Malaria is the leading cause of death in Tanzania, most notably in children under five. It is so ubiquitous that approximately 90% of the Tanzanian population is at risk of developing it.1 The disease has become a significant burden on Tanzania and a major source of poverty and underdevelopment in the country.2 Every year, approximately 14–18 million malaria cases are reported in Tanzania and approximately 120,000 deaths.1 To date, the insecticide-treated bed net (ITN) is one of the essential tools to prevent malaria transmission.3 The ITN is a mosquito net treated with an insecticide that kills mosquitoes that come into contact with it.4 A more recent innovation of the ITN is the long-lasting insecticidal net (LLIN), which has become the most recommended net by the World Health Organization (WHO).4 Unlike other ITNs requiring regular retreatment with insecticide, LLINs are factory-treated and therefore do not require retreatment.4
In Tanzania, tremendous ITN implementation efforts have spanned multiple decades. Notable examples include the recent National Insecticide Treated Nets (NATNETS) program, which operates under the National Malaria Control Program (NMCP),5,6 and the Zanzibar Malaria Elimination Program (ZMEP). These programs have been spearheading LLIN implementation efforts all across Tanzania.7 Nonetheless, operational and behavioural gaps in implementation exist, preventing the sustainable and universal adoption of ITNs.7,8
The priorities of NMCP and ZMEP were to increase the ownership rate of at least 1 LLIN for every two people to 80% by 2020 and 100% by 2022/2023, respectively.7 However, the 2017 Tanzania Malaria Indicator Survey (TMIS) revealed gaps in implementing these programs to the general population. One such gap was that 78% of households in mainland Tanzania owned at least one LLIN, with only 45% of households having one LLIN for every two people.7 Similarly, in Zanzibar, 79% of households were found to own at least one LLIN, but only 42% of households had one LLIN for every two people.7 To meet the strategic goals, the scope and quantity of LLIN distribution must be increased to reach households without any LLINs and provide sufficient LLIN coverage for all.7
As shown by the 2017 TMIS, the NMCP and ZMEP only attained approximately 80% ownership of one LLIN in Tanzanian households. Since both access and use can serve as reasonable proxies of how effective implementation strategies are to ITN implementation programs, the two indicators could explain the remainder of households not owning a net. Comparing LLIN access (i.e., the proportion of the population that could sleep under an LLIN if two people used each LLIN) to LLIN use can help identify behavioural gaps. That is, determining where available LLINs are not being used.7
Therefore, this study aimed to provide a deeper understanding of the existing barriers and facilitators to ITN implementation and help inform and improve future ITN implementation efforts within and beyond Tanzania.
METHODS
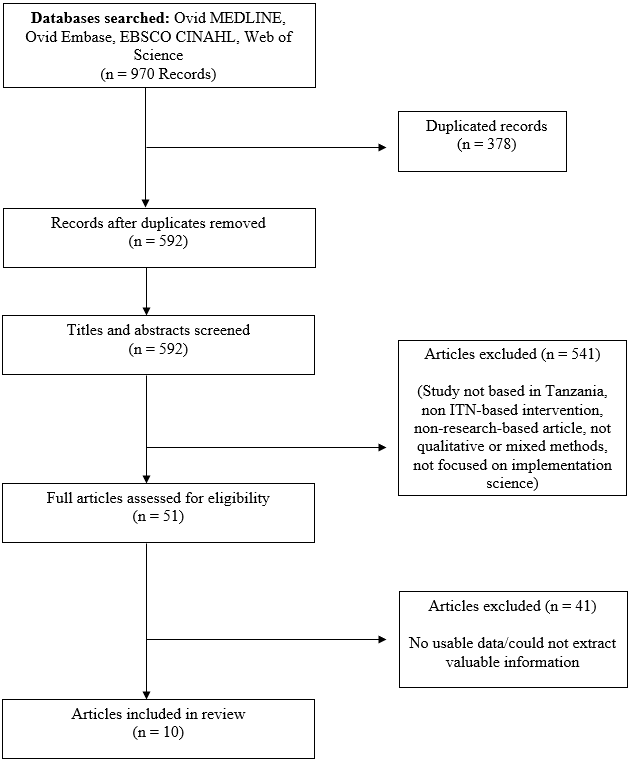
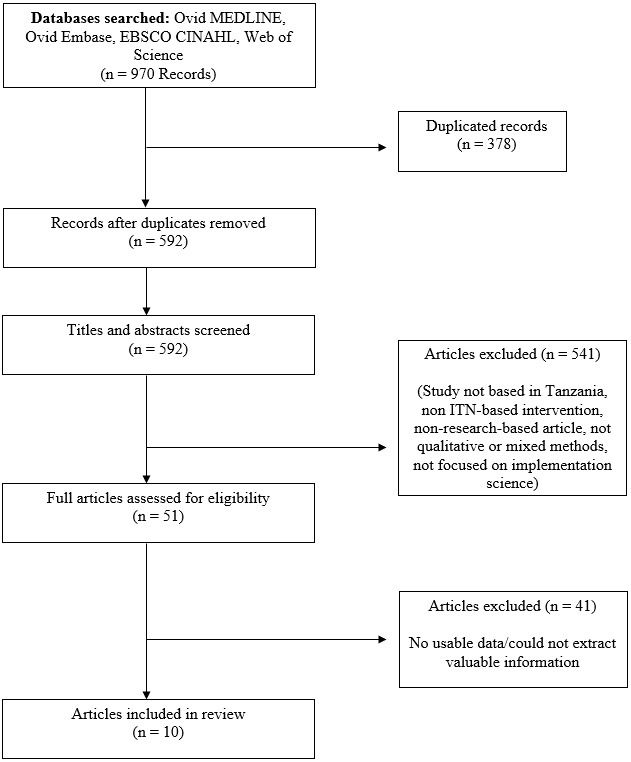
The authors followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines to present the review and analysis.9
Search strategy
A comprehensive search was conducted in OVID Medline, OVID Embase, EBSCO CINAHL, and Web of Science using a search strategy developed by an academic health sciences librarian (KB), with input from the research team. The search was conducted on September 15, 2020, and the results were limited to English-language primary journal articles solely involving human subjects. No publication date limits were applied. The search included articles focused on Tanzania, the Democratic Republic of the Congo, or both countries. However, in the interests of this review, only the results related to Tanzania are reported.
Eligibility criteria and study selection
To be included in the systematic review, studies needed to be English-language research articles published in an academic journal. The research needed to employ qualitative methods or mixed methods with a qualitative component. The article had to address the problem of malaria eradication. The research needed to have been conducted at least partially in Tanzania; if the study was executed in several countries, disaggregated data needed to be available for Tanzania. The study needed to report on an ITN intervention, campaign, or program. The study also needed to discuss the implementation of the intervention and report on at least one barrier or facilitator to implementation.
Study screening was completed using Covidence, a systematic review management tool. Article titles and abstracts were initially screened independently by two authors (YE and AN). Conflicts were resolved by a third party (KB). Next, the full texts of the publications were retrieved and imported into Covidence. Two authors (YE and AN) independently assessed them for eligibility, and conflicts were resolved by a third author (KB).
Forward and backward citation searches were performed for all included articles to find additional studies matching the eligibility criteria that the database search strategies may have missed. Each study included in the review was accessed using Web of Science, and the article’s reference list and the publications that cited it (the “cited by” list) were retrieved. Each article was then assessed to determine whether it met the inclusion criteria. If so, the process was repeated to review the new study’s references and cited by list until no potential studies remained.
Data extraction and analyses
Two authors independently extracted data (YE and AN) according to a standardised form and summarised it in tables. For each study, the following information was recorded: study title, author names, year of publication, study design and methods, study participants, study objective, facilitators of implementation, and barriers to implementation. If there were disagreements in data extraction, they were resolved through discussion facilitated by a third author (OE).
Following data extraction, two authors (YE and AN) coded the barriers and facilitators according to the Consolidated Framework for Implementation Research (CFIR). This conceptual framework comprises five broad domains and 39 constructs that guide the systematic assessment of factors that influence the implementation of interventions.10 The CFIR was used in this review to facilitate a thematic analysis of the data and increase the generalizability of study findings. To apply the CFIR, the barriers and facilitators identified during data extraction were independently coded by the two authors using the 39 constructs in the framework, and a third author (OE) resolved any conflicts in coding.
After coding, two authors (OE and YE) revisited the barriers and facilitators to identify and fix any inaccuracies in the data and to ensure the data extraction form instructions were adhered to and, in particular, that extracted data focused on the outcome of interest (barriers and facilitators). During multiple meetings, any extracted data that did not explicitly focus on ITN implementation were removed, such as data focusing on ITN usage instead of ownership. Selected articles were reviewed a second time to ensure that extracted data accurately reflected each article, provide further context on extracted barriers and facilitators if needed, and assess whether any barriers or facilitators were missed during the initial review and could be extracted. The two authors also revisited the assigned codes to ensure that construct definitions provided by the CFIR accurately matched their respective coded barriers or facilitators. The code was replaced if both authors deemed a different code’s definition to be more appropriate for a selected barrier or facilitator than its precursor.
Quality assessment
Selected studies were assessed for methodological quality using one of two critical appraisal tools. Qualitative studies were evaluated using the Critical Appraisal Skills Program (CASP) Qualitative Research Checklist.11 The tool comprises ten questions: two screening questions and eight that assess the study results’ validity. All questions can be answered by recording “yes,” “no,” or “can’t tell.” The researchers decided a priori that studies that did not receive a “yes” response to both screening questions would be excluded from the review.
Mixed-methods studies were evaluated using the Evaluation Tool for Mixed Methods Studies,12 a tool comprised of key questions to assist in the critical appraisal of studies that use more than one method. Questions focus on the study’s setting, sample, ethics, outcome measurements, group comparability, qualitative data collection and analysis, and policy and practice implications. Questions are answered using free text comments rather than fixed responses. The use of unique tools for critical appraisal acknowledges the unique natures and epistemologies of different research designs.13 This approach was chosen over a tool that could be used with any design, as general tools have been criticised as being too generic to engage with specific quality issues for each research design, especially mixed methods studies.12,13
RESULTS
Study characteristics
The detailed study characteristics of the ten included studies, including the year of publication, study objective, study participants, study quality appraisal, study location, and focus on ITN or LLIN, are presented in the following paragraphs. The study characteristics are summarised in Table 1.
Year of publication
All the included studies were published after 1995. Of these studies, two were published between 1995 and 2000, four were published between 2000 and 2010, and the remaining four were published between 2011 and 2020.
Study objectives
The studies examined the implementation of ITNs in a variety of ways. Two studies assessed the perceptions and practices surrounding malaria and ITN usage among village members in Tanzania. Similarly, one study evaluated existing challenges to the sustainable implementation of ITNs for village members in the Bagamoyo district of the Pwani region. One study assessed an intervention that sought to achieve sustainable net coverage levels by combining the free distribution of LLINs with community-tailored education in a Tanzanian village. One study evaluated the social and cultural factors that influenced ITN project implementation. The evaluation of the study included collecting evidence from village members through participant interviews, neighbourhood meetings, and informal and focus group discussions. One study sought to understand and compare the outcomes of a voucher scheme in Tanzania and another country (Ghana).
In contrast, two other studies sought to understand the community use of ITNs to control malaria in Tanzania. This review observed a study that evaluated the use of social marketing in the Kilombero and Ulanga districts of Tanzania to stimulate market development for ITNs. Finally, one study explored the reasons for scepticism and low uptake of ITNs promoted through a social marketing strategy for malaria control before the introduction of LLINs.
Participants
The study participants ranged from village members to members of larger entities involved in implementing ITNs. Of the ten studies, three included village members, and another three included Tanzanian residents from selected regions and associated districts as their participants. In addition, two studies observed caretakers of children under five as their study populations.
Community leaders (e.g., village and household heads), who possess a considerable influence over decisions and collective attitudes, were investigated in two studies. Three studies focused on health workers as their study cohorts, including child health clinic staff, pharmacists, and health facility staff. Members of both the private and public sector were involved as participants in one study, including manufacturers, wholesalers, importers and distributors of ITNs, members of the NMCP in Tanzania, members of regional and district health management teams, voucher scheme management agents, and staff members of the non-governmental organisation (NGO) coordinating voucher schemes. Finally, two studies included retail agents as study participants.
Quality appraisal
In total, ten studies met the inclusion criteria. These studies were qualitative (n=3) or employed mixed-method design (n=7). When the qualitative studies were appraised using the CASP checklist, the authors responded “yes” to all the checklist questions for one study, while the other two studies elicited a “no” for item 6, indicating a potential source of bias. One of the two studies elicited a “no” or “Can’t tell” for items 3, 4, 7, and 10. Of the seven mixed-methods studies appraised using the evaluative tool for mixed-methods study design, the authors responded “yes” to all the checklist questions for two articles, while five did not. The five articles which elicited a “no” were found to be lacking in one review area: ethics. None explicitly stated that they had received ethical committee approval or informed consent. Of those five articles, one also did not meet the researcher’s potential bias criteria, as the researcher’s position, assumptions, and possible biases were not outlined.
Study location
The studies included in this review took place in one or more of the 31 regions of Tanzania and their 169 subdivided districts. There were seven regions and ten districts featured in the included studies. The regions were Unguja North, Pwani, Kagera, Dar es Salaam, Morogoro, Mwanza, and Tanga. The districts were Kaskazini A, Bagamoyo, Karagwe, Kigamboni, Temeke, Kinondoni, Kilombero, Ulanga, Sengerema, and Muheza. The studies were predominantly conducted in the Morogoro region (n=3) and its respective districts, Kilombero (n=3) and Ulanga (n=3). The remaining regions and their respective districts were each covered in one study. One study was set across all of Tanzania—in all 31 regions and subdivided districts.
ITN or LLIN
Among the studies included in this review, six focused exclusively on ITNs, while two focused on LLINs. The remaining two studies examined both ITNs and LLINs.
Barriers
Of the ten included studies, two cited misconceptions about ITN usage as a barrier to implementation. One of these mentioned villagers’ concerns about the insecticide toxicity of government-provided nets as a widespread misconception. Many villagers believed that the insecticide affected fertility, including the capacity to “reduce men’s ability in sexual activity.”14 The other study highlighted how villagers perceived the need for bed nets as an additional misconception, as “some villagers said that they had been living without nets their whole lives and could not see why they should suddenly be necessary”15 posing a risk to implementation in Tanzania.
The poorly developed formal private sector in Tanzania, which resulted in limited resources allocated toward implementing bed nets, was cited as a barrier by one study.16 This study mentioned that in the poorly developed private sector, net distributors had access to “limited resources and therefore limited capacity to buy ITNs in bulk”16 and that a lower uptake rate by Tanzanians was observed. Conversely, the affordability of ITNs was viewed as an ambivalent factor, considered either a facilitator or a barrier to implementation in five studies. Of these five studies, four mentioned the cost of nets as a disadvantage to ownership, as nets were deemed unaffordable and too expensive for most Tanzanians,17–20 especially for individuals living under poor social and economic conditions.18
One study cited the method of single-day net distribution in one central location as an unsuccessful strategy for implementation compared to the high-frequency (multi-day multi-location) distribution method. Reasons for this lack of success included villagers being occupied on the day of distribution and the dispersed nature of some houses in villages, which made it difficult for committee members to reach them.15 Also, selling nets in advance as a form of distribution was cited as a barrier to implementation. Villagers doubted whether they would receive their nets after purchase, and committee members responsible for distribution occasionally forgot which villagers had purchased nets.15
Facilitators
In the context of malaria and ITNs, social marketing is defined as a strategy to develop activities that focus on promoting net ownership and usage, raising awareness of its health benefits, and creating healthy behaviour changes. This strategy was found to be successful in Tanzania by two studies. Various benefits emanating from the use of social marketing were cited, including the resultant development of “strengthened trust and understanding between the public sector and the private manufacturers,”16 as well as substantial increases in the number of outlets selling nets.21 One such study mentioned how “social marketing led to an outward shift in demand,”21 resulting in a greater increase in coverage and net availability in the targeted area.21
Projects focusing on communication were also proven to be successful in Tanzania by two studies. One study found that communication campaigns in the form of education sessions successfully implemented ITNs.22 These sessions, which focused on communicating the importance of net procurement to prevent malaria transmission, significantly improved villagers’ attitudes and consideration of net procurement and even modified their behaviours toward the nets.22 The second study, as mentioned above, cited continuous, direct communication between stakeholders (e.g., villagers, retail agents, and village resource people) as a successful implementation strategy.18
One of the studies cited the early promotion of ITNs as an implementation facilitator. That study noted that when promotion was initiated several months before the distribution of nets, this intensification of communication resulted in a higher initial coverage rate, thus enhancing net implementation.15
Village representatives were identified as an essential asset to ITN implementation. One study cited actively involving village government representatives in promoting net sales as a facilitator, leading to higher coverage rates in targeted villages.15
Of the ten studies, two cited voucher schemes as a facilitator of ITN implementation.16,23 Reasons given included the monetary discount that the voucher schemes provided, which was viewed as a positive incentive by local villagers,23 as well as their advantage in targeting specific at-risk populations on a larger scale, as nets could still be “distributed and sold through ordinary retailers”23 as opposed to health services.
One study found that the high-frequency distribution of nets (i.e., multi-day distribution) in multiple village locations in Tanzania was a successful strategy to increase ITN coverage rates. This same study also cited direct net transactions, in which nets were purchased and received immediately by buyers, as a facilitator of net implementation, as both strategies resulted in higher ITN coverage rates in their respective regions.
The availability of different sized nets was found by one study to increase coverage rates; customers were more satisfied with their purchases, highlighting the importance of variable net size options to uptake in Tanzania.15 In addition, although ITN affordability was cited as a barrier to implementation (see Barriers above), another study cited bed nets as an affordable option. Compared to the more expensive alternative protection measures on the market in Tanzania (e.g., mosquito repellents), the relative affordability of ITNs contributed to their increased uptake due to their economic advantage.15
CFIR results
The CFIR was used to help conceptualise the identified barriers and facilitators in a more organised manner. The CFIR is a guide composed of five broad domains and 39 constructs, each associated with effective implementation. Each facilitator and barrier was coded according to the CFIR with one of the 39 available constructs. A total of nine CFIR constructs were used in this review. Under the Intervention Characteristics domain, Cost was the only construct used. As Cost is defined as any costs associated with the implementation of the intervention, both “affordability of nets” and “financial constraints” were coded under this construct. Similarly, External Policies and Incentives was the only construct used to code any barriers and facilitators under the Outer Setting domain. This included the facilitator labeled “ITN Voucher Schemes,” which dealt with certificates of funding to alleviate ITN costs. Available Resources was the only construct used under the Inner Setting domain to code the extracted facilitator “availability of different sized nets” and the barrier “poorly developed private sector.” Under the Characteristics of Individuals domain, Knowledge and Beliefs about the Intervention was the only construct used. As the CFIR defines Knowledge and Beliefs about the Intervention as the attitudes toward and familiarity with the intervention that individuals possess, both barriers, “concerns with government-provided nets” and “perceived need of bed net” were coded using this construct. The remaining constructs used, including Planning, External Change Agents, Opinion Leaders, and Executing, fell under the Process domain.
DISCUSSION
The NMCP and the ZMEP lead LLIN implementation efforts in mainland Tanzania and Zanzibar have seen tremendous successes throughout the years. This was especially apparent in terms of their previously established distribution programs, such as the Tanzania National Voucher Scheme (TNVS) and the Under-Five Catch-Up Campaign (U5CC), which have helped put nets into the hands of numerous Tanzanians. Despite this achievement, major gaps in these programs still exist that impede the successful and sustained implementation of ITNs in Tanzania.9,10 By examining ten studies, this systematic review has identified multiple barriers and facilitators to implementing ITNs in Tanzania. Of the identified barriers and facilitators, factors affecting cost, knowledge and beliefs, and planning for execution were considered critical targets for future implementation efforts.
This review has determined that cost is an essential factor influencing the implementation of ITNs. Typically, mass distribution campaigns led by the government of Tanzania are the primary source of ITN procurement for Tanzanians.24 However, Tanzanians also have the choice to purchase ITNs, which are sold through private retailers at a cost of 3,000–5,000 Tanzanian shillings.17,20 Through our analyses, it was found that cost was considered both a facilitator and a barrier to implementation. Five studies cited cost as a barrier, mainly due to people not being able to financially afford ITNs. Although cost was cited as a facilitator in one study, this was only relative to the other malaria-control options available to Tanzanians, which were more expensive than nets. Outside of this context, the reality is that ITNs are still too costly for most Tanzanians, who often cannot afford to pay the price required to acquire a net for themselves or their entire family. This situation is made worse by people’s preferences to purchase nets from retailers instead of receiving them free of charge or at a discounted cost from the government (due to distrust of the government), further calling attention to the role cost plays in implementation.
Therefore, as mentioned in the results of this review, a voucher scheme can become a crucial element of an ITN implementation program in Tanzania. Because voucher schemes essentially provide individuals with a voucher that they can use at a public or private provider to purchase an ITN at a discounted price, they can help alleviate burdens caused by financial incapability. In fact, voucher schemes were found to successfully make “acquiring an LLIN widely affordable,”16 resolving complications concerning the cost of nets. Although this review identified cost as a critical factor affecting the implementation of ITNs in Tanzania, voucher schemes can increase ITN ownership by catering to locals’ preferences while decreasing the financial burden associated with acquiring nets.
Various beliefs and attitudes toward ITNs exist in Tanzania, related to ITNs ownership.14 Yet, none were identified in our review as having an influence on implementation except two notable beliefs, which were crucial in determining the success, or lack thereof, of ITN implementation in Tanzania. The first of these beliefs was the potential consequences of using a government-provided bed net. Due to their lack of trust in the government, villagers believed that nets provided by their local government office contained insecticides that could “reduce men’s ability in sexual activity.”14 Regardless of these nets being provided free of charge, villagers refused them. The second belief was the perceived need, or lack thereof, for ITNs. As highlighted in the Results section, some villagers noted that they had lived without nets their entire lives without having caught malaria and did not deem it necessary to acquire one. As villagers refused the procurement of nets for these reasons, both of these beliefs contributed to low rates of coverage in Tanzania. In this case, we suggest that implementation practitioners conduct education sessions on ITNs and malaria transmission in tandem with the distribution of ITNs. These measures would help reduce (and possibly eliminate) negative perceptions of ITNs circulating within the population and instead help inform residents of the benefits of nets and advocate for their use. Understanding local beliefs and addressing them throughout the first stages of implementation can be a useful strategy to increase coverage and ensure sustained ITN use in Tanzania.
Adequate planning before net distribution could lead to a more successful implementation of ITNs in Tanzania. This would include selecting the proper strategies for promoting and distributing ITNs, which remain essential steps in any implementation strategy. This review identified the social marketing of ITNs as a facilitator of implementation. This is because this form of marketing promotes the use of ITNs and raises awareness of the need to decrease malaria transmission; therefore, it addresses the public’s current health behaviours while providing them with a solution. However, it appears that social marketing alone is not sufficient. The timing of such events is also critical. In this sense, the promotion of ITNs several months before their distribution also substantially increases coverage rates by giving communities more time to become accustomed to using nets.
In addition, local village government representatives must be part of the implementation strategies, as they are the ones who ultimately lead and promote distribution efforts. These local leaders have a better understanding of local needs and beliefs and greatly influence the target populations’ decisions and behaviors regarding ITN procurement and usage. Therefore, they can provide support and backing to overcome any problems during the promotion and/or distribution process. Practitioners must consequently consider the earlier promotion of ITNs through the use of social marketing and work with local community leaders to ensure successful implementation.
The method of distribution is also vital for successful implementation. A noteworthy distribution method identified in this review is direct net transactions, in which ITNs are sold the same day they are distributed. Tanzanians are more comfortable with this distribution method, as they are always guaranteed a net immediately after purchase, which strengthens their trust in the implementation project and the product itself. We found that the frequency and location of distribution also matter. Tanzanians are away from towns during many days of the week due to work or other activities, such as fishing or farming.15 As a result, they may not be present on a distribution day and will therefore be unable to acquire a net. Distribution of ITNs occurring on multiple days during the week in multiple, widely separated areas is the best possible solution to this challenge; it would accommodate Tanzanians’ schedules without forcing them to adjust or miss opportunities to purchase nets. In fact, Tanzania locals have expressed dissatisfaction with other distribution methods that have been used previously, such as advanced net sales and single-day distribution.15 The planning of strategies to be used during implementation is necessary to ensure the highest coverage possible, especially in the context of Tanzania.
Limitations
This systematic review has several limitations. While a comprehensive search strategy was executed in academic journal databases and supplemented through citation searching, experts were not consulted to solicit additional articles for potential inclusion. Another potential limitation is using a determinant framework, the CFIR, to code the barriers and facilitators to implementation. Such frameworks have been criticised for their inadequacy in describing causal mechanisms or how change takes place.25 However, the authors chose to use the CFIR to situate the findings of this research within the context of the existing implementation science literature. The use of separate assessment tools for quality appraisal prevented an integrated assessment of the evidence and the overall quality of the included studies. However, employing separate appraisal tools based on the studies’ research designs improved the rigour of the quality assessment.26 The variety of studies included in this study is also a potential limitation, as it increases the risk of presenting varied results, making it difficult to make precise conclusions. However, the integration of various studies is required if the results should be used to inform stakeholders on the many facets of malaria ITN implementation in Tanzania.27
CONCLUSIONS
The findings of this review suggest that future implementation practitioners must attend to certain key factors to ensure the successful implementation of ITNs in Tanzania, including (i) the cost of ITNs, (ii) knowledge and beliefs about ITNs among potential users, and (iii) planning for execution of ITN distribution programs. Thus, additional strategies beyond ITN distribution are warranted to increase net ownership and decrease the malaria burden in Tanzania. ITN implementation can be improved if national stakeholders invest further in processes that promote ITN procurement, such as voucher schemes, providing additional education sessions, integrating distribution methods that cater to locals’ preferences, and initiating the promotion of ITNs months in advance of their distribution.
Acknowledgments
The authors are grateful to Vithusha Kumarathasan for comments on earlier drafts of the manuscript.
Funding
No funding was received for this research project.
Authorship contributions
Study conception and design: OE and KB. Analysis and interpretation of data: OE, YE and AN. Draft of the manuscript: YE and OE. Critical revision of the manuscript for important intellectual content: OE, YE and KB. All authors read and approved the final manuscript.
Competing interests
The authors completed the Unified Competing Interest form at http://www.icmje.org/disclosure-of-interest/ (available upon request from the corresponding author) and declare no conflicts of interest.
Correspondence to:
Obidimma Ezezika, PhD, MEM
Faculty of Health Sciences, University of Western Ontario, 1151 Richmond Street London, Ontario, Canada, N6A 3K7
Email: [email protected]