
The coronavirus disease 2019 (COVID-19) health crisis had uneven effects across nations and population groups. Older adults (OA) are especially susceptible to severe disease and death from COVID-19.1 Old age is accompanied by a significant decline in functional, psychological, economic and social capabilities and preexisting health conditions,2 rendering OA a high-risk group from the beginning of the pandemic. Measures to contain the spread of the virus were prioritised to reduce the number of infections among OA, because mortality in this population group was higher than in younger and middle-aged adults.3 Nevertheless, these measures adversely impact the physical and mental health of OA.4,5
The aging process and preexisting health conditions lead to reduced mobility and access to activity spaces in OA. For this reason, public spaces play an important part in meeting their needs, especially the need for social contact and conviviality.6 In OA, decreased mobility may contribute to the increased prevalence of digestive diseases, such as constipation, which is one of the most common digestive system complaints in older adults.7 Constipation is widespread in the general population,8 and in OA, it can contribute to the deterioration of quality of life (QoL).9 QoL is a multidimensional concept that includes both observable and self-assessed aspects and where the subjective component is strongly conditioned by individual experience in a specific social and spatial context10; this is why closed public spaces; readjusted daily activities; restricted physical contact with family, friends and neighbors; and mobility may have degraded the life experience of OA during the pandemic. This study reports on the perceptions of their QoL by OA, their adherence to prevention measures, the impact of social distancing measures on their mobility, social relationships, daily activities and eating habits, and the prevalence of constipation.
Methods
Setting
A cross-sectional study with a mixed approach was conducted, with data collected using an online instrument that targeted adults aged 60 years and older. This instrument was designed in the FORMS application of the Microsoft Teams platform. The link was distributed across the social networks Facebook, WhatsApp, and email to the personal contacts of the research group members, inviting them to share the link. Electronic informed consent was integrated into the presentation section of the survey, and the anonymity of the responses and confidentiality in handling and analysing the data was guaranteed to the participants. The survey was available from November 1, 2020, to May 31, 2021. During the second wave of COVID-19 in Mexico, voluntary social isolation was the most important measure implemented for the protection and care of the elderly.
Study participants
Our study included 114 adults aged 60 years and older. The number of participants was influenced the call made by the research group and the access of OA to the media througt which the instrument was disseminated. The study was approved by the Research Ethics Committee (Pro1MC-01052021).
Survey
The research instrument included the entirety of the World Health Organization’s Quality of Life in Older Adults Scale (WHOQOL-Old)11 in its validated version for the Mexican population12,13; the Rome III Criteria14 for chronic functional constipation; and questions from the Bristol Scale15 on the prevalence of chronic degenerative disease, fear of infection, adoption of preventive measures for SARS-CoV-2, sociodemographic characteristics, and perceived degree of impairment of mobility, social interaction, and activities of daily living due to the pandemic. Adults aged 60 years and older who had access to the survey and chose to participate were included.
The WHOQOL-Old Scale11,12 is an instrument including 24 items with responses given on a five-point Likert scale, equally distributed across six dimensions: sensory abilities, autonomy, past, present and future activities, social participation,; death and dying, and intimacy. The scores for each dimension range from 4 to 20 points. The total score for the scale is between 24 and 120 points, and the higher the score, the higher the QoL.11,12
The Rome III criteria14 are used to diagnose chronic functional constipation. These criteria include the presence of at least two of the following symptoms over more than three months, such that in at least every fourth bowel movement, there is straining to defecate, the presence of hard stools, a sensation of incomplete evacuation, a sensation of anorectal obstruction, the need for manual manoeuvres to facilitate bowel movements or fewer than three bowel movements per week.14
The Bristol Scale15 is used to study gastrointestinal disorders to observe stool consistency, allowing descriptive and graphic evaluation of stool types.14 This instrument makes it possible to establish a relationship between stool consistency, stool form, and discomfort during defecation. The scale comprises seven types of stool based on their shape and hardness: type 1 is the hardest, and type 7 is the most liquid. Types 1 and 2 correspond to constipation.15
To measure adherence to SARS-CoV-2, a list of nine preventive measures was created, and participants selected those they had followed during the pandemic.
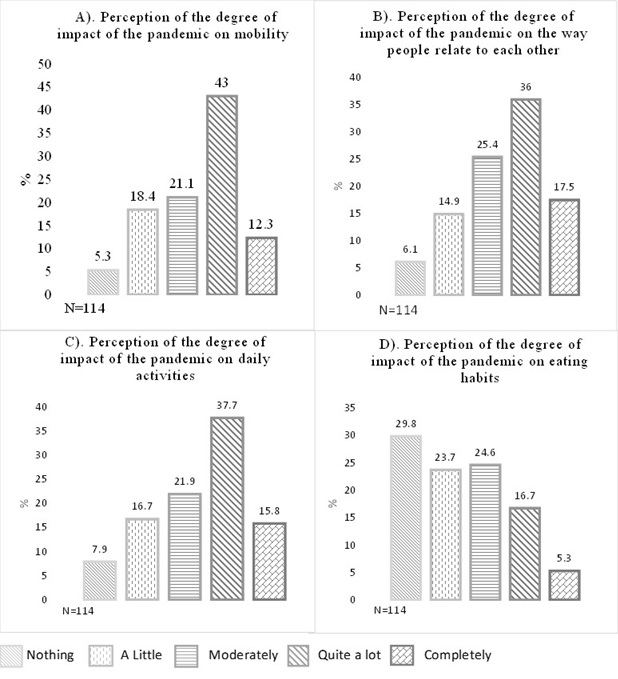
Perceptions of the impact of the COVID-19 pandemic on mobility, daily activities, relationships, and eating habits were collected by asking participants to describe how the pandemic had affected each of these aspects.
The sociodemographic variables collected by the research instrument were age, sex, marital status, schooling, religion, and occupation. The prevalence of several diseases (hypertension, diabetes, obesity, smoking, chronic obstructive pulmonary disease, cardiovascular disease, chronic renal failure, asthma, and immunosuppression) was also indicated.
Statistical analysis
This information was used to create a data matrix in IBM SPSS®, version 20. Frequencies and proportions were estimated using qualitative and quantitative variables (as means and standard deviations). Student’s t-test for independent samples was used to compare the global scores obtained in QoL based on sociodemographic characteristics: sex, having a partner, suffering from a chronic degenerative disease, fear of contagion, considering oneself a person with constipation, and identifying two conditions for the diagnosis of chronic functional constipation. Analysis of variance (ANOVA) of one-factor tests was used to compare the overall score obtained on the WHOQOL-Old scale between groups based on: marital status (single, married, widowed, and separated), low (junior high school or less) and high (high school or more) schooling, religion (Catholic, non-Catholic, and no religion) and occupation (employed, unemployed, and retired). The relationship between variables was estimated with Pearson’s correlation coefficient. Finally, linear regression was used to predict QoL from the variables examined in the study. Qualitative methodology was used to analyse discourses related to perceptions of the impact of the pandemic on mobility, relating to others, daily activities, and eating habits. The data management procedure used in this section began with the typification of the discourses, which involved the treatment of the data obtained before the data were entered into the Iramuteq version 0.7 software for processing. Once the data were entered, the discourses were schematised, which produced a synthetic figure that supported subsequent analysis. In the final stage, the discourses were analysed by category, with description and discussion using graphic support for the core and periphery of the discourses that revolved around QoL and its constituent spheres.
Results
A total of 178 people responded to the online form, of which 64 were excluded because they did not meet the age criteria. No incomplete responses were recorded in the instrument. The participants in this study (114 OA) ranged in age from 60 to 99 years (mean = 68.89 ± 7.97). Of these, 59.6% (68) were women, 55.3% (63) lived with a partner, 54.4% (62) had little schooling (primary and secondary), and 81.6% were Catholic. At least one preexisting health condition (hypertension, diabetes mellitus, obesity, smoking, chronic obstructive pulmonary disease, cardiovascular disease, chronic renal failure, asthma, or immunosuppression) was reported by 63.2%, the most prevalent being hypertension (56.9%), diabetes mellitus (23.6%), and obesity (12.5%).
The total QoL scores ranged from 51 to 118, with a mean of 89.06 ± 13.83. The dimensions of intimacy and social participation had the lowest QoL scores. The 60 to 79 age group had a higher mean score (91.1 ± 12.20) than the 80+ year age group (74.36 ± 16.26). 78.1% of the participants considered that the COVID-19 pandemic altered their QoL. The QoL scores dimensions of autonomy, intimacy, past, present, and future activities, and sensory abilities in the 60 to 79 year age group were different QoL scores the 80+ year age group applying Student’s t-test for independent samples (Table 1).
The mean QoL scores in relation to basic characteristics and demographic attributes are observed in Table 2. Significant differences in the QoL of the associated groups were observed for preexisting health conditions, living with a partner, having abdominal distension, and being self-assessed and/or classified as constipated by Rome III criteria.
The comparison of the mean QoL scores based on the variables of marital status, educational level, occupation, and perception of the impact of the pandemic on the form and frequency of their bowel movements (ANOVA of one factor and Tukey’s Post Hoc test) allowed us to observe statistically significant differences between the means for the married and widowed segments of the population (P=0.040) with education in terms of primary and undergraduate studies (P=0.004), primary and postgraduate studies (P=0.050), and employment in terms of retired and unemployed people (P=0.025).
The experience of fear of COVID-19 infection was reported by eight out of 10 OA in the segment of the population that was evaluated (79.8%). QoL of those who experienced fear of contagion was equal to the quality of life of adults who did not experience it, applying the Student’s t-test for independent samples.
The SARS-CoV-2 preventive measure most frequently self-reported by OA was frequent hand washing (98.2%), and the least adopted was disinfection of frequently touched surfaces (Table 3).
Using Pearson’s correlation coefficient, a moderate and negative relationship was found between the age and QoL (r=−0.439, P<0.001); a weak and positive relationship was found between years of schooling and QoL (r=0.350, P<0.001); a weak and negative relationship was found between QoL and the number of conditions for constipation (r=−0.279, P = 0.003) and for the number of days with bloating (r=−0.347, P<0.001); and finally, a weak and positive relationship was found between QoL and the number of preventive measures taken (r=0.331, P< 0.001). All correlations were significant at the 0.01 level.
Taking these correlations and using linear regression (r = 0.603), the following predictive model was constructed: Y = 106.023 − 0.449 (age) + 0.597 (years of schooling) − 1.687 (days with abdominal distension) + 1.423 (number of preventive measures taken). This model explains 36.4% of the score, obtained on the QoL scale.
A plurality of the ratings of the degree to which the pandemic caused changes in mobility, daily activities, and relating to others was “quite a lot”. Eating habits were generally rated as “not at all” affected by the pandemic (Figure 1).
_mobility__b)_how_people_relate_t.jpg)
Concerning the impact of the pandemic on mobility, daily activities, relating to others, and eating habits, the OA identified that the main aspects affected were: physical activity, entertainment/leisure/distraction, needs, education, social relations, home, risks and concerns, and food.
In the discourses, evidence was provided that physical activity was affected: “…it is difficult/I am not allowed/I cannot… going for a walk… exercising outside the home… going to the gym… going to the sports hall… going for a run… walking in the park.” It can be seen that measures aimed at reducing mobility had an impact on the QoL of the OA, reducing their options for moving around and practicing physical activity.
Regarding entertainment/leisure/distraction, the discourses on how QoL were affected included the following: “… boredom…, … I have not been able to… going out to go places… going out to church… going out to some public space… going out freely… going out in the street… doing activities that I like…. attending workshops/craft classes… going out alone… go for a walk/outdoors/park… going to squares/parks/gardens/mass/church/restaurants… sitting on a bench in the park… meeting in my church groups… .” A negative association was observed between the adoption of distancing measures and social activities that had been common before the pandemic and that were no longer carried out because of restricted mobility. Regarding the transformation of activities during the pandemic, the following language was extracted: “…I am… working from home… inside the house… more glued to the television…,” “…it affected a lot… in my mobility… in moving to other places… in being in front of the PC all day… in the way I interact in public spaces… .”
With respect to needs, the following language was noted: “… no… going to the market … being able to enjoy food in restaurants… walking to go to the doctor… going out to the street… going to the free supermarket… selling in markets because of restrictions… shopping activities were suspended… I avoid going out/travelling/moving around… I have to work… I closed my workplace… I only go out for shopping… .” Similarly, the following language “…I am… working from home… inside the house… more glued to the TV… …it affected a lot… in my mobility… in moving to other places… in being in front of the PC all day long… in the way I relate to public spaces…” was recorded in association with the transformation of activities. Hence, two aspects revolve around needs: one relating to the avoidance of some activities to adhere to restrictive measures, and another showing the performance of work activities, despite restrictions, since the economic income and subsistence of the person and his or her family depended on these activities.
Education affects QoL, particularly in terms of the practical ways in which it is conducted, as seen in the following: “… no… I can take my classes… I can take the bus to school…”; education, thus, is considered to have undergone a significant adaptation in terms of the use of new technologies in the wake of the pandemic.
Social relationships are taken to include those with individuals and those with social groups and of all degrees and types, such as acquaintances, friends, and family in all their derivations. For this category, the following were recorded: “… can’t… contact with people… visit family… attend meetings/parties with colleagues…socialise with my age group… greet friends from church… .” This is a negative point since social isolation contributes to the avoidance of socialisation in microsocial spaces.
The home has become the center of social relations during the pandemic. Therefore, QoL has been affected, giving rise to this type of negative discourse: “… I am/feel… locked… irritable… powerless… alone… … I cannot… move freely…” indicating a clear state of deprivation of freedom, together with a condition that goes beyond the simple fact of feeling locked in. As such, the home, far from providing a site of relaxation and healthy coexistence, has created a greater amount of tension and stress. Nevertheless, it is also associated with a positive state, in which the discourses have been as follows: “… I feel that… it has not affected me… I have home activities… I carry out my activities as usual…”; the association is different here because some individuals are not used to having activities outside the home, indicating the perception that their relationships have not been modified.
Risks and worries were inscribed in the following aspect, to which the discourses refer: “… for fear of infecting/contagion to my family … I have to take good care of myself … I limit myself when I go out….” This category is related to protecting oneself and the community.
The final category, food, was discussed in the following terms: “… I have to modify my diet… I eat… more than I should eat… moderately… at home now… more fruits and snacks… more… with modified schedules… strictly… healthier… by anxiety… with more water… less to lose weight… my habits are healthy… I stopped drinking soda… money is not enough… there are foods that have gone up in price… .” Clearly, impactful changes took place in relation to food.
Figure 2 shows the discursive associations expressed by the participants regarding QoL and the impact of the pandemic on their mobility, relating to others, activities of daily living, and eating habits. This image provides the center that conditions each of the moments described above and how these are associated with the periphery, determined by the dynamic process of associations between the core and the periphery, which change in relation to the temporality of the phenomenon.

Discussion
The COVID-19 pandemic substantially impacted the QoL of OA, proportionally to age. This phenomenon may be related to both biological and social vulnerability, which are frequently associated with preexisting health conditions in older populations, as well as with social exclusion, isolation, and neglect; conditions were related to the context imposed by the health crisis, which exacerbated historical inequalities between population groups16 and relate to the risk of severity and mortality by COVID-19 in OA.2 Importantly, preexisting health conditions were found in six out of 10 study participants, risk factors that have been shown to affect the prognosis of COVID-19-infected patients with arterial hypertension, diabetes mellitus, and respiratory diseases.17
The unemployed people had the lowest QoL scores, with statistically significant differences between them and retired people. Economic challenges have been among the negative social consequences of the COVID-19 quarantine and pandemic, especially for unemployed people.18 This context, imposed by the pandemic, complicated the employment landscape for an economically active population that has long been characterised by informality in Mexico.19
A worsening QoL was shown for OA with lower levels of schooling (secondary or less) compared with those with higher levels of schooling (high school or more). Those with lower levels of schooling have a lower QoL.12,13 Recently, it was found that the individuals characterised by low levels of education and lack of employment obtained significantly lower scores in QoL, relative to the other study groups.20 There was a negative correlation between age and QoL, so it is possible to consider age as a predictive variable of QoL of OA in daily practice.
The participants in our study were highly adherent to protective measures against COVID-19. Epifanio et al.20 found a higher rate of adherence to prevention and control measures among OA (63.8%) than among middle-aged adults (63%) or young adults (62.4%). Adherence to basic public health measures can limit the spread of virus transmission in the community,21 and the adherence of OA in particular, to such measures is critical because of their high vulnerability to COVID-19.22 The fact that OA had high adherence to prevention measures may be related to the perceived risk of disease transmission and fear of death. In turn, Gershon et al.23 found that both adherence and intention to adhere to prevention measures at the individual or collective level are associated with the perception of risk and the severity of the situation. In this study, 79.8% of participants reported experiencing a sense of fear of contracting the disease. Uribe Alvarado et al.24 reported that the fear of infection and death from COVID-19 predicts the confinement actions of both men and women without distinction; however, in another study published in the same year, it was reported that age was not a substantial factor in compliance with prevention and control measures for COVID-19.25
The perception of the impact of the pandemic on QoL in the study population, considering mobility as well as the way of relating to others, daily activities, and eating habits, it could be identified that the reduction of mobility and social distancing as a basic public health measure had an adverse impact on the QoL of OA. The discourse analysis of the participants’ responses in relation to this aspect showed that the adoption of mobility restriction measures had an impact on their QoL, reducing their mobility options26; not only was the impossibility of carrying out physical activity linked to health care expressed, but also the restricted ability to perform activities to meet daily needs was mentioned.
A decrease in physical activity levels has a negative impact on energy balance, which can lead to increased body weight, especially when accompanied by an increase in calorie consumption, as the performance of physical activity represents an extra expenditure of energy relative to the requirement for the maintenance of basic vital functions.27 Physical inactivity is the most important risk factor for mortality worldwide and is the main component of lifestyle,28 having been linked to conditions such as overweight, obesity, cardiovascular diseases, diabetes mellitus, and hypertension during the COVID-19 pandemic, all of which are considered risk factors for the disease. Restricted mobility affects physical activity in OA and encourages the adoption of a sedentary lifestyle, limiting their participation in a physical activity program and discouraging physical activity within the home,29 especially in relation to those who lack support for physical activity, given that people who are more physically active are more likely to have support, especially from family.30
Physical activity also contributes to preserving the cognitive, physical, and social functions of OA andaintaining a level of Independence.31 The existence of discourses accounting for the level of both spatial and emotional adaptation to the context imposed by the pandemic was present among the participants, along with the discussion of available resources to meet such needs, especially concerning those who show interest in continuing with their daily routine. The speeches show the level of adaptation to the context imposed by the pandemic, especially among those who show interest in continuing with their daily routine.28
Regarding entertainment/leisure/distraction, a negative association was observed between the adoption of distancing measures and social activities performed before the pandemic and which were no longer performed due to restricted mobility. This directly impacted the QoL of OA as it constituted a constraint for the release of stress, restricting access to recreational spaces, to respect the health regulations imposed.32 Therefore, entertainment that represented a moment of freedom and enjoyment was replaced by the denial of activities and feelings of boredom.33 In this sense, discourses were also associated with the transformation of activities, to which adaptation had not been fully achieved.34 Note that no such recreational activities, were identified but rather those that were an extension of work and, in parallel, a reflection on what the pandemic has left in the QoL in relation to public spaces that were the center of recreation and mobility. In this way, religious activities, recreation, social interaction, etc. were activities that OA valued as part of their usual cultural practices concerning lifestyle, quality time, and enjoyment.
Regarding meeting needs, two aspects can be observed, namely, work activities that could not be abandoned because the family’s livelihood depended on them19 and optional activities that were avoided for their own protection and of the community23 In this way, the pandemic affected health directly, leading to the generation of stress, anxiety, and concerns related to the satisfaction of needs.
The implementation of social isolation and confinement to the home led to the adoption of new practices in the regions of academic study, work, commerce or business, entertainment, health, and others. Teleworking and tele-education were developed as new ways of work and human coexistence35; however, for the OA population, online work was a challenge due to the need to face use technologies to carry out their work.36 The COVID-19 pandemic produced a need to resort to the use of communication technologies to explore new ways of working, living together, and relating to others. OA necessarily found themselves subjected to new forms of social exclusion, as the lack of access to technological resources and skills to manage them exacerbated exclusion in times of social confinement, confirming the existence of a marked gap in the digital era, despite the increased internet use seen in OA, their levels of use remain low compared to other age groups.37 In Mexico, according to data from the National Survey on Availability and Use of Information Technologies in Households, 2019,38 34.7% of people aged 55 and older use the internet, the lowest rate of any age group. Hence, the pandemic affected health directly by generating stress, anxiety, and worry.18
The impact of the pandemic on social relationships was negative, as social isolation contributed to the distancing and deterioration of interpersonal relationships and participation in social activities such as feasts or celebrations39; thus, the impediments to socialisation in microsocial spaces had a negative impact on the individual’s social circle and with whom they share life experiences, impacting on psychological wellbeing.5 It is known that as individuals age, social relationships change, showing a tendency to decrease, especially among people with older age, lower income, and lower education40; however, measures of social distancing could accelerate the reduction of social contacts and participation in activities (as shown by the mean scores obtained by the participants of this study, concerning the dimension of social participation), already diminished in OA, leading to a feeling of social isolation and loneliness.41
Additionally, the home has become the center of life during the pandemic, denoting a deprivation of freedom, as well as a condition that goes beyond the simple fact of feeling locked in, generating a greater amount of tension and stress, which provides a niche of opportunity for the development of strategies to promote healthy coexistence and relaxation within the home.42 However, this was also related, particularly for individuals who were not used to having activities outside the home, to a positive state, with the perception that their relationships had not been affected.41
Risks and concerns had greater relevance to the individual aspect. Although health measures indeed represent the most abundant limitations in this discussion, what has really determined the behavior of our participants is the experience of fear.43 Fear may influence decision making regarding the adoption of protective measures and QoL44; however, so far there is a lack of social programs aimed at improving QoL, except for access to psychological assistance, as part of mental health care.45
Food, as the last of the categories, showed changes in three aspects: dietary, eating habits and economic aspects. Dietary changes were related to the amount of food consumed and the integration of new foods into the diet; such changes have been associated with dietary improvement. .46 Alternatively, it was found that food habits were delimited by the establishment of schedules, inclusion or exclusion of some type of food, and the adoption of a generally more natural diet.47 Finally, economic aspects were related to the increase in food costs, which were found to have a negative impact on health.48 These dietary changes had a direct impact on gut health, which is clearly related to diet. However, it is important to recognise that dietary changes are focused on adopting as natural and healthy a diet as possible.
In relation to diet and gut health, it was found that 28.1% of OA were classified as constipated. The prevalence of constipation in the Mexican population ranges from 2.4% to 22.3%.8 Constipation in OA has a negative impact on QoL due to the presence of preexisting conditions.7,9 and factors related to insufficient fiber intake, lack of physical activity/mobility, stress, anxiety or depression, and increased drug intake.49
Although this study did not inquire about dietary fiber intake, it can be affirmed based on the results, that the OA who participated in this study experienced reduced mobility and consequently low physical activity, increased sedentary lifestyle, and dietary changes.
Conclusions
OA with poorer QoL during the COVID-19 pandemic had older age, lower educational attainment, unemployment, no partner, chronic illness, and self-reported functional constipation. Through the analysis of the perception of OA regarding the impact of the pandemic on their mobility, daily activities, relating to others, and eating habits, it was found that during the pandemic, social isolation, activity limitation, and low physical activity impacted the QoL of OA and possibly on their gastrointestinal health, making it necessary to implement strategies that provide care to this vulnerable group and contribute to their overall wellbeing.
The evident trend of an aging world population and the possibility of facing new pandemics in the near future makes it necessary to implement public actions at the governmental level that contribute to the general welfare of the elderly by reducing social inequalities that promote and preserve their capabilities and autonomy. Digital literacy of older adults can contribute to the overall well-being during pandemic episodes. The implementation of this strategy should take into account their limited access to technology as a population group and that their prior knowledge is minimal, so it is necessary to train and guide them. Greater access to knowledge of information technologies and the use of digital tools could facilitate the implementation of programs that promote mobility at home, through digital tools such as devices and applications, as well as the acquisition of healthy eating habits to contribute to the improvement of the nutritional status of older adults through advertising, digital applications, among others.
Among the limitations of this study was its design, since being a cross-sectional study, it was unknown whether the low quality of life in older adults could be attributed to the effect of the pandemic. Another limitation was the bias in the sample size, since the use of the instrument was limited to being online and remote; due to the need to adopt voluntary social isolation as a measure to prevent the transmission of the disease, especially among older adults, which limited their participation. However, the support of a direct and younger family member was of vital relevance for data collection.
Funding
None.
Authorship contributions
All authors contributed to study design and writing of the manuscript.
Competing interests
The authors completed the Unified Competing Interest form at http://www.icmje.org/disclosure-of-interest/ (available upon request from the corresponding author), and declare no conflicts of interest.
Correspondence to:
Brenda H Camacho Díaz.
Biotecnología, Instituto Politécnico Nacional, Centro de Desarrollo de Productos Bióticos.
[email protected]