Immunisation is one of the most reliable and cost-effective public health interventions to reduce the incidence and associated mortality of numerous infectious diseases.1 During the coronavirus disease 2019 (COVID-19) pandemic, it was again globally adopted as an effective public health strategy to curb the pandemic. In India, the National Expert Group on Vaccine Administration for COVID-19 (NEGVAC) was formed to guide all aspects of COVID-19 vaccine administration.2 In accordance with the committee guidelines, in January 2021, the Government of India rolled out the world’s largest vaccination drive by inoculating priority groups against COVID-19.3 The first vaccination phase covered thirty million healthcare workers (HCWs) and frontline workers. The second phase began by covering the entire population over 60 years and those aged 45 years and above with specified co-morbid conditions. In the next phase, everyone above 45 years of age was covered, and after an onslaught of the massive “second wave”, the vaccination drive was expanded from 1st May 2021 to cover everyone above 18 years of age.4
The first phase of the vaccination was critical for India as HCWs are positioned to play a pivotal role in fighting5 the COVID-19 pandemic by playing a critical role at every stage, including planning, target group identification, community engagement, mobilisation, service delivery, tracking, and follow-up.6 Being the navigators and connectors of their communities with the health systems, their confidence in the benefits of the vaccination process is vital to ensure a positive impact on the uptake of vaccination in the community.7 The HCWs vaccinated are more likely to recommend vaccination to others.8 Vaccine scepticism9,10 may negatively impact vaccine uptake among communities, and data suggest that vaccination rates among HCWs correlate positively with their willingness to recommend COVID-19 vaccination to their patients.11
Only 32,94,612 HCWs were fully vaccinated against COVID-19 until 5th March 2021 in India, as per the Ministry of Health and Family Welfare, Government of India.12 Vaccine hesitancy could be one of the contributing factors to the low vaccine coverage. Before introducing the COVID-19 vaccine in India, research conducted with health workers found that they were apprehensive about the vaccine’s safety, efficacy, and possible side effects, along with insufficient knowledge about vaccine development and misinformation on social media.13 However, data regarding COVID-19 vaccination acceptance among HCWs in India is scarce. With this background, the study was conceptualised in March 2021 to assess: a) knowledge, attitudes, and perceptions towards the COVID-19 vaccine or/and vaccination process; b) uptake of the COVID-19 vaccine among HCWs to assess the acceptability of COVID-19 vaccine. The study was conducted with HCWs of the Pune district in Maharashtra. Maharashtra was included in the present study as it is the second-most populous state in India (124.7 million).14 In context to COVID, it was one of the most severely impacted states during both the “first” and “second” wave15 and also reported high hesitancy in the initial phase (Jan-June 2020) of the vaccination drive.16 Within Maharashtra, Pune is the second-most-populous district in the state17 and one of the worst hit during the COVID-19 pandemic.18 In Maharashtra, as of 31st March 2021, in rural areas, there are 12,272 female and 8102 male health workers/auxillary nurse midwifery (ANM) working at sub-centre and 2214 female at PHCs and for PHCs in urban areas 3086 female health workers.19
METHODS
Sampling and participants
Purposive sampling was used to select two blocks, Velhe and Haveli, out of the 15 blocks in the Pune district of Maharashtra. These blocks were selected due to their proximity to the local research team’s office and high population index. Velhe is a rural block comprising 118 villages with a population of 54,516. Haveli has a mixed (rural and urban) population of 24,35,581, comprising 125 villages. In total, 82 villages {Haveli (n=38) and Velhe (n=44)} were purposely selected for this study. To be eligible for the study, the villages should reside within a radius of 65 kilometres from the local research team’s office. Subsequently, HCWs were selected using snowball sampling, wherein the supervisors or heads from the primary health center (PHC), sub-centres, and Sarpanch offices (office of an elected village-level head by the local self-government in India) were approached to further connect with them. The HCWs directly involved with the community health center (CHC), PHC, or sub-centre were included in our study. As per NEGVAC for COVID-19, the HCWs are defined as healthcare service providers and other workers in healthcare settings. These are categorised as frontline and integrated child development services (ICDS) workers, nurses and supervisors, medical officers, paramedical staff, support staff, students, scientist, research staff and other health staff.20
Data collection
A self-administered, online questionnaire was completed with the HCWs to assess their knowledge, attitudes, and perceptions regarding the COVID-19 vaccine and its uptake. Considering the COVID-19 pandemic, a ‘Google Form’ of the questionnaire was shared with the participants to avoid paper contact between the research team and participants. The data was collected from June-August 2021. The questionnaire included a section on the socio-demographic profile to document participants’ age, gender, education, designation and involvement at the health system level.
Knowledge was assessed using nine questions related to the COVID-19 vaccine (e.g., Do you know if the COVID-19 vaccine is effective in preventing COVID-19?). Attitudes towards the safety and immunity developed after the COVID-19 vaccination was measured using seven questions. The perceptions towards COVID-19 vaccination were assessed through seven questions focusing on the approach of vaccination, side effects and implications on everyday life, vaccine hesitancy and its reasons. The vaccine uptake among HCWs was assessed using two questions (Have you taken the COVID-19 vaccination? If not, what hesitations do you have about getting the COVID-19 vaccine?).
The research team developed the questionnaire after a thorough literature review (national and international), adapting questions from the validated tools21–24 and the Government of India’s guidelines for implementing the National COVID-19 vaccination program.20 The questionnaire was first developed in English and then translated into Marathi, understanding the contextual background of the participants. The questionnaire was also back-translated from Marathi to English to ensure translation accuracy, and the translated items retained the same meaning as the original. Before commencing the data collection for the main study, the questionnaire was pre-tested with HCWs (n=10) to ensure its face validity. The selected HCWs were not part of the main study. Feedback received during the pre-testing was incorporated into the questionnaire before finalising for the main study.
Statistical analysis
Statistical analysis was done with the help of Statistical Package for Social Science (SPSS) Version 22. Simple descriptive statistics expressed as means, standard deviations (SD), and percentages were used to understand participants’ demographic profiles and responses.
Ethics considerations
The study was reviewed by the Institutional Ethics Committee of Public Health Foundation of India (TRC-IEC 466/21) and Janaseva Ethics Committee (Ref no:404A/06/2021) and exempted from human subject’s research oversight. The written informed consent was taken from all the participants. The consent stated the permission for data collection, data to be used in scientific publications, dissemination of study findings by maintaining the confidentiality of the study participants and anonymity of the collected data.
RESULTS
In total, 357 HCWs participated in both the study blocks (Haveli=183, Velhe=174), out of which 85.3% were women. The response rate among HCWs was 98.9%, and the reasons for non-participation included refusal due to other work-related commitments. The mean age of the participants was 39.4±9.8 years. Concerning their work, the majority of the participants worked at the community level (78.7%), followed by PHC (14.6%) and sub-centres (6.7%). As per the NEGVAC classification, the majority (81.2%) of participants comprised Frontline Health Workers and ICDS workers, followed by nurses and supervisors (5%), medical officers (3.6%), paramedical staff (2.3%), support staff (0.6%), students (0.3%) and others (7%).
Knowledge of healthcare workers toward COVID-19 vaccination
Overall, the participants’ knowledge regarding COVID-19 vaccination was high (90%). The highest knowledge was for the availability of the COVID-19 vaccine in the community (99.9%) and the importance of practising COVID-appropriate behaviour after being vaccinated (99.7%). Besides high knowledge, a few gaps were also identified, 27.7% of HCWs believed that the COVID-19 vaccine could increase the risk of allergic reactions, and 34.2% were unaware of the vaccination registration process (prior/on-spot) (Table 1).
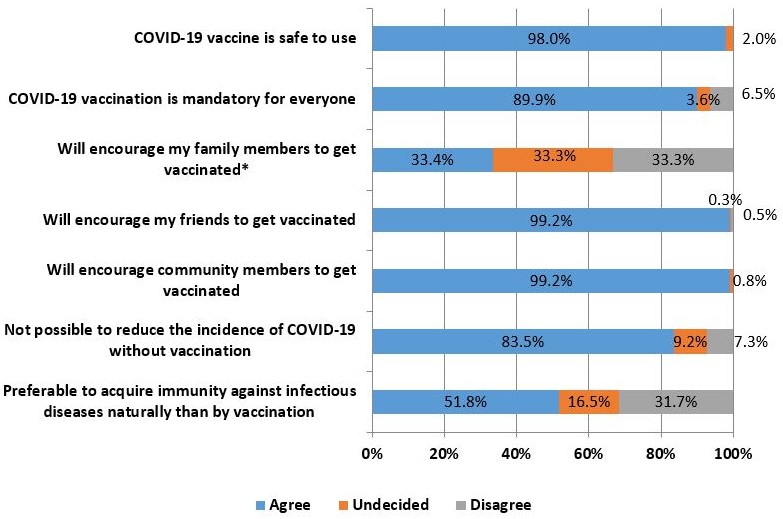
Attitudes of healthcare workers toward the COVID-19 vaccine
Most participants (98%) believed the COVID-19 vaccine is ‘safe to use.’ Most of them said that they would encourage their family members (33.4%), friends (99.2%), and community members (99.2%) to get vaccinated. Besides these, there were a few alarming concerns, such as a little over half (51.8%) of participants believed that acquiring immunity naturally (by contracting the infection) is better than receiving the vaccine. Another noticeable figure was that 16.5% believed it is possible to reduce the incidence of COVID-19 without vaccination (Figure 1).

Perceptions of healthcare workers towards COVID-19 vaccine
A majority of participants (95%) believed that everyone should be vaccinated to control the pandemic, and 87.1% believed that the phased manner of vaccination process is the right approach used by the government for rolling out the COVID-19 vaccination drive in India. As many as 65.0% of the participants believed that people have become careless after the vaccine’s introduction by showing a casual attitude towards COVID-19-appropriate behaviours.
Many gaps were identified regarding participants’ perceptions about COVID-19 vaccination. It was seen that 36.1% of them believed that practising COVID-19-appropriate behaviours (wearing a mask, social distancing), are safer options over receiving a vaccine. An even larger gap was observed in the perceptions regarding side effects of the vaccine, wherein 28.8% thought that the COVID-19 vaccine might have side effects, and 21.3% could not comment on it. 14.0% of participants believed vaccine is not the most likely way to control a pandemic, and 29.4% were unsure about the same (Table 2).
Regarding COVID-19 vaccine hesitancy, 55.2% did not perceive vaccine hesitancy among other HCWs in India. When asked about their perceptions on hesitancy in the community, almost half (47.4%) of the participants perceived that people in India are hesitant to get the COVID-19 vaccine (Table 2). The most commonly reported reasons for vaccine hesitancy in the community were: unknown side effects of the vaccine, safety concerns of the COVID-19 vaccine, and unknown vaccine effectiveness.
Vaccine uptake by healthcare workers
The study findings reported that 93.0% of participants were vaccinated with two doses of COVID-19 vaccine, and 4% received only one vaccine dose. Only 3% (n=11) HCWs were not vaccinated, out of which eight (8) planned to get vaccinated shortly. Among the remaining three; the reported reasons for vaccine hesitancy were: ‘being worried about the effectiveness of the COVID-19 vaccine’ (n=1) and ‘unknown side effects of vaccine’ (n=2).
DISCUSSION
To the best of our knowledge, this is the first study in India that comprehensively assesses the knowledge, attitudes, perceptions, and COVID-19 vaccine uptake among HCWs engaged at various levels of health facilities, including CHC, PHC and sub-centres. Most of the studies to date focused on health workers from hospital settings or vaccine hesitancy.25,26 We engage with HCWs due to their vital role in introducing the vaccine in the community and their association with community members. Research evidence shows that community health workers play a significant role in vaccine promotion and acceptance through community dialogue and engagement, education, trust-building, myth-busting, or community entry.27 The impact of HCWs on health security and pandemic preparedness has been seen in Africa during the 2014 Ebola epidemic28 and the Zika virus epidemic in 2015,29 wherein HCWs contributed significantly by increasing access to health services and awareness. In Sierra Leone, due to prompt reporting of suspected cases by HCWs of Ebola, further spread of the virus could be prevented.28 Evidence globally emphasised the vital role health workers in the success of immunisation.30 In India, a study showed a significant increase (14-22%) in the coverage of specific vaccines and full immunisation in a few states, along with a 16% reduction in the incidence of ‘infants with no immunisation’ due to the Accredited Social Health Activist (ASHA) worker program.31 Eradication of polio in India is another health worker success story; thus, some researchers even suggested a replay of the polio vaccination drive to increase COVID-19 vaccination.32 Hence, it is critical to address the gaps in understanding of HCWs, as they are the first point of contact for any health-related concerns.
Our study assessed the knowledge, attitudes, and perceptions of HCWs regarding the COVID-19 vaccine. Our study findings revealed that a majority of HCWs had a good level of knowledge, in agreement with studies conducted in Ethiopia, China, and India.33–35 Our study findings revealed an overall positive attitude towards COVID-19 vaccination. Despite good knowledge and attitude levels among HCWs, a few gaps were also identified through our study. The identified knowledge gaps were about the vaccination registration process. Some even believed that ‘COVID-19 vaccination increases allergic reaction’ and ‘it is better to build immunity naturally over vaccination’. They were also unsure about the vaccine’s benefits in leading us out of the pandemic or returning life to normal, along with the usual worry of ‘unknown side effects of the vaccine’. Though these are few concerns that have been replicated worldwide but considerable research conducted internationally suggests that vaccination may reduce the spread of infection by either decreasing the viral load or by making the infected person less infectious.36 Researchers in Israel37 and United States38 saw a decrease in COVID-19 viral load in their vaccinated population. Our study also highlighted that HCWs perceived that people had become careless in practising COVID-19 appropriate behaviour after the vaccine’s introduction. A study conducted in Chile also reported similar results.39 Hence, supporting the momentum of the COVID-19 vaccination drive, it calls for the prompt addressing of these gaps in the minds of HCWs about the vaccination, as they are the ambassadors for vaccine acceptance in the community,40 and any doubt in their minds would hamper the progress of vaccination process. Thus, it is important to have a structured program for HCWs in India that includes one-on-one interaction and constant engagement with them. These interactions should seek to resolve any conflicts in their minds by providing them with expert training and continued follow-up sessions. An open ‘two-way’ channel for constant communication with HCWs needs to be maintained at all times. Evidence suggests that the training programs for health workers positively influence an intervention’s effectiveness.41 The mobile technology is rapidly gaining popularity in India across all socio-economic strata, including rural and urban areas. Considering this as an opportunity, a mobile-based App for the HCWs who are involved in the vaccination process, similar to mSakhi App can be introduced.42 The intent of the app will be to break the myths existing around the COVID-19 vaccine and to provide accurate and up-to-date information.
Despite these gaps, vaccine uptake is fairly high among HCWs (93% vaccinated with two doses and 4% with one dose) in our study. This stands in sync with other studies in Germany43 and India.44 Although the above study in India was conducted on medical students across 22 states and union territories, including Maharashtra from Jan-Feb 2021 (6 months before our study and before the delta wave) yet similar to our study, it also looked at a lower rate (10.6%) of vaccine hesitancy in them, confirming our findings. India also achieved a 100-crore COVID-19 vaccination landmark and this has won appreciation globally and from the World Health Organization.45 However, it is also in contrast to other international studies that have reported lower rates of COVID-19 vaccine acceptance, especially in the USA (36%).11,46 In our study, the main reported reason for vaccine hesitancy was “unknown side effects of a vaccine”, similar to many other countries.47
As our study was conducted in June-Aug 2021, the high acceptance rate could be due to the high priority status given to HCWs for vaccination and multiple efforts put forth by the Indian Government to figure out how to maximise vaccine coverage. Under NEVAC, a ‘Vaccine steering committee’ and ‘Task force’ have been formulated at state, district, and block levels and virtual training sessions were organised at every level to brief up the workforce on the latest COVID-19 vaccination updates.48 Additionally, mass awareness campaigns were also run by the Government of India and state governments,49 including TV advertisements, caller tune messages on all phone calls,50 mega awareness drives, IEC material display on COVID-19 vaccine.49 These task forces and efforts were vital in a prompt and smooth vaccination process and attributed to high COVID-19 vaccination acceptance. In addition to governmental efforts, the ordeal of the devastating delta wave in India (especially in the study region) may have played a role in improving vaccine acceptance.
We recognise the limitations of our study. Only two blocks of Pune were included. A wider representation and assessing the sample validity against Census data 2011 could have improved the generalizability of the study findings. The responses to the questionnaire may have been affected by social desirability bias. Additionally, the attitudes and perceptions of the HCWs were only observed using a quantitative questionnaire. A mixed-methods approach by incorporating the qualitative data collection methods could have given a comprehensive understanding of the perceptions and attitudes of HCWs. Furthermore, the lack of multivariate analysis of data also serves as a limitation of our study.
CONCLUSIONS
The COVID-19 vaccine uptake was high among HCWs in the Velhe and Haveli blocks of the Pune district. The predominant concerns towards COVID-19 vaccination in the minds of HCWs that impact vaccination uptake need contextual training at regular intervals and constant communication to improve vaccine coverage in society. There is also a need to develop public health messaging and communication strategies (mobile-based app) to address the specific reported gaps and the positive factors associated with COVID-19 vaccination among the HCWs in our study. Our study findings will also provide useful information to plan future interventions and improve COVID-19 vaccination acceptance among the community. Further studies with a larger representative sample size are needed to assess future uptake of booster/ precautionary dose of COVID-19 vaccine.
Funding
This work was supported by AXA Business Services as part of their Corporate Social Responsibility (CSR) to Public Health Foundation of India.
The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Authorship contributions
All authors contributed to the study and manuscript.
Competing interests
The authors completed the Unified Competing Interest form at https://www.icmje.org/disclosure-of-interest/ (available upon request from the corresponding author), and declare no conflicts of interest.
Correspondence to:
Shalini Bassi
Public Health Foundation of India (PHFI), Gurugram, Haryana, 122002, India.
[email protected]