Pediatric pneumonia remains a major public health problem. Pneumonia is the world’s leading infectious killer of children, claiming the lives of more than 922,000 children under five years annually and more than 2,200 every day.1 Integrated Global Action Plan for prevention and control of pneumonia aimed at 90% access to appropriate pneumonia case management by the end of 2030.2 Globally, about 16% of deaths in children under five years is due to pneumonia, and healthcare-seeking levels are at 58 %.3 In Kenya, pneumonia accounts for 16% of all child deaths and is the second biggest killer of children under five years.4 A report by Endebess Sub-county health information department indicated 3283 (47.7%) and 2842 (41.3%) new cases of pneumonia in 2017 and 2016, respectively.5 In addition, pneumonia is the leading cause of morbidity in children under five years in Endebess Sub-county.5 However, progress in reducing deaths due to pneumonia in children under five has been significantly slower than in other infectious diseases.6 The slow progress may be attributed to poor health-seeking behaviour of caregivers whose children were under five years as evidenced by the caregiver’s history of the presenting illness of taking 1-14 days before visiting a health facility for treatment.5
Early care-seeking for children with pneumonia symptoms from hospitals reduces child mortality. However, in recent years care-seeking for children with acute respiratory infection symptoms from a healthcare provider has stagnated in Western and Central Africa as well as in Eastern and Southern Africa.7 Furthermore, in Sub-Saharan Africa, where most pneumonia deaths occur, less than 50% of children with pneumonia symptoms are taken for the care, with the lowest proportions in rural areas.7 Locally, in Kenya, healthcare-seeking levels for acute respiratory infections is at 67%, which is below the recommended 90% global coverage.8 Therefore improving coverage and access to child health services is a priority for the government of Kenya.
Delay in seeking health care may be associated with hospital practices and prescription patterns by health care personnel. For example, in Uganda, health facility deterrents known to influence health-seeking were: the attitude of healthcare providers, the lateness of staff and the lack of drug supply.9 Additionally, in Malawi, lack of medicines and supplies, long waiting times, late facility opening times, negative attitude of health workers, and suboptimal examination of the sick child were cited as critical health system factors affecting health-seeking for child health services.10 In Kenya, specifically in Homa-bay County, the important deterrents included prolonged waiting times, poor communication between staff and patients, previous negative experiences resulting in caregivers losing trust in health services, and fear of being tested for HIV when presenting their child for treatment.11 In addition, caregivers were frustrated by the lack of reliable drug stock at their local health facility; most participants volunteered examples of when they had presented for treatment only to be turned away or sent to a private chemist to purchase medication.11 In Peruvian, delays in reaching a health facility were not reported; however, once the caregivers reached a health facility, they perceived a lack of competence of medical staff and inadequate treatment provided by the primary care physicians.12
Despite the evidence of the influence of health facility practices on health-seeking in the context of childhood pneumonia, health facility practices such as adherence to clinical instructions and shared decision making on the choice of the antibiotic route remain unknown in Kenya. Shared decision making is a practice whereby clinicians and patients/caregivers make decisions together using the best available evidence. Patients are encouraged to consider available screening, treatment, management options, and the likely benefits and harms.13 Increasing clinical evidence demonstrated that patient involvement in medical decision making significantly improved health care outcomes, and therefore shared decision-making remains central to the patient-centred care movement.14 Many health care decisions are based on treatment and screening options while considering costs and benefits that are valued differently by individual caregivers and their families. Shared decision making considers patient needs, values, and preferences as part of the medical decision-making process. Such consideration increases patient confidence in medical decision outcomes by reducing uncertainty and decisional conflict and improving treatment adherence. A goal of healthcare currently is evidence-based, patient-centred decision making, and the importance of shared decision making in combination with patient-reported outcomes is stressed in the treatment of patients.15 Unfortunately, several studies have shown that patient involvement in decision making was poor worldwide.16
There is evidence that informed medical shared-decision making, allowing caregivers of children with pneumonia to share in choosing injectable or oral antibiotic therapy, helped improve caregivers’ satisfaction with pneumonia treatment in Italy.17 However, shared decision making on the choice of antibiotic routes in the context of pediatric pneumonia in Kenya remains unclear and unknown. The information obtained from this study was to help health care providers appreciate the importance of caregivers’ wishes and choices. Most caregivers satisfied with the proposed treatment plan would continue to give the prescribed medication at home and even observe return dates to the health facility for review, which they rarely do.
Adherence to treatment instructions was another health facility-related practice of great importance. Adherence refers to sticking firmly to the treatment instructions given by a health care provider, more so drug instructions. In Zambia, 46 % of caregivers adhered to treatment and gave their children the entire 5-day course of dispersible amoxicillin, while some caregivers administered the prescribed antibiotics for 3 to 4 days.18 A study done in Kenya reported that despite global treatment recommendations that call for children with pneumonia to receive amoxicillin dispersible tablets, only one–third of children with pneumonia received any antibiotics, and many did not complete the entire course of treatment.19 There was a need to document if the instructions given to caregivers were adequate to promote better adherence to the prescribed treatment.
Lastly, antibiotic therapy for severe pneumonia involves the administration of injectable penicillin and gentamicin, while oral antibiotic therapy for pneumonia is amoxicillin dispersible tablets.20 WHO,21 reported that children with suspected pneumonia do not receive life-saving treatment, and only 31% received appropriate antibiotics. Pneumonia guidelines revealed that oral amoxicillin is just effective in treating pneumonia as the injectable benzylpenicillin.22 Agweyu et al.,23 also confirmed no inferiority of amoxicillin to benzylpenicillin in Kenya. The new pneumonia guidelines recommend treatment using a high dose of amoxicillin dispersible tablets.24 Shockingly, only 33% get appropriate antibiotics.24 The question is what is prescribed for the remaining 67%. However, despite the confirmation, some caregivers strongly believe that their children can only be cured through injections compared to oral medications, but it is not always the case. Some caregivers seek inappropriate alternative care when injectable antibiotics are not prescribed for their children. The alternative inappropriate health care provider may administer sub-standard medication, which can either be an overdose or underdose. This may lead to disease recurrence, drug resistance, permanent injury to nerves and abscess if the injection is not administered well, prolonged, expensive illness, and lastly, death. It was essential to understand how shared decision-making on the choice of antibiotic route influenced health-seeking behaviour to avert pneumonia-related complications and deaths when the caregiver seeks inappropriate alternative care when dissatisfied with the prescribed antibiotic route. In this study, health facility practices referred to activities surrounding the service of providing medical care at health institutions. It involves the management and treatment of pediatric pneumonia and the communication of health information between the caregiver and healthcare provider in pediatric pneumonia. The dependent variable for this study was appropriate health-seeking behaviour, and it referred to the preference or willingness of the caregivers to revisit the same health facility if given the opportunity and on subsequent visits.
METHODS
Study setting
The study site was Endebess Sub-county Hospitals, Trans-Nzoia County in Kenya. Endebess has 130,747 people, 22,620 children under five, and 21,525 households with 14 community units and seven public hospitals.5 It is estimated that in 2018 pneumonia cases in children under five years was 3421.5 It is mainly a rural setting, and most residents engage in agricultural activities and small scale businesses. The departments considered for the study were inpatient and outpatient departments. The inpatient department was only applicable to the Endebess sub-county hospital since other health facilities do not offer inpatient health services. According to patient files, the mean duration of admission due to paediatric pneumonia is three days (Min 1; Max 7). Oxygen therapy is only available in two health facilities: Endebess sub-county Hospital and Chepchoina Health Centre. In case of requirement for referral services, one ambulance stationed at Endebess Sub-County Hospital serves the whole sub-county. A hospital-based descriptive cross-sectional study using a quantitative approach and qualitative study among caregivers of children with pneumonia and health personnel was conducted between May 2019 and August 2019. The study design was preferred because there was no waiting for the outcome to occur, and there was no loss to follow-up.
Study population
The study population consisted of caregivers of children under five years with pneumonia seeking care at Endebess Sub-county hospitals and health personnel working in Endebess sub-county health facilities. The cadres of health personnel included in the study were medical officers, nurses, and clinical officers. The participants consented to participate in the study. Caregivers who were mentally challenged were excluded. In addition, caregivers whose children were diagnosed with a second medical condition other than pneumonia were excluded.
A simple random sampling technique made the identification of study subjects. The process began using the column on diagnosis in outpatient and inpatient under five register to identify and list all children with pneumonia. All caregivers of children under five years with pneumonia were informed about the study. Next, numbers were written daily, and caregivers who picked even numbers and met eligibility criteria and gave consent were included in the study. The following day those who picked odd numbers were included. This was repeated until a threshold sample size of 273 caregivers was reached. Caregivers of children <- five years were proportionately sampled for participation in the study from 7 hospitals depending on the percentage contributing to pneumonia cases to obtain the sample size of 273 (Table 1). For a qualitative study in the health personnel, all 24 healthcare workers were included as key informants.
Data collection procedures
Data collection was preceded by a pilot study under which the validity and reliability of data collection instruments were determined by test-retest reliability. Intraclass correlation coefficient (ICC) was used, and a reliability coefficient of ≥ 0.5 was considered reliable. ICC was computed by a single measurement, absolute agreement and a two-way random-effects model. The obtained values indicate good reliability (P<0.001; ICC=0.896, 95% confidence interval, CI=0.870-0.917). Therefore the test-retest level of reliability ranged from good to excellent. The interviews were conducted in inpatient and outpatient department consultation rooms. Face to face interviews of caregivers of children under five years and health personnel were conducted by trained research assistants using a questionnaire and key informant interview guide (KIIs). Participants’ responses were recorded by note-taking. Patient files and booklets were used to verify data on the names of the prescribed drugs.
Data management and analyses
The data collection tools were checked for completeness. Quantitative data was coded, edited and cleaned to check for any errors. Qualitative data was organised in tables depending on the emerging themes. The data were entered into an excel worksheet and then verified to ensure that subject identification numbers matched with the data in the questionnaires. After that, the data was imported into IBM SPSS Version 22. Statistical significance was determined using chi-square and logistic regression at a statistical significance below 0.05. Chi-square was used to compare differences in pneumonia care and management practices and differences in information shared. The logistic regression model was fitted to determine the relationship between prescription patterns and health-seeking behaviour. Qualitative data from Key informant interview guides (KIIs) was analysed by searching for emerging themes and presented in textual form.
Ethics considerations
Ethical Review Board of the University of Eastern Africa, Baraton (Ref No: UEAB/06/03/2019) and the National Commission for Science, Technology and Innovation in Kenya (NACOSTI/P/19/32404/29550) approved the study. Endebess Sub-county Medical Officer of Health granted permission to conduct the study in Endebess.
RESULTS
Participants’ demographics summary
Table 2 summarises the socio-demographic characteristics of the respondents. The social-demographic aspects of the respondents interviewed included gender of the caregiver, the caregiver’s relationship to the child, age of the caregiver, marital status, age of the child, occupation, household income and education level. The majority, 263 (96.3%) of respondents, were female, with 252 (92.3%) being mothers and only 10 (3.3%) fathers. Slightly below half of the respondents, 115 (42.1%) were aged between 25-34 years, and 246 (90.1%) were married. More than half of the children, 147 (53.8%), were aged between 0-12 months, the primary occupation was business 96 (35.2%), with only a few, 21 (7.7%), being formally employed. Most 187 (68.5%) respondents had household income less than Kenya Shilling (KES) 5,000 (United States Dollas, USD 45.57), with only 15 (5.5%) earning more than KES 10,000 (USD 91.12). Slightly more than half, 137 (50.2%) attained secondary education.
Relationship between socio-demographic characteristics and health-seeking behaviour
There was a significant relationship between household income (P=0.029) and willingness to revisit the health facility, level of education (P=0.038) and willingness to revisit a hospital. Most 13 (86.7%) respondents with a household income of KES > 10,000 (USD >91.12) preferred to revisit the hospital if given the opportunity as compared to the 108 (41.9%) with an income bracket of KES <5,000 (USD <45.57). In addition, among caregivers with a college education, 16 (69.6%) were willing to revisit the health facility as opposed to primary levers 51 (48.1%) (Table 3).
Relationship between care, management and health-seeking behaviour
This study compared various hospital practices and health-seeking behaviour. Chi-square results show that health-seeking behaviour was significantly associated with the availability of drugs (P<0.001), administration of a starting dose at the health facility (P<0.001), type of medication prescribed (P<0.001), place caregiver seeks treatment (P=0.001), the willingness of the caregiver to recommend the facility to a friend (P<0.001), and if the caregiver is always treated at the health facility (P=0.001) (Table 4). More than half, 146 (71.6%) of caregivers who received all the prescribed medication at the facility, if given a chance, could revisit the facility (Table 4). In contrast, 52 (75.4%) who missed some drugs could not wish to revisit the facility (Table 4). Caregivers of 112 (87.5%) whose children received starting doses at the health facility preferred to revisit the facility; likewise, without a starting dose being administered, ninety-four (64.8%) caregivers could not honour return dates (Table 4). 86 (90.5%) caregivers preferred injection medication, as evidenced by the preference to revisit the facility (Table 4). More than half of caregivers, 34 (55.7%) whose first treatment contacts were local shops and herbal medication, preferred not to revisit the hospital. However, caregivers 136 (64.2%) who visited chemists and hospitals could revisit health facilities (Table 4). In addition, a logistic regression determined the relationship between the choice of antibiotic therapy and appropriate health-seeking behaviour. The logistic regression model did not fit well (X2=0.851, P=0.380). However, the model explained a 4% variance inappropriate care-seeking and correctly classified 59.7% of cases. Therefore the odds of appropriate care-seeking are 2.06 times greater among caregivers who had an injection medication prescribed for their children (P=0.380; OR 2.064, 95% CI 0.409-10.417) than those on oral medication.
The preferred route of antibiotic therapy
Among the respondents, 265 (97.1%) preferred injection medication as compared to oral medication 8 (2.9%), as shown in (Table 5).
Reasons why respondents preferred injection medication
Respondents preferred injection to oral medication because of the following reasons: belief that injection is more effective 144 (52.7%), the injection acts faster 68 (24.9%), it enhances fast recovery 32 (11.7%), the children could not vomit 18 (6.6%), and injection was strong 7 (2.6%) as shown in Table 5. The minority preferred oral medication because they feared their children being pricked 3 (1.1%) and believed it was effective as injection medication 1 (0.4%), as illustrated in Table 5.
Reasons for preference of private hospitals for respondents not willing to visit the health facility again
Generally, 108 (68.4%) caregivers, if given the opportunity, would visit the same health facility, and interestingly, some 50 (31.6%) could not wish to go back; instead, they preferred private hospitals (Table 4). Preference for private hospitals was related to waiting time of less than one hour 4 (16.67%), proper assessment of the child 3 (12.5%), there is shared decision making about medication routes, whether oral or injection 5 (20.83%) and return dates for injection is given 12 (50%) (Table 5).
Satisfaction levels depend on the medication prescribed
For most respondents whose satisfaction level was very satisfactory, 108 (39.56%), the clinician had prescribed injectable antibiotic therapy, namely benzylpenicillin and gentamycin, as evidenced by the responses (Table 6). However, oral medication was prescribed for most caregivers whose satisfaction levels were bad 104 (20.87%) or very bad 4 (1.47%), as illustrated in Table 6.
Why satisfactory levels were bad or very bad
Half of the caregivers, 55 (50.5%), were dissatisfied because of the lack of drugs (Table 5). Some complained that their children had used oral medication at home without improvement, yet the clinician had prescribed it again 27 (24.8%) (Table 5). 21 (19.3%) were not happy that their children were not given an injection (Table 5). A small number 2 (1.8%) of caregivers based their frustration on long waiting times of more than one hour, no injection prescribed by the caregiver yet had administered the same drugs as what had been prescribed at home 2 (1.8%), bad attitude from health personnel 1 (0.9%) and the child cried a lot during intravenous drug administration 1 (0.9%) (Table 5).
Patterns of prescription in different health facilities
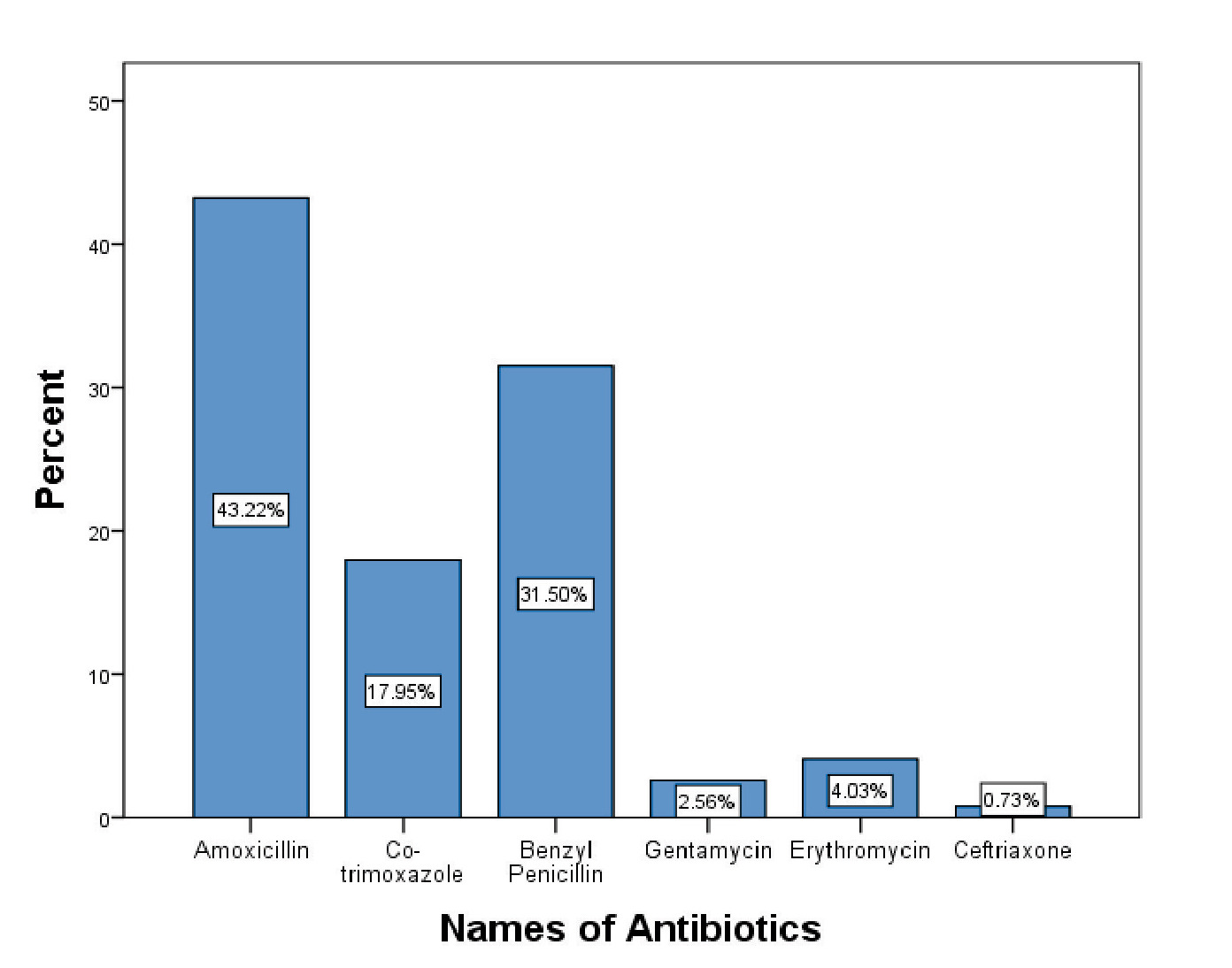
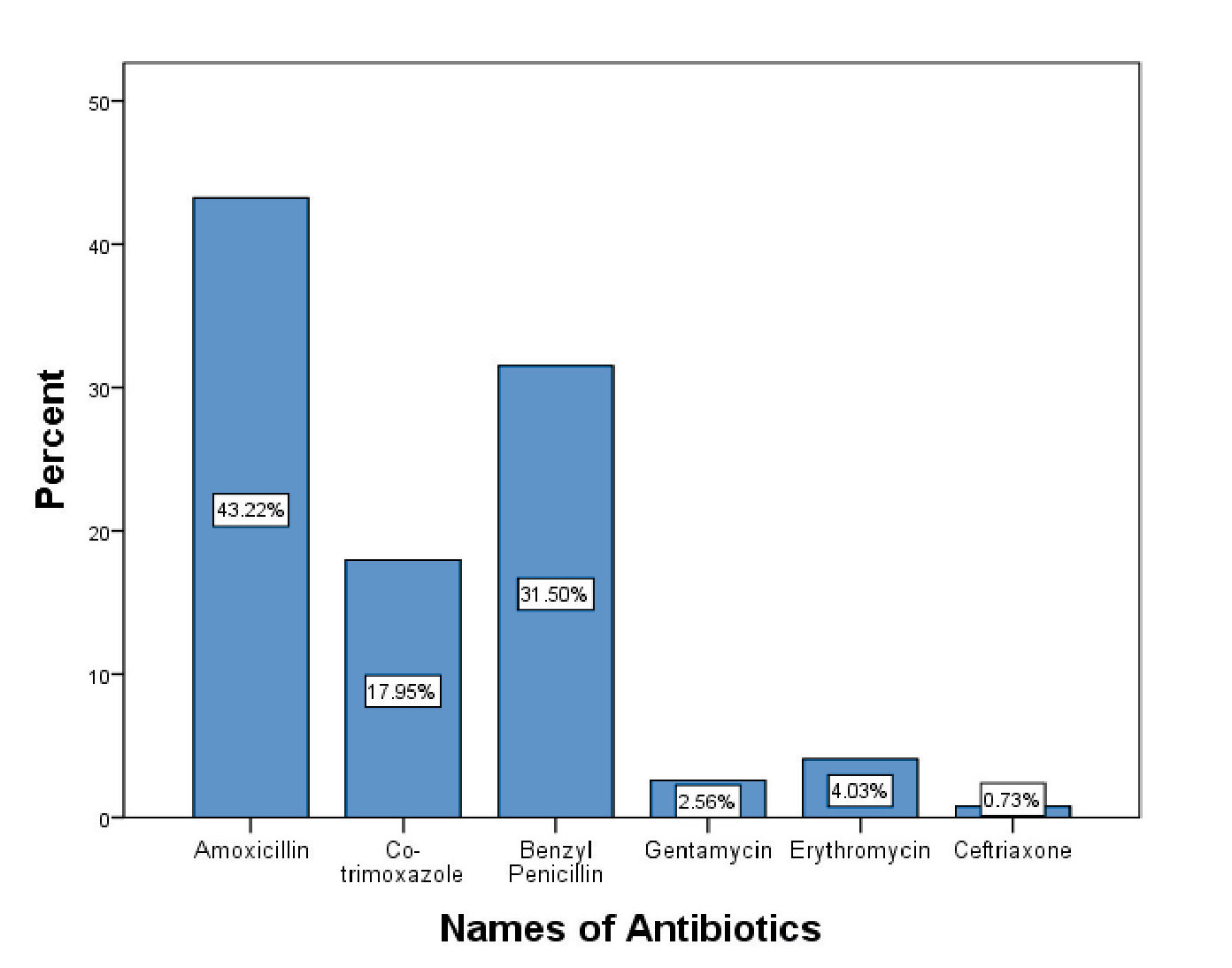
There was slight variation across hospitals in managing pediatric pneumonia. In all the health facilities in the Sub-county, the oral antibiotics of choice were amoxicillin 118 (43.2%), followed by co-trimoxazole 49 (17.9%) and erythromycin 11 (4%) (Figure 1). However, some health care workers preferred injectable medication such as benzylpenicillin 86 (31.5%), gentamycin 7 (2.6%) and ceftriaxone 2 (0.7%), as shown in Figure 1. Prescription of injection medication was dominant among health personnel in Endebess sub-county hospital 25 (49%), Kitum dispensary 15 (34.9%), Matumbei dispensary 6 (35.3%) and Chepchoina health centre 15 (31.3%) (Table 7).
Association between information given and health-seeking behaviour
This study further compared the health information given with health-seeking behaviour. From Table 8, chi-square results show that health-seeking behaviour was significantly associated with adequate instructions on how to administer the medications (P<0.001), the confidence of the caregiver to administer the correct dose of the drugs at home (P<0.001), the ability of the caregiver to recommend the facility to someone else (P<0.001), respondent satisfaction levels (P<0.001) and shared decision making on the choice of antibiotic therapy (P=0.005). All Key informants, 24 (100%), agreed that the shared decision on the antibiotic route was not being practised at the health facilities. This was attributed to the belief by the healthcare workers that the caregivers had a knowledge deficit and therefore had much confidence in the decision of their healthcare providers 9 (37.5%). In addition, the health care providers also stated that there was a belief among caregivers that injectable medication was more effective and would always be preferred by the caregivers if given the opportunity 15 (62.5%) (Table 8).
DISCUSSION
Based on the study findings, there is a significant association between the availability of drugs, preference for administration of a starting dose at the health facility, and health care seeking. Most caregivers who did not receive prescribed drugs in health facilities preferred to visit private hospitals. The findings are similar to a different study in Kenya.11 Limited supply of drugs may be attributed to more demand for drugs than what is supplied. For instance, treatment of children under five years is free in dispensaries and health centres in Kenya.
Regarding patterns of the prescription, most caregivers who were satisfied with the prescribed medication route had an injection prescribed for their children and preferred seeking treatment in the same facility in subsequent visits. On the other hand, other caregivers were dissatisfied with the oral medication. In contrast, this study’s findings differ from Agweyu et al.,23 reports on the acceptability of amoxicillin dispersible tablets and oral suspension in the treatment of pediatric pneumonia in Kenya, which revealed high levels of acceptability among both dispersible tablets (93.9%) and oral suspension (96.1%). The same report also revealed good adherence to the same oral medication.23 This difference might be due to a difference in the socio-demographic composition of the caregivers, given that Endebess Sub-county serves clients from West Pokot county and Uganda. In this study, the caregivers’ dissatisfaction was based on the following reasons: no injection prescribed for their children, no injection prescribed yet the caregiver had administered the same oral drugs at home as what the clinician had prescribed for the child, the caregiver having administered oral medication at home without improvement. Some of the reasons could be attributed to the belief by the caregivers that injection was more effective than oral medication.
This study also showed a diversity of prescriptions among health personnel. The dominant antibiotics prescribed were Amoxicillin 118 (43.2%) and Benzylpenicillin 86 (31.5%). It was evident that injectable medication like Benzylpenicillin, Gentamycin and Ceftriaxone meant for severe pneumonia was not limited to inpatient care in Endebess sub-county hospital but was also extended to outpatient care meant for non-severe cases in other rural health facilities in the sub-county. This may be attributed to the presence of newly employed health personnel in rural health facilities, which are yet to be inducted into the current guidelines for managing childhood pneumonia. Consistently, two studies in Italy and India reported an increase in antibiotic prescription in paediatrics with respiratory infections.25,26 In addition, the percentage of encounters with injectable antibiotics is still high. This means that prescribing patterns, according to World Health Organization, are less likely to be followed. More injection prescriptions may be related to a knowledge deficit on the current guidelines. In line with other studies in Tanzania and India, the investigators found that more than a quarter of all admitted children with pneumonia received injectable instead of oral antibiotics.27,28
It was evident from this study that satisfaction levels on medication routes were a determinant of appropriate health-seeking behaviour during childhood illness. Similarly, in Italy, the study on satisfaction levels of caregivers revealed that allowing caregivers of children with pneumonia to participate in shared decision making on the choice of antibiotic therapy improved caregivers’ satisfaction levels.17 Respondent’s satisfaction with the information given also influenced care-seeking, such as adequate instructions on administering drugs at home, confidence to give the prescribed dose, and discussion on the choice of antibiotic therapy. This may be due to caregivers’ full participation in the care and management of their children. The findings were consistent with study findings at Homabay County in Kenya, which identified satisfaction with care and treatment as a health facility factor influencing health-seeking behaviour.11 Additionally, in a different study in Kenya, respondents who rated the service as satisfactory were more likely to seek health-related help than those who reported dissatisfaction.29 Concerning individual characteristics, household income and level of education were significant predictors of willingness to revisit the health facility. Most caregivers with a household income of more than KES 10,000 (USD 91.12) preferred to revisit the same facility. The reason may be that some caregivers who missed some drugs had money to purchase the out of stock drugs from private chemists and the primary interest was a prescription from qualified health personnel. In addition, most caregivers with a high level of education could not mind revisiting the hospital compared to those with a low level of education. A knowledge deficit may explain this among caregivers with a low level of education and the assumption that government health facilities do not offer quality care. The findings have been reported in similar settings.29
Limitations of this study relate to the possibility of recall bias because of self-reported information and a small number of health personnel. The possibility that caregivers forgot some information could not be excluded. However, this was minimised by verifying some caregiver responses, like the names of prescribed medications documented in patient files and booklets. The study was also limited to 24 health care personnel because of low staffing levels in the rural health facilities. Therefore all health personnel were included in the study. Despite the limitations, after data analysis, it was evident that prescription and health facility practices influence health-seeking behaviour in Endebess Sub-County, Kenya.
CONCLUSIONS
This study established slight variation in care and management of pneumonia in different health facilities, though most caregivers preferred injection medication to oral medication. On the other hand, communication of health information determines appropriate care-seeking behaviour. Therefore, this study demonstrates that continuous medical education among health care workers is critical to improving patterns of prescription based on current pneumonia treatment guidelines. It is critical for health facilities to stock adequate drugs, mostly antibiotics and non-pharmaceutical commodities, to strengthen service delivery. The health management team needs to carry out regular supportive supervision on adherence to pneumonia management guidelines and policies in health facilities by conducting audits of pediatric pneumonia files from time to time. In addition, the government should employ more health personnel to curb staff shortages.
Consequently, health personnel should consistently demonstrate to caregivers how to give the prescribed drugs at home. Caregivers need to be counselled on follow-up care in 2 days for review, to complete the prescribed dose, and to intensify efforts to reduce the long waiting time of more than one hour during hospital consultations. Future studies to compare alternative antibiotics and supportive care approaches to pediatric pneumonia should be considered.
Acknowledgements
The authors acknowledge all caregivers of children for their cooperation. We would also wish to express our deepest gratitude to the Endebess Sub County health management team for permitting us to conduct the study in their area.
Data Availability
The data used to support this study’s findings is available from the corresponding author upon request.
Funding
No funding was received for this study.
Authorship contributions
All authors contributed to the conception, design and implementation of the study. ENO did analysis and interpretation of data. All authors contributed to the drafting and revision of the manuscript. All authors read and approved the final manuscript.
Competing interests
The authors completed the Unified Competing Interest form at www.icmje.org/coi disclosure of interest form (available upon request from the corresponding author) and declare no conflicts of interest.
Corresponding author:
Everlyne Narano Opuba
Master of Science in Epidemiology and Biostatistics
Division of Vaccines and Immunisation
Ministry of Health, Trans-Nzoia County
Kitale, Kenya.
[email protected]