
Non-communicable diseases (NCDs), primarily cardiovascular disease, cancer, chronic respiratory disease, and diabetes mellitus, are the leading causes of mortality worldwide.1 Globally, NCDs accounted for 41 million of the 55 million deaths reported in 2019.1 NCDs pose a greater threat to low- and middle-income countries, where more than three-quarters of global NCD deaths occur.2 This silent epidemic fosters poverty, hinders economic development and sustainability, and is perilous for health systems, health equality, and thriving communities.3 Unless prevention and control interventions are implemented in primary health care (PHC), global NCD mortality rates are projected to reach 52 million by 2030.4
The World Health Organization (WHO) outlined a framework for the management of NCDs in low- and middle-income countries in the 2013-2020 Action for the Global Strategy for the Prevention and Control of Noncommunicable Diseases.5 This global strategy includes implementing Healthy Lifestyle Centers (HLCs), which integrate a community-based approach to research, education, prevention, and treatment of NCDs.5,6 HLCs serve not only to treat disease and illness, but also to address the physical, mental, social, and spiritual well-being of individuals and communities.
After World War II, Dr. Andrija Štampar, one of the founders of the WHO, proposed that to best address the needs of agrarian regions, rural health centers should be created. These health centers would reduce the need for patients to travel long distances and ensure that healthcare providers were well aware of the environment in which their patients lived. The local understanding of healthcare workers in these clinics would allow them to focus on the positive aspects of healthcare that are necessary to prevent and manage NCDs, such as better food, physical activity, health education and medical care. This essential approach is now conceptualized through the WHO as the HLC.7,8
Similar to other low- and middle-income countries, Nepal is currently in a transition from infectious diseases to NCDs as a major public health concern, which poses a significant burden on its under-resourced health system.9,10 WHO currently estimates 66% of all deaths in Nepal are due to NCDs.11,12 According to the WHO 2022 NCD Progress Monitor, the total number of NCD deaths in Nepal is 117,300, with higher rates in women than in men.11,12 Additionally, there is a 22% probability of premature mortality from NCDs.12 However, many areas of the country still lack baseline information on the prevalence of NCDs and underlying risk factors.9,10,13
Nepal’s PHC model provides services centered on treating infectious diseases, with NCDs identified primarily through health facility-based screenings.9,10,14 These centers are ill-equipped to manage the long-term chronic care needs and comorbidities associated with NCDs.14 A 2020 report projected that on the current course, NCDs will contribute to the highest proportion of deaths in Nepal by the year 2040.15
The rising burden of NCDs in Nepal demonstrates the crucial need to integrate HLCs into PHC delivery to reduce the prevalence of NCDs, mitigate existing pathologies, and assess risk factors.13,16,17 PHC must be restructured to integrate HLCs to improve public health and meet the goals of the WHO Global Action Plan for the prevention and control of NCDs.16,18
Like other low-income countries, Nepal has historically been ineffective in their response and management of public health emergencies, with the NCD epidemic being a prime example. Decades of political instability has exorbitantly burdened Nepal’s health system and weakened its resilience to health crises. An environment of such turbulence is at risk of collapse.19 In addition to political turmoil, challenges and opportunities to the development of HLCs in Nepal include: (1) resource scarcity, (2) low health literacy, (3) poor insurance coverage, (4) high out-of-pocket expenditure, (5) shortage of trained medical professionals, (6) access inequality, (7) insufficient health care services, (8) increasing rates of workplace violence against health care workers, and (9) lack of unified agenda between government and private stakeholders.19,20 These barriers, all exacerbated by the Covid-19 pandemic, greatly influence the successful implementation, execution, and delivery of HLCs in Nepal.19
Good Health Nepal (GHN) was founded in 2013 and currently operates (in cooperation with governmental health care services) both permanent and outreach clinics in the Thaha municipality of the Makawanpur District in central Nepal. The clinics are staffed by volunteers and Nepali medical providers trained by Acupuncture Relief Project (ARP), a US 501(c)(3) nonprofit organization that works collaboratively with GHN. GHN/ARP, with a prioritization on patient education and prevention, has provided simple, practical, safe, evaluation and therapy to more than 500,000 patient visits within the clinics’ catchment area in the Makawanpur District since it began (Figure 1).

In 2018, GHN conducted a population survey in rural Nepal in alliance with the Nepal Health Research Council, Social Welfare Council of Nepal, Makwanpur District Health Office, and Thaha Municipality. Utilizing the WHO STEPwise model, the survey was conducted in five wards of the Thaha municipality to assess baseline NCD prevalence and risk factors. Several areas of concern were revealed, including respiratory disease, stage 2 hypertension, obesity, tobacco use, alcohol use, and chronic pain, representing a significant burden on current available health services.21
Objective
GHN received governmental approval in 2016 to become the first integrated HLC in Nepal. As the first of its kind, the scope of practice and operational authority are not well defined. The purpose of this paper is to document GHNs current operational model for evaluation and implementation at the PHC level in rural Nepal. The proposed integrative model is cost-effective, easily replicable, and highlights the need for comprehensive and sustainable care, NCD prevention and education with effective treatment, case management, community-centered care, referral networks, and telemedicine. This model supports the future establishment and operation of all HLCs in Nepal.
Governance
HLCs serve as adjunctive PHC facilities, providing complementary and overlapping services to the existing health system. They deliver medical advice, diagnosis, and treatment for both acute and chronic conditions, prioritizing preventive health education, palliative care, dietary changes, exercise, and other lifestyle modifications. Once established, clinical operations should be overseen by the following organizations: Nepal Health Research Council (NHRC), Nepal Health Professionals Council (NHPC), Department of Health Services (DOHS), and respective District Health Offices in Nepal. Peer-to-peer authority between providers, across platforms and among various facilities should be established to maximize service delivery and community-based resources, strengthen access to rural populations, enhance transparency and accountability, and cultivate organizational partnerships.
Leadership and staff
Chief of primary health center
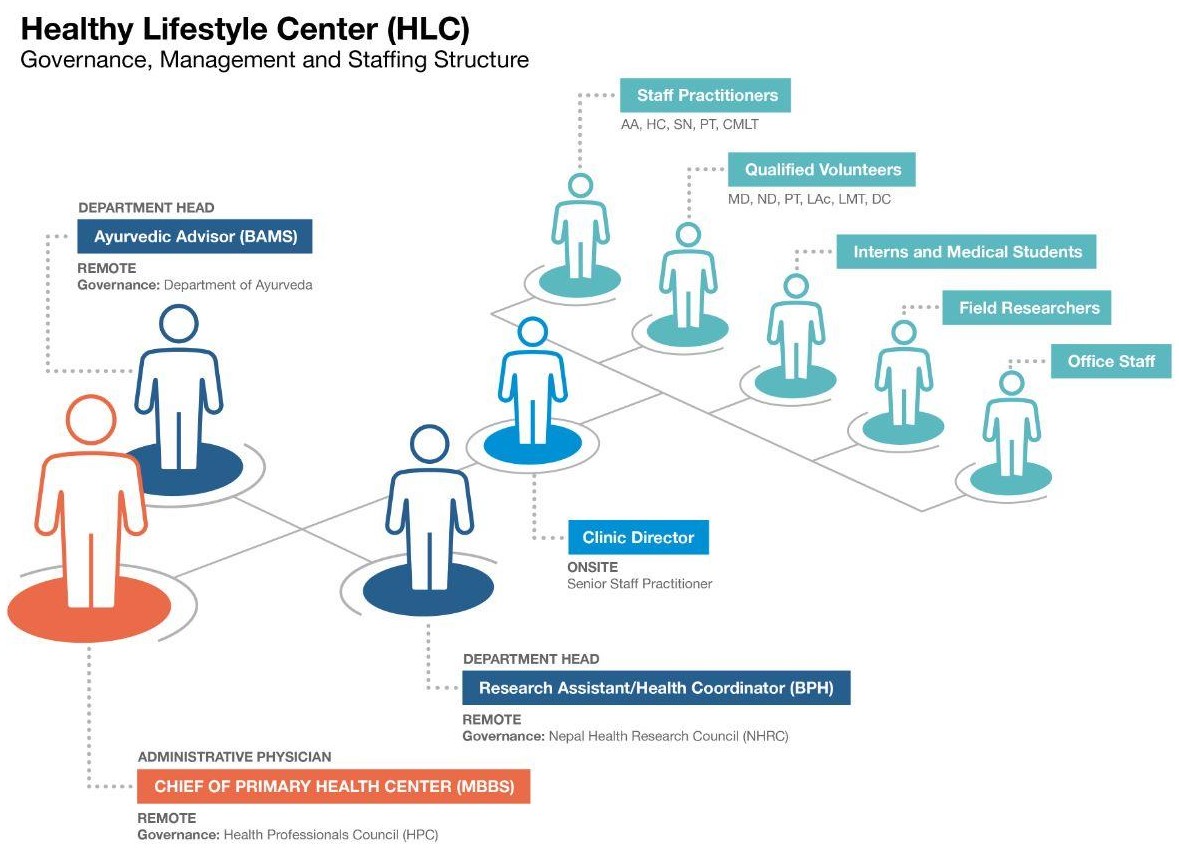
Primary governance under NHPC provides each HLC with greater autonomy and requires oversight by a Primary Health Center Chief Physician (CP) with a Bachelor of Medicine and Bachelor of Surgery (MBBS). The CP is responsible for daily clinical operations and strategies. The CP also provides medical oversight to HLC practitioners and is the deciding authority on diagnosis, treatment, patient care, and case management. Working predominantly via telemedicine, one Chief Physician can simultaneously support several HLC clinics.
Department heads
Department Heads include an Ayurvedic Advisor with a Bachelor of Ayurvedic Medicine and Surgery degree (BAMS) and a Research Assistant/Health Coordinator with a Bachelor of Public Health degree (BPH). The Ayurvedic Advisor is responsible for the safe and ethical application of Ayurvedic modalities and oversees practitioners licensed by the Department of Ayurveda. Serving as a liaison between the NHRC, District Health Office, and GHN, the Research Assistant/Health Coordinator is responsible for evaluating research priorities and opportunities, overseeing research designs, guiding program development, fostering community partnerships, and strengthening health policy (Figure 2).
__governance__management_and_staffing_structure.jpg)
Department Heads operate remotely to maximize cost-effectiveness and deliver sustainable support across multiple clinics. To provide oversight for a broad application of HLCs, Department Heads should be provisioned by provincial, district or municipal governments. Alternatively, they could be provisioned by individual clinic facilities, rural municipalities, or non-governmental organizations (NGOs) to provide services to select areas.
Permanent staff
Staff practitioners provide on-site support to treatment facilities year-round. They are the primary source of medical advice, assessment, and diagnostics for the communities they serve. Staff practitioners could include any combination of the following disciplines, as determined by the CP, on-site clinical director, and the needs of the community: Acupuncturist (AA), Health Assistant (HA), Physical Therapist (PT), Staff Nurse (SN), Lab Technician (CMLT), and Office Helper (OH). A clinical director will oversee staff practitioners and day-to-day operations on-site, and report directly to the CP.
Qualified volunteers
Qualified foreign and domestic practitioners serving as volunteers augment and/or complement services provided by staff practitioners. These volunteers may include Medical Doctors (MD), Doctors of Naturopathic Medicine (ND), Physical Therapists (PT), Licensed Acupuncturists (LAc), Licensed Massage Therapists (LMT), and Doctors of Chiropractic (DC) They operate under the guidance of the department heads and permanent staff.
HLCs utilize Female Community Health Volunteers (FCHVs) acting under the auspices of the Family Health Division at the Ministry of Health and Population (MoHP). These local women provide frontline community-based health education and services in rural areas, with an emphasis on maternal and child health and family planning. FCHVs serve as liaisons between primary care facilities and community members, making them integral to enhancing community mobilization, patient referrals, health screenings, and follow-up care.
Interns and medical students
HLCs may serve as training facilities for medical students and/or employ interns for any authorized modality to help train HLC practitioners for other clinic sites, under the guidance of the CP and permanent staff.
Scope of practice
Consultation services
HLCs are the primary source of medical advice, assessment, and diagnostics for their communities. Practitioners mobilize and deliver appropriate resources to patients with both acute and chronic pathologies. Services include NCD primary assessment, emergency assessment, NCD case management, palliative end-of-life care, medication management, patient education, lab analysis, dietary advice, lifestyle advice, and first aid. Services are tailored towards individual and community needs.
Therapeutic (treatment) services
Patient visits at HLCs consist of simple, practical, safe, low-cost, and sustainable therapies and include screening for modifiable risk factors of NCDs. Cost effective, evidence-informed therapies, such as acupuncture and botanical medicines, naturopathy, physical therapy, Ayurveda, chiropractic, massage, yoga, meditation, assistance and support with over-the-counter medications and wound care are used as interventions when needed. HLC treatments are delivered in a community setting that provides valuable social engagement, coordinates care between healthcare providers, and maximizes patient numbers to maintain low-costs. However, when more complex care or technology is necessary, HLC staff and volunteers will refer up the care ladder to PHC facilities, hospitals, or other medical specialists and will consult the CP as needed.
Naturopathy is a system of primary care with emphasis on disease prevention and natural therapies. Therapeutic modalities also may include physical manipulation, botanical medicine, clinical nutrition, homeopathy, hydrotherapy, and prevention and lifestyle counseling.22 NDs require a doctoral degree from an accredited four-year medical school, a passing score on the Naturopathic Physicians Licensing Examinations (NPLEX), and active licensure equivalent of an MBBS.22
Acupuncture, in particular, is easy to teach to other healthcare workers and does not depend on medication availability, making it a low-cost method for the treatment of many conditions, including acute and chronic pain.
While utilizing evidence-informed, natural therapies, practitioners will refer to the WHO Package of Essential Noncommunicable (PEN) Disease Interventions for Primary Health Care to effectively detect, diagnose, treat, and manage patients with NCDs. Additionally, WHO PEN protocols will guide early diagnosis of cancer, palliative care, and healthy lifestyle education. WHO PEN offers an integrated approach to NCD prevention and control in low-resource environments, making it a useful tool for HLCs in rural areas.23 The WHO HEARTS Technical Package is a strategy for improving cardiovascular health. The six modules in the package can be used to train providers in cardiovascular standard of care and disease management.24 As providers become more aware and knowledgeable about the rural areas where clinics are located, this information will be used to instruct a co-creative process with HLC leadership that results in a consensus protocol for HLC treatment of high blood pressure. Both of these tools have been created for use across a multitude of environments and can be modified to adjust for resource scarcity or availability as needed.23,24
Data collection and research
Currently NCD data on patient demographics, NCD type, prevalence, and regionally-specific risk factors is limited, particularly in rural areas. Therefore, robust data collection is necessary to build a network of lifestyle clinics in Nepal. HLCs will establish baseline data through field research surveys, as outlined in the WHO 2014-2020 Multisectoral Action Plan for Prevention and Control of NCDs,25 which highlights systematic data collection at the primary care level (surveillance, research, monitoring, and evaluation) as a key component for tracking NCD prevalence and risk factors.25
In addition, HLCs will use permanent medical records. Like many other low-income countries, Nepal’s current national health system uses paper-based medical records (MRs). Each patient is responsible for storing their MR, typically at home along with other important documents, and carrying it to each visit. Patient compliance is low, and chart notes are often lacking, which leaves significant gaps in patient health history, disease diagnosis, active medications and dosages, patient outcomes, labs, etc. MRs, in their current state, do not accurately reflect the current health status of each patient or their history of care. A permanent MR system allows HLCs to maintain accurate patient records, deliver safe treatment, and effectively collect and track NCD data. MRs will be created for each patient and stored onsite at a permanent facility.
Implementing a permanent medical record system on-site at permanent facilities allows HLCs to collect patient data at each visit and track qualitative trends over time. HLC data collection is an effective tool for scaling up NCD management by providing information on early detection, screening, timely treatment, and high-impact intervention protocols. Additionally, the robust collection of data from primary facilities enhances accurate government reporting and supports the operation of future HLCs in Nepal.
Referral resources
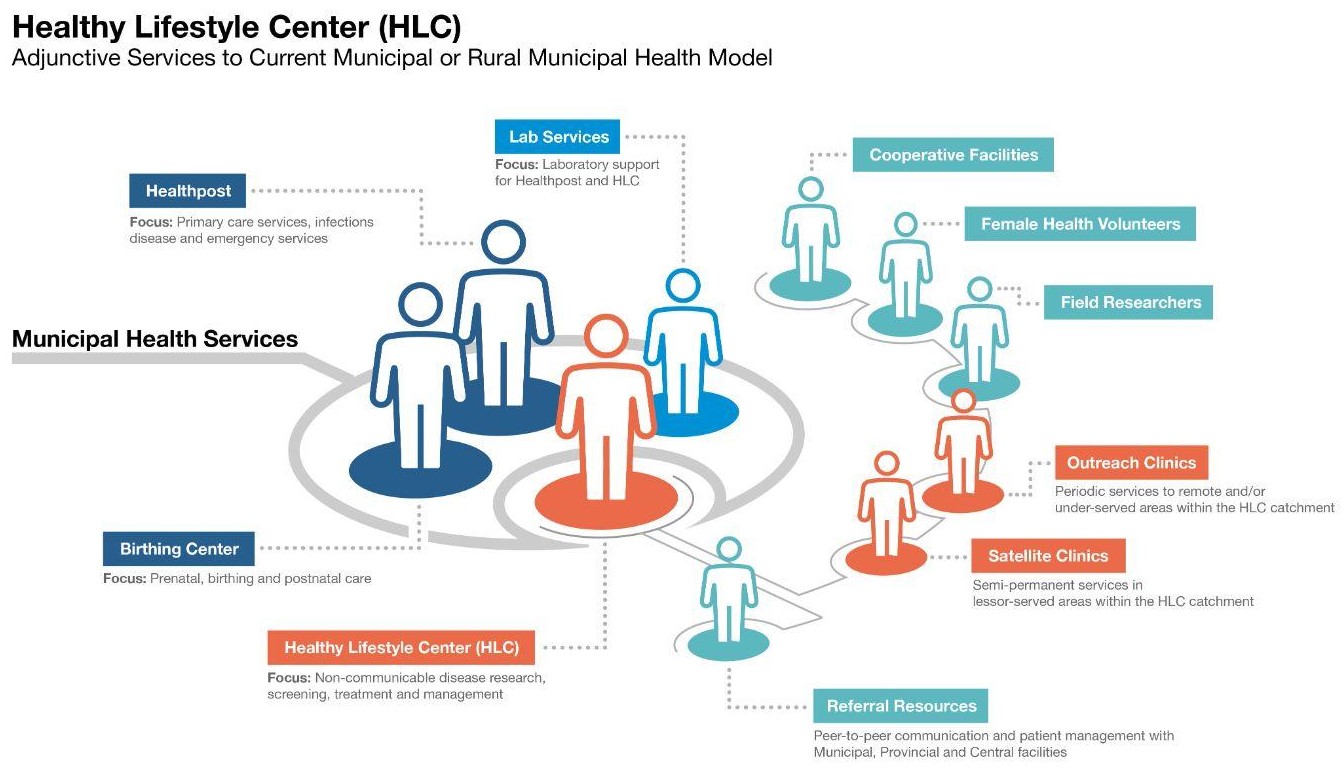
Developing sustainable linkages between HLCs and local resources (health posts, primary care facilities, regional hospitals, and central hospitals) will require HLCs peer-to-peer referral authority to such facilities (Figure 3).
Facilities
Primary clinics
HLCs will operate in one permanent facility (ideally within a governmental health post compound), (Figure 3), providing low-cost primary care evaluation and therapies to local populations. Permanent facilities should serve a rural catchment area of at least 5,000 people within a two-hour walking radius. Facilities must be at least 1000 square feet, capable of accommodating 2-4 therapists working simultaneously, and serve 40-100 patients per day.
__adjunctive_services_to_existing_municipal_health_model.jpg)
Satellite and outreach clinics
Satellite and outreach clinics in Nepal’s rural areas have proven beneficial in delivering care to isolated populations. These clinics provide HLC services to rural residents living far from primary facilities and raise community awareness about available services. Satellite clinics provide regular care to the surrounding community, can be established using available space in community buildings, and should accommodate two practitioners. Outreach clinics provide episodic mobile acres to more isolated villages and can be set up using medical tents, etc. in village schools or other public spaces. These facilities are staffed by HLC practitioners who travel to the site on a regular basis to administer services as needed while surveilling the population for NCDs and risk factors.
While reducing the need for patients to travel long distances, satellite clinics also enable healthcare providers to garner important knowledge about the unique environment in which patients live. The knowledge gathered through the HLC will provide feedback that benefits the entire healthcare system. This enables a unique response, in the spirit of the health center promoted by Dr. Štampar that is geared towards individuals in specific regions of Nepal.26
Cooperative facilities
Cooperative facilities may be governmental or private. HLCs may establish partnerships with cooperative facilities, which provide space and salaries in return for HLC trained personnel, supplies, and oversight.
Cost-effectiveness
Serving as a complementary adjunct to the existing primary care system, the proposed integrative HLC model offers a low-cost, high-impact, and sustainable approach to NCD management and prevention in rural Nepal. It is a cost-effective and easily replicable community-based model that can be implemented by governmental and non-governmental organizations providing primary care to populations in rural areas.
Telemedicine/decentralized oversight
Decentralized oversight by department heads is a cost-effective method of streamlining patient care and HLC service delivery. Fulfilling this role on-site is associated with higher costs due to long travel times to multiple clinics. Utilizing telemedicine, department heads can simultaneously provide clinical oversight to multiple facilities and timely care to more patients in all locations. Department heads oversee centralized therapists at remote sites in managing patients across a broad spectrum of complex conditions.
Public health surveillance
Nearly 70% of all visits to a primary care facility are for pain complaints. The cost of chronic pain to a health system and to a person’s overall quality of life is high.27–29 Thus, coupling a low-cost modality like acupuncture for the management of chronic pain with frequent health screening provides a unique opportunity for the HLC. Patients are able to access services that they are in need of, and the HLC is better able to surveil the population for NCDs and risk factors without additional costs.
Prevention
The direct and indirect expenses of NCDs are depleting Nepal’s economy, resulting in significant financial and social burden on patients, families, and caregivers. NCDs lower productivity and human capital while driving up healthcare expenditures due to chronic illness, disability, and death. Missed diagnoses and treatment have exacerbated the burden of NCDs. A preventative approach to NCD management assures fiscal sustainability of Nepal’s health system and secures significant economic benefits in the short and long term. Focusing on preventative healthcare allows HLCs to identify the most pressing risk factors and inform interventions such as NCD screenings, health education, palliative care, dietary changes, exercise and other lifestyle modifications. This allows HLCs to identify early stage NCDs, which reduces long term care needs for medications and specialized care.
Barriers to development
Currently, there are a number of barriers to successful HLC implementation in Nepal. To successfully implement this model, several policy measures have to be taken simultaneously: (1) HLCs need to be authorized and defined by the MoHP, (2) The NHPC needs to define, establish scope of practice, and authorize Acupuncturists as a distinct and protected health profession, and (3) Provincial health authorities need to recognize the value of HLCs as an adjunct to existing health services and provision for their development.
Currently Acupuncture is only recognized at a certificate level with many practitioners studying abroad for advanced degrees. This is unsustainable and will not yield an adequate supply of skilled manpower to staff HLCs. Improvement is needed in acupuncture schools currently operating in Nepal. They are inadequate in providing competency in NCD screening and management and their education needs to be extended to a Bachelor’s level. Other health professionals in Nepal also need additional awareness and training in management and screening of NCDs.
Conclusions
The WHO’s global strategy for addressing NCDs such as cardiovascular disease, cancer, chronic respiratory disease and diabetes mellitus includes the implementation of HLCs. HLCs reduce the risk of NCDs by working with individuals and communities to establish healthy lifestyle environments and to screen for modifiable risk factors of NCDs. HLCs mitigate existing pathologies through the provision of patient-centered care that includes routine and emergency assessment, first aid, medication management, education, lifestyle and nutrition counseling, appropriate life-stage care, low-cost treatment modalities (i.e. acupuncture and botanical medicine), and referral up the ladder of care to more complex services when necessary.
The clinics that GHN/ARP are currently running in cooperation with government healthcare services are a proven working model for HLCs in Nepal. These clinics have provided over half a million patient care visits in the Makwanpur District, addressing conditions that include respiratory disease, hypertension, obesity and chronic pain. The GHN/ARP model can be implemented as HLCs at the PHC level in rural Nepal with the establishment of a leadership team that includes: a Primary Health Center Chief Physician, an Ayurvedic Advisor, and a Research Assistant/Health Coordinator. Staff practitioners are chosen by the leadership team and assist with the oversight of qualified foreign and domestic volunteer practitioners. HLCs and FCHVs collaborate for improved maternal and child healthcare.
Clear communication routes and referral standards between HLCs and local health resources (e.g., hospitals) must be established to maximize service delivery and care partnerships. HLC medical records will be tracked and stored onsite at a permanent facility where they are accessible for care coordination. HLCs will add to data collection by continuing the field research begun by GHN that tracks the NCD picture in Nepal.
The GHN operational model described here is an easily replicable, cost-effective approach to HLC implementation at the PHC level in Nepal. The prototype demonstrates leadership, awareness, and commitment to rural primary care that has the potential to contain the rising burden of NCDs and improve the quality of life for the individuals and communities that call Nepal their home.
ACKNOWLEDGEMENTS
We would like to thank Nepal Health Research Council, Nepal Social Welfare Council and Makwanpur District Health Office for their valuable contributions to the material presented.
FUNDING
This research project is financially supported by Acupuncture Relief Project, Inc., a 501(c)3 non-profit organization (ID: 26-3335265). The content of the publication is the sole responsibility of authors (independent researchers) and does not necessarily reflect the position of the organization.
AUTHORSHIP CONTRIBUTIONS
Content material and conception of the presented model: AS, BG. Original manuscript: AS, AW. Review of the manuscript: BG, RG. Editing of the manuscript: AS, AW, RG.
COMPETING INTERESTS
The authors completed the Unified Competing Interest form at www.icmje.org/coi_disclosure.pdf (available upon request from the corresponding author) and declare no conflicts of interest.
CORRESPONDENCE TO:
Acupuncture Relief Project, Vancouver, WA, USA, [email protected]