4,8,10)”, late night drinking "…disturbances (P1,2,3,4)", "…fights late into the night (P2,3)", anxiety “thinking (P2,4,10)”, “…pain (P10) and unable to wake up early (P2)”. These were clustered as sleeplessness. It affected their day to day lives and activities.
The women of AUDs suffered physical violence at the hands of their husbands “…he is throwing something or other” (P2), “…sometimes he beat me..” (P9); sexual abuse “he is addicted to sex … does not talk to me properly” (P10). These above codes generated the sub-category, physical misery.
The second sub-category was Emotional disturbances. Various emotional upheavals were seen in the women. The codes that generated this sub-category included feeling sad, annoyed, no peace, worry about children, hopelessness, despair and disturbing thoughts.
Foremost was sadness “…am so unhappy” (P2,3), “…feel very upset” (P3,8), “cannot do anything for children” (P2), “… did not know his drinking habit” (P2,11). The clusters that showed prolonged anguish about their life were coded as sadness. This was coupled with frustration because “After drinks, he talks nonsense continuously (P4,6,7)”, “… a lot of fights among us at home” (P2,3,4,8), “…fights late into the night” (P2,3), “…cannot even tell my parents” (P2), “I used to get irritated” (P6). The code feeling of annoyance was assigned to these excerpts.
The women worried about children as their husbands were not concerned about children or family. These extracted statements found that they worried about her children’s lives and future "…worried about children (P5,8,9), I wish to buy something for children (P2), I cannot afford (P4,5)“. “Children are growing up… who will take care of marriage (P4,8,9), studies (P8,9), ..save money for children” (P6), “..cannot depend on relatives” (P6)”. The code was named worry about children.
Every wife wished to have a peaceful life. It was reflected in these extracts “…there was no peace of mind (P1,4,5,8)”, “…it was always struggling…daily fights” (P4), “arguments even for small issues (P3,4)” and coded as no peace. Some women gave up their life’s dreams and desires, “No one understood me, not even his parents…it upsets” (P3), “…no hope from anywhere” (P4), "…all my desires are going away" (P2). No hope in life was coded as hopelessness and despair.
Many thoughts were upsetting “…just thinking” (P2), “…my mind is disturbed” (P3,4), “… feel like ending life” (P4), “his parents misunderstood me” (P3), “… feelings are very hurt” (P3), " feel like crying all the time" (P4,7), “my family is upset too” (P3), "…unable to do activities" (P3), “…. I keep silent” (P7). It was coded as disturbing thoughts.
The second category was the effects on women’s life, formed from sub-categories like marital discord, impaired social relations and financial burden.
Most women faced discord in their marital life due to a lack of trust, abuse and violence. They faced the insults of their husband as in “…he used to shout at me and say bad things”(P2), “everyone is upset” (P3) “…speaks nonsense continuously..”(P4,6,7), “..insults others …my brother rarely comes to my house”(P3), “daily fights, arguments, threats” (P4). These clusters of extracts were coded as verbal abuse.
Some women of AUDs lost faith in their husbands because they lied and hid their drinking habits. “I do not believe him… he always tells lies and hides…” (P3), and “I do not trust him” (P10). So these clusters were coded as lacking trust in each other. Few of them felt estranged “…it’s been 15 years… he lives on his own terms…” (P8), “…do not talk to each other (P4,7,10)”, “… we stay separately, doing for children” (P10). Hence these extracts were coded as communications breakdown among spouses.
Most of the AUD husbands threw caution to the wind “..he never listens” (P2,4,5,10), “…I refused to let him drink” (P2,5), “…it is for his health”(P5). Thus it was coded as heedless to counsel. The AUDs were indifferent to the concerns of their women, children or family as evident in their expressions “…never understands me” (P4,6,10), “tried many times” (P6), "no support from him…" (P8), “…speaks nonsense…” (P3,4,7), "… spent earnings on drinks (P2,3), “.. lot of expenses, wastes most of it” (P2,4), “…daily fights” (P4), “argues even for small issues (P3,4)”. These statements were coded as a lack of empathy or care. These codes were formed into the sub-category marital discord.
The next sub-category was impaired social relations formed by following codes. Some women felt embarrassed and shameful about their husband’s addiction “… feel little and ashamed, people talk, (P2,3,7,10) now his health is bad (P2) … others know” (P7,10) and named the code as feeling ashamed. Some women had to even hide their drinking habits as expressed in extracts "Both families were happy when we got married (P2)… I hide problems (P2,10), I live a hidden life (P7),… cannot tell my parents or neighbours (P7,10) or relatives (P10) I cry alone silently (P7)…". The code referred to here is hiding problems from others. Seeking help was also seen as shameful and a source of disgrace to the family “..taking any help is a bit embarrassing (P4,7),…they start talking” (P4,7). Hence was coded as embarrassment to seek help.
Many women avoided interaction with others for fear of having to open up “..do not like talking to people (P3,7,10,11)…”, “..do not talk about it… people talk at the back (P3)”. The referred code is disliking social interaction. Few of the women had less socialising with others. As this extract reveals “… I do not go out of my home much, rarely go to relatives (P2,10,11)”, “…stay at my home mostly…not even go out with him” (P3). P7 said “I eat alone”. These clusters are code named social isolation.
Another sub-category generated was a financial burden. From the clusters of extracted statements, it is clear that a large sum of money was expended “…he spent earnings on drinks (P2,3) … lot of expenses, wastes the most in it”(P2,4), unable to provide for the family due to ill health "…is lying here no other means (P1,4,6,8), does not support the family “does not give to family (P1,2,8)”, "others do not pay back loans (P4), incurs debt or loses job “there is the financial problem” (P2,4,5,8)". The families had to fend for themselves. This code was named financial burden due to loss of income and irrational spending.
The second theme, ‘stuck at the crossroads in life’, was developed from the various categories of coping styles used by women in facing the alcoholism of their partner. In the extracts below, the women shared their experiences of how they cope with their husbands drinking. A few of them put their faith in God to help them, ie.,“… I trust in God (P2,9) … grace and kindness of God (P2,6)”: code-named belief in God. Some believed in self “… confident of myself (P5)”, “… can handle any problem”(P6). Coded as belief in self. Despite being AUD, some relied on a positive outlook like “I get angry, but I calm down knowing that talking in that situation is useless. He does not know what he’s talking about; the next morning, he forgets what happened last night” (P8). I wish him to get well soon (P9)". A few exhibited trust in their husbands, in that “We trust each other….” (P5,11). We are in it together, in sorrow and happiness…he believes in me, and I also do (P7)", “he does not disturb others… he is good…even though he drinks, not like others who drink and beat their women, he is not abusive…”(P11), “…he loves me, he does everything for me (P7)”, he also earns (P9) "I love him (P2,11) … with love only make him understand, it works to improve his behaviour" (P11). This was coded trust in spouse and acceptance.
Some of the women sought help from family in time of need, “Yes, I am getting support” (P2), “support from family” (P2,6,7,10,11). These statements have been coded as seeking support from family. Some others felt that as their husbands were not concerned about the family and children, they took over responsibilities as in these extracts "…he is not having concern regarding expenses in family, I am managing it right now…" (P3,4). “I have to look after home and education of my children. If the children are rusticated from school, there will be no option…. my husband is sick” (P2).“If there is a problem, then we have to solve it … I have the strength to handle any problem” (P6). Here the women expressed their strength to handle responsibilities and solve her problems. Code given to this cluster is taking charge of helping the AUDs.
Some of the women felt that there was no point in talking, had given up or were radio silent to avoid confrontations, seen in statements such as “….there is no point of talking” (P2,4). P6 felt “It is 20 years now, it is fine…”, P6 also said, “..we adjust to keep the family atmosphere calm”. “… given up, let him do what he feels, … what else I can do?” (P4,5,7,9). Code named tolerance. Women said “… I avoid him..” (P8), “…I go outside and sit alone…”(P4,10), “no much energy in me to speak” (P2,10), “I used to get angry …. now I just keep quiet” (P4,7,8,9,10). P (7,10) expressed that “I do not want to fight …. I do not have strength …to get peace” (P9). The code assigned to the clusters is avoidance. From these statements and codes, the sub-category that was constructed is coping techniques employed by women.
Overall Essence Women of AUDs experienced various physical health and violence, emotional, financial and social challenges. Each one faced some or all of the challenges at the time of study or has been experiencing them for some time and may have to cope indefinitely. It led to a generation of three major categories: Impact on Self, Effects on Life, and Coping Strategies used. Two themes were constructed “Faced innumerable challenges in life” and “used adaptive and maladaptive coping techniques” to answer the research question. Invariably, all the women living with AUDs faced a lot of challenges and relied mostly on coping strategies that were not healthy or productive that could cause them further harm.
DISCUSSION
In this study, 11 spouses of men with alcohol problems were interviewed. The study explored women’s experiences and found that partners’ alcoholism posed several problems for the women.1 From the analysis, two themes and many sub-themes emerged: the first theme showed that the women “faced innumerable challenges in life,” indicating the amount of verbal, physical, and emotional abuse they suffered and endured. Women experienced poor health marked by fatigue, pain, and sleeplessness, similar to other studies where poor general health and quality of life were seen,9,10 felt overpowered and overwhelmed.17 Moreover, women had an increased risk for physical abuse, as seen in other studies: 63.5% of women sustained injury by their husbands,12 60% AUDs were violent to female partners as against the 12% in the comparison sample.19 As in another study, women covered their drinking habit for fear of disgrace and dishonour to the family.14 Some faced stigma and ostracisation when these habits came to light.8 They withdrew to themselves and felt sad, lonely, frustrated, with no peace and hopelessness, worried about children and had disturbing thoughts.14 AUDs, preoccupied with drinking, ignored needs, did not provide for family and neglected expected roles and responsibilities. This placed a lot of task overload14 and added burden on the women. The results corroborate the findings of earlier studies.3
Confirming the results of this study were other studies that found lifetime at-risk drinking a risk factor for psychological distress in spouses,24,25 depression,26,27 moodiness, anxiety or stress.13,26 Similarly, it was found that 38% reported depression and 59% reported anxiety.28
A well-documented association exists between the financial difficulties, losses and debts caused by husbands drinking, which increased the burden and suffering of women.29 Marriages marred by alcoholism shook the very bedrock of the relationship, marked by violence, abuse, neglect, disconnect, lack of trust and proper communication among spouses. Physical, social, and economic abuse lead to marital discords.12 It was seen as stressful and confrontational.27
With an apparent lack of support or assistance, most women did nothing about it. Living in constant stress like this and not paying attention to problems have long-term effects on women, including chronic health problems, mental illness, permanent injuries and damaged relationships.
The second theme is that women employed both adaptive30 and maladaptive coping,31 as corroborated in other studies.27,28 Women need support and counselling to use adaptive coping for two reasons: firstly, for self-preservation and to prevent long-lasting harm; secondly, coping methods like avoidance, acceptance, tolerance, faith, emotional blunting and hoping for change can be damaging as it ignores the real problem as it worsens. Literature also abounds with evidence that women’s unhealthy relationships with AUDs might hamper partners’ recovery.32
A review by McCrady and Flanagan published in 2021 compiled many empirically efficacious interventions for families of AUD, such as Al-Anon, community reinforcement and family training (CRAFT), the 5-step method, a relational intervention sequence for engagement (ARISE), significant other engagement in motivational interviewing (SOMI), alcohol behavioural couple therapy (ABCT), behavioural couples therapy (BCT), brief family-involved treatment (B-FIT), brief strategic family therapy (BSFT), multidimensional family therapy (MDFT) and multisystemic therapy (MST).4 A study found that women who wanted interventions that did not require disclosure or identifying victims had multiple options and preserved respect for autonomy.17 On completion of the interviews, all study participants were referred to the counsellor for further evaluation. Self-help networks were formed to empower each other along with marital and family therapy, which was seen to be helpful in the prevention and treatment of the AUDs and partners,19 was instituted at the current facility with a designated counsellor.
This study underscored that women in Indian society faced the constant stress and strain of living with an AUD and had very limited choices for help-seeking. Even when some attended de-addiction centres with their partners, their need for therapy as victims often went unnoticed. Findings also indicated that women needed to use adaptive coping strategies to mitigate the detrimental effects on them and the AUDs. Thus gaps were identified in unmet needs, provisions of support, protection and services that empower women with information, education, skills, and lack of interventions that focus on the needs of women. There are currently no clearly defined best practices. Hence healthcare professionals, facilities, and policymakers in India must develop and implement the best family-focused interventions. The training of professionals has to consider family-focused treatment knowing that AUD has a ripple effect across the person’s family and friends network. Mental health nurses need to provide empathetic understanding, support and counselling to women to use adaptive coping to reduce physical, emotional and behavioural problems, improve family relations and aid in treating the AUDs.
The study’s strength lies in the use of thematic analysis well suited to large data sets. The researchers used a systematic and rigorous approach to reflect and shape the data analysis continuously. Braun and Clarke’s quality check was done to ensure this reflexive approach. The main limitation includes a selection bias of women sub-selected by AUDs under treatment. Findings reflect the experience of women whose partners are motivated to enrol in a de-addiction programme at a tertiary hospital, which may explain the lack of reporting of very violent or extreme AUD behaviour. Furthermore, the experience was self-reported by participants; hence there is a chance of under-reporting due to stigma. Future large-scale and multisite studies can examine nationally representative samples, explore women’s resilience, women’s experience over time in a longitudinal manner and what interventions women prefer.17
CONCLUSIONS
It requires a continuous commitment from the healthcare system, where personnel like mental health nurses and others involved with AUDs have an important role in supporting family members and strengthening their support systems. Thus, given the rising alcohol consumption among men, special attention must be paid to the needs of women cohabiting alcohol-dependent partners.
Acknowledgements
Faculty, Manipal College of Nursing for independent coding
Experts involved in vetting and translation
Ethics clearance vide No: F15(2/2.25)/2017/HO(M)/ILBS/CONEC/ILBS/09/19
Funding
No funds received for the study
Authorship contributions
MG: Conceived, thematic analysis, wrote paper
NBD: Collected, coded data and thematic analysis
Competing interests
“The authors completed the Unified Competing Interest form at http://www.icmje.org/disclosure-of-interest/ (available upon request from the corresponding author), and declare no conflicts of interest.”
Correspondence to:
Dr Mini George PhD, MPhil, MN, BSc (Hons) N, RN RM
Principal, College of Nursing, Institute of Liver and Biliary Sciences
D-1, Vasant Kunj, New Delhi -110070, India
[email protected], [email protected]