
The WHO Rehabilitation Call to Action 2030 highlights the importance of strengthening health systems to provide rehabilitation.1 Chronic respiratory diseases (CRDs) represent a significant global burden, especially in LMIC,2 where >90% of CRD-related deaths occur and where the demand for pulmonary rehabilitation (PR) greatly outweighs capacity.3 PR is supported by the highest levels of evidence4 and reduces the disability associated with lung disease. This multidisciplinary, complex intervention has supervised exercise training and education at its core, supporting people to manage their condition.5 In LMIC, PR has the potential to make a significant and sustainable contribution to the wellbeing of individuals as well as wider social, cultural and economic impacts.6 Although recommended internationally,4 the capacity to deliver PR in LMIC is underdeveloped.7
The National Institute for Health and Care Research (NIHR) Global RECHARGE Group (17/63/20)8 seeks to build capacity to address the unmet need for PR in LMIC. With five project partners in four countries - India (Pune and Delhi), Sri Lanka (Colombo), Kyrgyzstan (Bishkek) and Uganda (Kampala), the project proposes to reduce the disability associated with CRD through context-specific PR and building capacity for research,9 leadership and service development.10,11 With NIHR support LMIC partners are exploring how to implement and take account of the cultural, workforce, demographic and health differences.12
Accordingly, we describe an innovative education programme designed to build sustainable local capacity in PR teaching and delivery in LMIC. The Global RECHARGE Group, in collaboration with the International Primary Care Respiratory Group (IPCRG), developed a Teach the Teacher (TtT) programme. Our TtT programme is a scalable and sustainable model for workforce training, building local capacity to develop expertise in PR, service development, and teaching clinicians how to deliver PR.
METHODS
IPCRG is a clinically led charity, collaborating globally with primary care partners to achieve a vision of a world, feeling and breathing better through universal access to the ‘right care’.13 The IPCRG education strategy proposes a TtT programme model to increase teaching capacity in primary care.14 It encompasses teaching and learning principles taught in parallel with evidence-based clinical content. Unlike conventional ‘train the trainer’ programmes based on a model of cascading knowledge,15 this approach empowers clinicians working in multiple health systems and in different languages, to think creatively about developing context-specific programmes that strive to maintain fidelity to evidence-based practice. Previous TtT programmes have been piloted successfully in two European programmes on difficult-to-manage asthma16,17 and tobacco dependence, as well as a global programme on paediatric asthma18 and a Latin American programme on Asthma Right Care.
The RECHARGE-IPCRG TtT comprised a three-tier cascade programme (Figure 1) of education and was adapted for PR and, due to the severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) pandemic, it was further adapted to a digital-only environment.
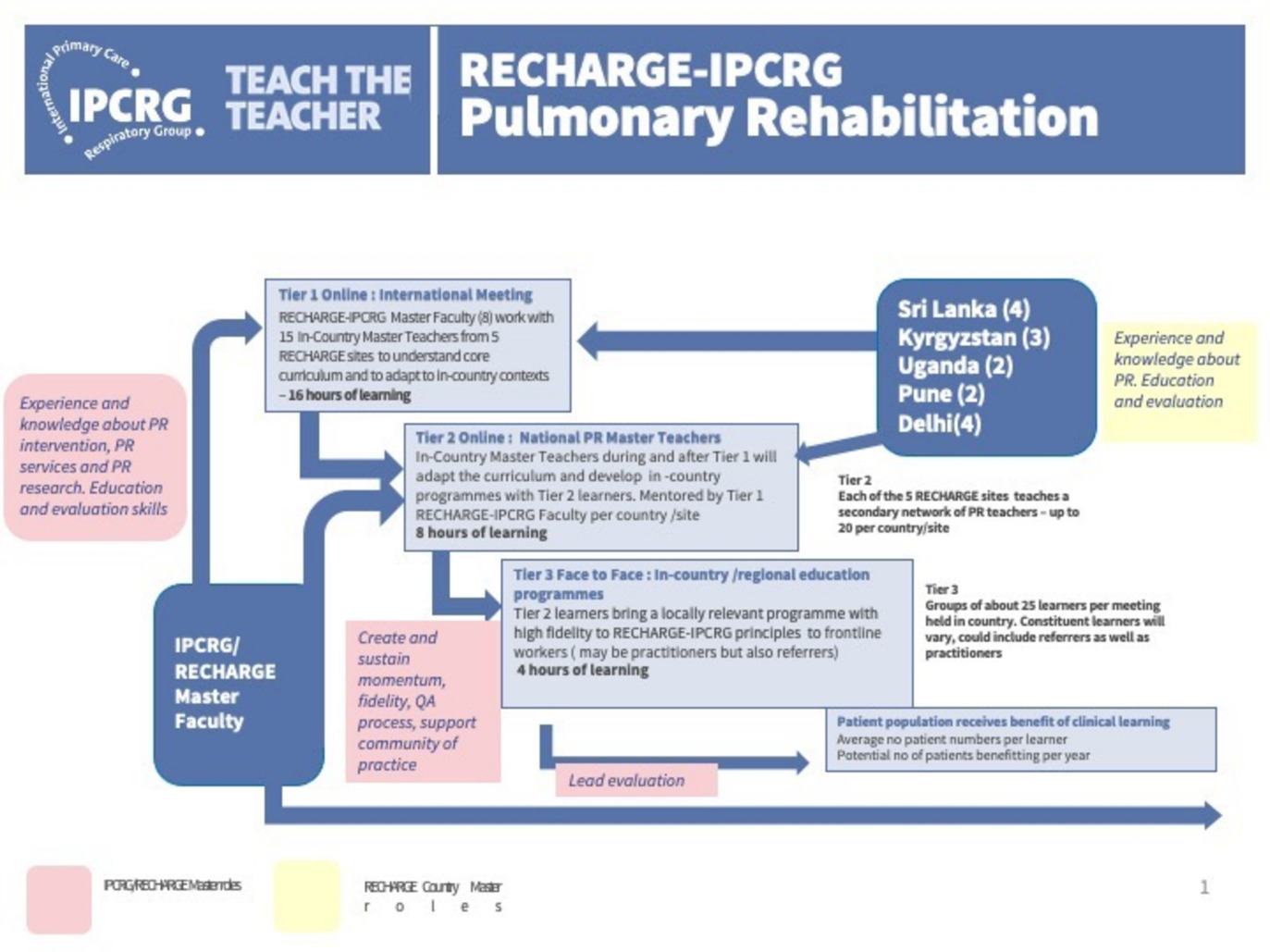
We first convened a joint RECHARGE-IPCRG Master Faculty with combined expertise in PR (research and practice), teaching and learning for primary care, policy and behavioural interventions. We then conducted a situational analysis (SI in online supplementary material) to inform the curriculum and learning design. This was completed by Principal Investigators (PIs) and team members from each of the five RECHARGE project partners. This helped the faculty to understand differences and challenges in respective healthcare systems, education and PR provision. We discussed the analysis with PIs to decide where to focus the programme to complement what was already offered as a core part of the research. We decided to focus on the education element of PR because there is greater potential variation in learning needs and adaptation for context than the exercise component and a lack of capacity to support spreading and sustaining PR. We recruited participants termed ‘In-Country Master Teachers’ (n=15) whom PIs selected based on a bespoke teacher specification (S2 in online supplementary material), including an assessment of English language capability, teaching/online teaching experiences, PR knowledge and PR delivery experience.
There were specific adaptations to the programme design, resulting from the need to transfer to an online learning environment due to the SARS-CoV-2 pandemic. We held a ‘Tier Zero’ meeting with a broader group of stakeholders to enhance online teaching and learning skills. A series of RECHARGE-IPCRG Faculty planning meetings enabled programme design and selection of optimal educational approaches. We consulted PIs about the feasibility and timings for online events. We used digital tools (such as Padlet: https://en-gb.padlet.com) for Faculty and Country Master Teachers to introduce themselves using text and photographs before the event.
We also held a technical pre-meeting (16.9.21) to build engagement with participants. The meeting lasted one hour and was hosted by some of the faculty. We met participants and introduced them to the online environment and features of the online platform, such as the ‘chat function’, reactions/ emojis and room management.
The Tier 1 online international meeting took place over four sessions, each lasting four hours – sixteen hours of education (September-October 2021). All the sessions took place online. The curriculum consisted of teaching principles and techniques, the components of PR, and we supported participants in considering how to adapt the core PR curriculum to local settings (Table 1). For example, we included a session on which topics were culturally appropriate to include. While most participants would include topics such as how the lungs work, there were differences of opinion about including other topics such as how to have sex when breathless, death and dying and worrying about family finances.
Throughout the programme, there was a deliberate balance between teaching the important elements of PR (clinical content) and exploring how the Country Master Teachers would subsequently teach this to their clinical colleagues (process). This balance was achieved in many ways:
-
We used various online teaching methods and tools, including Zoom features such as chat, Q&A and reactions; live polling; live surveys (e.g. https://www.polleverywhere.com/); videos; formal slide presentations and small group work in breakout rooms followed by whole group feedback and discussions.
-
Google Classroom was used as a repository for learning materials, session transcripts, and recordings, made available to all participants.
-
Transparent decision-making, whereby the RECHARGE-IPCRG faculty shared with participants about the process elements in running the course and demonstrated real-time dynamic adjustments to teaching content and delivery.
-
Faculty Members were paired with each country group to offer support and mentoring. The Faculty also communicated behind the scenes, using WhatsApp and dropbox to share resources and adapt the programme in real time.
At the end of Tier 1 online international meeting, each country team presented proposals for PR education programmes and how they plan to transition their programme into tier 2 and tier 3 (Figure 1). This was delivered via PowerPoint presentation, with the faculty and other participants acting as a panel for discussion and constructive feedback. The teams contextualised the programmes to their local environments, including healthcare systems and cultures. They identified key stakeholders to ensure the scalability and sustainability of their programmes. We incorporated theory and practice of leadership and improvement skills during the course, which was also demonstrated in the final presentations.
FINDINGS
Case report
We used an adapted framework to evaluate professional learning and its impact (Figure 2).19 There are five levels of evaluation with different indicators, ranging from simple to complex.

Level 1: Participant Reaction
-
Attendance: 15 participants from four countries, attended sixteen hours of online education. Participants included nurses, physiotherapists, doctors and early career health professionals/researchers.
-
Participant reaction was evidenced by immediate and post-event experience survey and free-text feedback. Illustrative quotes:
-
“The interactions with the entire group from varied backgrounds and geographies were quite insightful. Theoretical knowledge on teaching was very helpful,” and “I learned a lot from how the course was delivered and the interactive nature of the training”.
-
All participants reported that their knowledge and confidence to teach online had increased and feeling more motivated and confident than before the course to run a Tier 2 education programme.
-
Level 2: Participant Learning
-
A post-event knowledge survey (S3 in online supplementary material) consistently indicated improvements across all participants (n=15) in knowledge and confidence related to:
-
Identifying learning needs, learning theory, designing a learning event and engaging learners.
-
Patient selection and assessment, properties and conduct of field-based walking tests, fundamentals of exercise prescription, and aerobic training.
-
Knowledge and confidence in stakeholder mapping and behaviour change models.
-
Level 3: Organisational dimensions (factors which are critical to or can hinder/ prevent impact)
-
Participants presented proposals for PR education programmes, as well as how they plan to transition their programme into tier 2 and tier 3, which addressed specific features of local healthcare systems.
- For example, how to engage and influence across public/private healthcare sectors (India - Pune)
Level 4: Participants use of new skills and knowledge
-
Participants developed feasible proposals for PR services and tier 2 & 3 education programmes adapted to their local context and demonstrated leadership to engage and influence multiple professional groups and stakeholders. Presentations were observed and recorded by RECHARGE-IPCRG Faculty, who provided feedback to participants.
- Proposals included cultural adaptations to support changes, such as nutritional support (Sri Lanka), incorporating the arts into PR, including dance (Kyrgyzstan) and singing (Sri Lanka), and other cultural adaptations like Yoga (India).
Level 5: Impact on participant practice and on service users
-
Participants completed baseline qualitative work prior to TtT to examine the feasibility and acceptability of a national PR programmes.20–22
-
We continue to support participants to track implementation and to explore impact evaluation using narrative and standardised data collection.23
-
RECHARGE-IPCRG Faculty will provide ongoing mentoring.
-
Five abstracts on implementation were presented to the IPCRG World Conference in May 2022.24–28
DISCUSSION
‘Train the trainer’ or ‘cascade’ training has been widely proposed as a method for capacity building and strengthening health systems, by upskilling local experts and clinicians to offer peer-to-peer training and mentoring.15 It has been argued that a cascade approach oversimplifies a complex capacity-building process and often has a short-term horizon, raising questions over the effectiveness of training and longer-term sustainability - it has also been noted there is a lack of empirical evidence on the topic.15
Teach the Teacher (TtT) is an educational intervention which seeks to develop the capacity for teaching subject-specific knowledge and skills through a cascade approach, but offers an enhanced framework, which addresses the criticisms cited above. Through various iterations of the programme, we have enhanced and extended our understanding of capacity building in primary and respiratory care.16–18 This paper reports on our observations and experience of the IPCRGs TtT programme, which involved collaborating with the National Institute for Health and Care Research (NIHR) Global RECHARGE Group. It contributes to a larger body of work and practical knowledge concerning sustainable capacity-building models.
We proposed a three-tier cascade programme (Figure 1) of education adapted for PR. We successfully engaged an expert RECHARGE-IPCRG Faculty and five teams from four countries to develop in-country evidence-based education programmes for developing PR programmes. There were specific adaptations to the programme design, resulting from the need to transfer to a digital learning environment due to the SARS-CoV-2 pandemic. This was achieved through changes to learning design and supporting infrastructure for Faculty and participants. There was a deliberate balance between clinical content (teaching the important elements of PR) and process (how the Country Master Teachers would subsequently teach to their clinical colleagues).
Our evaluation demonstrated that in-country teachers are highly motivated to develop in-country programmes building on previous participation and baseline work in the RECHARGE project. Each country now has a cohort of ‘In Country Teachers’ trained in PR and plans for an education programme adapted to their national context. Educational resources have been developed which can be used to sustain this work. There is increased confidence to offer PR to patients in clinical practice and to design and lead programmes of PR education. In-country teachers have the potential to develop PR services and, through repeated programmes, strengthen their teaching and expertise. In-country teachers were also highly motivated to influence policy and practice changes.
We have sought to address the lack of empirical evidence concerning capacity-building initiatives by being explicit about the faculty’s work together on learning design and management of the programme and to elucidate a model of evaluation. This is practice-based knowledge,29 which is sometimes neglected in traditional forms of academic literature - but is an important contribution for those tasked with designing and leading capacity-building projects.
At this stage, longer-term programme evaluation is inconclusive but suggests potential in developing PR services. It is unclear which factors or conditions contribute to success, as economic, political and social contexts are all significant variables.30 There are commonalities in broad aims and challenges across partner countries, substantive differences in organisational, functional, professional, and service integration and population focus. These differences are useful in understanding the varied forms that implementation can take. Future research that tracks PR implementation at a service and/or population level is needed and will provide important lessons for service providers and policymakers seeking to build capacity for PR.
CONCLUSIONS
The RECHARGE-IPCRG TtT programme provided a clear education and service development framework to support PR capacity development in LMIC. High-quality teaching programmes can support the implementation of PR in LMIC, where demand greatly exceeds capacity. The RECHARGE-IPCRG TtT programme combined educational, and PR service development concepts with core clinical content adapted for project partners and a digital environment. Local leaders in PR can develop context-specific tiered education programmes to develop a critical mass of expert teachers and PR practitioners. RECHARGE-IPCRG TtT can be successfully adapted to an online environment using various teaching methods and digital tools, which can meet the needs of diverse international participants. A whole system perspective to PR allowed consideration of health systems, culture, referral pathways and scalability.
Acknowledgements
The authors would like to acknowledge Siân Williams, CEO of IPCRG for her valuable contribution in conceptualising, setting up and leadership of the RECHARGE TtT project.
Funding
This research was funded by the NIHR (17/63/20) using UK aid from the UK Government to support global health research. The views expressed in this publication are those of the author(s) and not necessarily those of the NIHR or the UK government. Professor Singh is a NIHR Senior Investigator. The views expressed in this article are those of the author(s) and not necessarily those of the NIHR, or the Department of Health and Social Care.
Authorship contributions
NB, MO, AB and SJS conceived and established the programme. JM, MO, LHW, NB, AB, JCS, IT, NG were the RECHARGE- IPCRG Faculty who designed and led the TtT programme and evaluation. TS, BK, SW and SS are PIs. AA, GM, MM, RK, WW, TA, MS, RK, RI, OA, HH, PD, DT, SS, MB are the in-country Teachers and participants of the TtT programme. JM conducted the analysis and wrote the first draft. All authors contributed to the final draft and checked for the content. All authors approved the manuscript as submitted.
Competing interests
The authors completed the Unified Competing Interest form at http://www.icmje.org/disclosure-of-interest/ (available upon request from the corresponding author) and declare no conflicts of interest.
Corresponding Author:
Dr Mark Orme PhD, Lecturer, Department of Respiratory Sciences, University of Leicester, University Road, Leicester, LE1 7RH, UK. [email protected]