Globally, about 38 million people were living with HIV in 2019, with 1.7 million people newly infected with HIV in the same year.1 While men who have sex with men (MSM) make up a modest proportion of the global population of people living with HIV (PLWH), they are at extremely high risk for HIV infection, with the risk of HIV acquisition among this population 26 times higher than it was among all adult men in 2019. MSM accounts for an estimated 23% of new HIV infections globally and about 44% in Asia and the Pacific.2 Although new HIV infections have reduced by 23% from 2010 to 2019, HIV infections among MSM have increased by about 25%.3
A meta-analysis of 355 cross-sectional studies covered 40 provinces and municipalities of China estimated the overall national prevalence of HIV among MSM was 5.7% (95% CI: 5.4-6.1%) from 2001 to 2018, with an upward trajectory over time.4 The HIV prevalence among Chinese MSM is higher than the rate found in the general Chinese population (< 0.1%).5 MSM in China are estimated to account for about a quarter of new infections.6,7
Benefits of antiretroviral therapy
Antiretroviral Therapy (ART), introduced in the late 1990s, increased the life expectancy of people living with HIV (PLWH) and transformed their quality of life. Formerly a life-threatening condition, HIV now became a chronic disease that can be managed with lifelong treatment.8 Early ART initiation is beneficial at both individual and population levels. A large international, randomized study reported that immediate initiation of ART has clear benefits in reducing serious AIDS-related and non-AIDS-related events (e.g., bacterial infectious disorder).9 Another randomized study on 2,056 HIV-infected adults reveals that the risk of HIV-related illness and death is 44% and 35% lower, respectively, in the early ART initiation group than their counterparts in the deferred initiation group.10 At the population level, mathematical modeling predicts that ART initiation immediately after diagnosis would decrease HIV incidence rates.11–13 Results from the HIV Prevention Trials Network also suggest that early initiation of ART significantly reduces HIV transmission among couples by inducing viral suppression (< 200 copies per milliliter).14,15
Following WHO’s recommendations on when to start ART, China updated the national guidelines and began providing free ART to all PLWH regardless of their CD4 levels in June 2016.16 Data from the National Free Antiretroviral Treatment Programme (NFATP) suggest that receiving ART is associated with virological suppression, increased CD4 counts, and a significant decrease in mortality.17–19 A retrospective cohort study on 34,581 PLWH with CD4 > 500 cells/μl reported that ART initiation within 30 days following diagnosis was associated with more than 60% reduction in mortality.20
Despite these benefits, ART coverage was estimated to be 67% (95% CI: 54-79%) globally and 60% (95% CI: 43-75%) in Asia and the Pacific in 2019.2 ART coverage in China has been increasing steadily and was estimated to be 80.4% by the end of 2017.21 However, MSM who are living with HIV often reported lower ART coverage rates compared to national coverage rates.22,23 Limited literature suggests that the ART coverage rates range from 26.1% in 201124 to 60.3% in 2016 among MSM in China.16
Factors associated with ART initiation
A review of 11 studies conducted in Canada, the UK, and Australia summarized a set of interconnected factors that affect utilization of HIV treatment, including intrapersonal barriers (e.g., risk of unwanted disclosure of HIV status, negative beliefs around the benefits of ART medications, mental health problems such as depression), interpersonal barriers (e.g. poor relationships with family, lack of social support), and extrapersonal barriers (e.g., costs of ART, a high threshold for eligibility for ART subsidies, financial hardship).25 Education, stronger social network support, disclosure of status, and greater satisfaction with social support, having a regular partner, and lower CD4 count are associated with greater initiation of ART.26–28 Nonetheless, few studies have examined the correlates of ART initiation among MSM in China, a country with more than 18% of the global population. A study on 238 MSM participants in Beijing, China reported that older age, having a Beijing Hukou (official residential status), being married to a woman, longer duration of HIV infection, experiencing opportunistic infections, and sexually transmitted infections are associated with ART initiation.24 A study of 364 MSM living with HIV in Beijing, China reported that participants who scored higher on the Hospital Anxiety and Depression Scale (HADS) are more likely to initiate ART in the 12-month follow-up period after HIV diagnosis.29 Older age, having local Hukou (or legal residency), and time since HIV diagnosis are also found to be associated with ART initiation by among 227 participants in Chengdu and Hangzhou, China.16
Given the lack of knowledge of ART initiation rates among MSM in China, the first aim of this study was to report the ART initiation rate in this sample. The second aim was to further explore and conceptualize the correlates of ART initiation among MSM in China using Andersen’s Health service Utilization model.30 This model offers a theoretical framework to understand the individual and social determinants of health service utilization.31 According to this model, the dynamic set of factors that influence the utilization of health service can be categorized into predisposing (demographic and social structure), enabling/disabling (individual, family, and community resources), and need (the degree of symptoms, chronic disease, and general health) factors.
Depending on the specific health services, the three sets of factors are hypothesized to differ in their ability to predict and explain use. Specifically, healthcare utilization for serious medical problems would be mainly explained by demographic and need factors, while optional services such as dental service use would be mainly explained by enabling factors.30 Given that HIV/AIDS is a potentially life-threatening medical condition coupled with China offering free treatment for all PLWH, we hypothesize that demographic and need variables will be the strongest predictors of ART initiation, followed by enabling/disabling factors would not be as predictive.
METHODS
Data collection
Data for these analyses were derived from a larger study examining HIV-HCV co-infection among MSM in China. Participants were recruited using snowball sampling in Chengdu and Shanghai, China, between 2014 and 2016. Local non-governmental organizations specializing in HIV prevention among MSM assisted with participant recruitment and enrollment. Eligible participants were HIV positive, at least 18 years of age, and reported ever having anal or oral sex with men. Eligible index case participants were first recruited and then given an egocentric contact tracing survey to solicit as many sexual partners in the past three months as they could recall.
The people mentioned on the list were then contacted and invited to perform HIV testing in the non-governmental organizations. Experienced nurses performed phlebotomy and collected plasma samples. The samples were then screened for HIV antibodies using an enzyme-linked immunosorbent assay (ELISA) and confirmed by Western blot. Those who tested positive for HIV received post-test counseling and were advised to start free ART treatment. These participants also filled out the contact tracing survey to invite their sex partners for HIV testing and participation in the study. A detailed description of the egocentric behavioral network design is documented elsewhere (Xu et al., manuscript under review). All participants also filled out a questionnaire about their demographic information, depression, sexual risk behaviors, and intimate partner violence (IPV).
Measures
Demographics
Demographic information collected including participants’ age, Hukou, ethnicity, marital status, educational background, and monthly income.
Clinical variables
The information about participants’ HIV status, CD4 count, and Hepatitis Type C infection was collected from the blood samples. Participants who are aware of their HIV-positive status were then asked if they have initiated ART.
Depression
Depression symptoms were assessed with the Center for Epidemiologic Studies Depression Scale short form (CES-D). This scale captures the severity of depression symptoms in the past week with 12 items (e.g., “You were bothered by things that usually don’t bother you”). Participants responded on a 4-point Likert scale, from rarely or none of the time = 0 to all of the time = 3. Clinically significant depression is suggested by a score equal to or higher than 9. The scale was translated from English to Mandarin using forward and backward translation and was used in several studies conducted in China.32 Cronbach’s alpha was 0.92 in this sample.
Sexual risk behaviors
Participants indicated the number of male sex partners that had in the past 12 months by choosing from none, 1, 2-4, 5-7, 8-9, or more than 10. Participants answered “Yes” or “No” to seven types of sexual risk behaviors in the past 12 months, including unprotected sex with a primary partner, unprotected sex with a sex worker, unprotected oral sex, unprotected anal sex, unprotected sex with casual sex partners, unprotected sex after alcohol, and unprotected sex after drug use. In this paper, we used unprotected anal sex in the analysis because its prevalence has been increasing among MSM.33
Intimate partner violence
IPV in the past five years was measured with seven items (hit you or threw something at you, threatened to stop helping you with money or with housing, verbally threaten to harm you physically or emotionally, verbally threatened to physically or emotionally harm someone you care for, forced you to have sex, damaged or destroyed your property, threatened to tell others the sexual relationship between you two), which were adapted from a study by Dunkle et al. on MSM in China and was later used in other studies.34 Participants indicated the number of each IPV incidence they experienced in the past years. The item about forced sex was selected for inclusion in the analyses because of its high HIV transmission risk.
Data analysis
Descriptive analyses were performed to summarize participants’ characteristics and clinical variables. Stepwise logistic regressions were then used to test the incremental contribution of each block of independent variables to improve the predictive accuracy of the model. Specifically, the ART initiation variable was used as the dependent variable, and the independent variables were entered sequentially in the following steps: Step 1: predisposing factors, including age, Hukou, and ethnicity; Step 2: enabling/disabling factors, including depression, marital status, education background, monthly income, employment status, and retirement status; and Step 3: need factors, including HCV status, CD4 count, unprotected anal sex in the past 12 months, number of sex partners in the past 12 months, and forced sex.
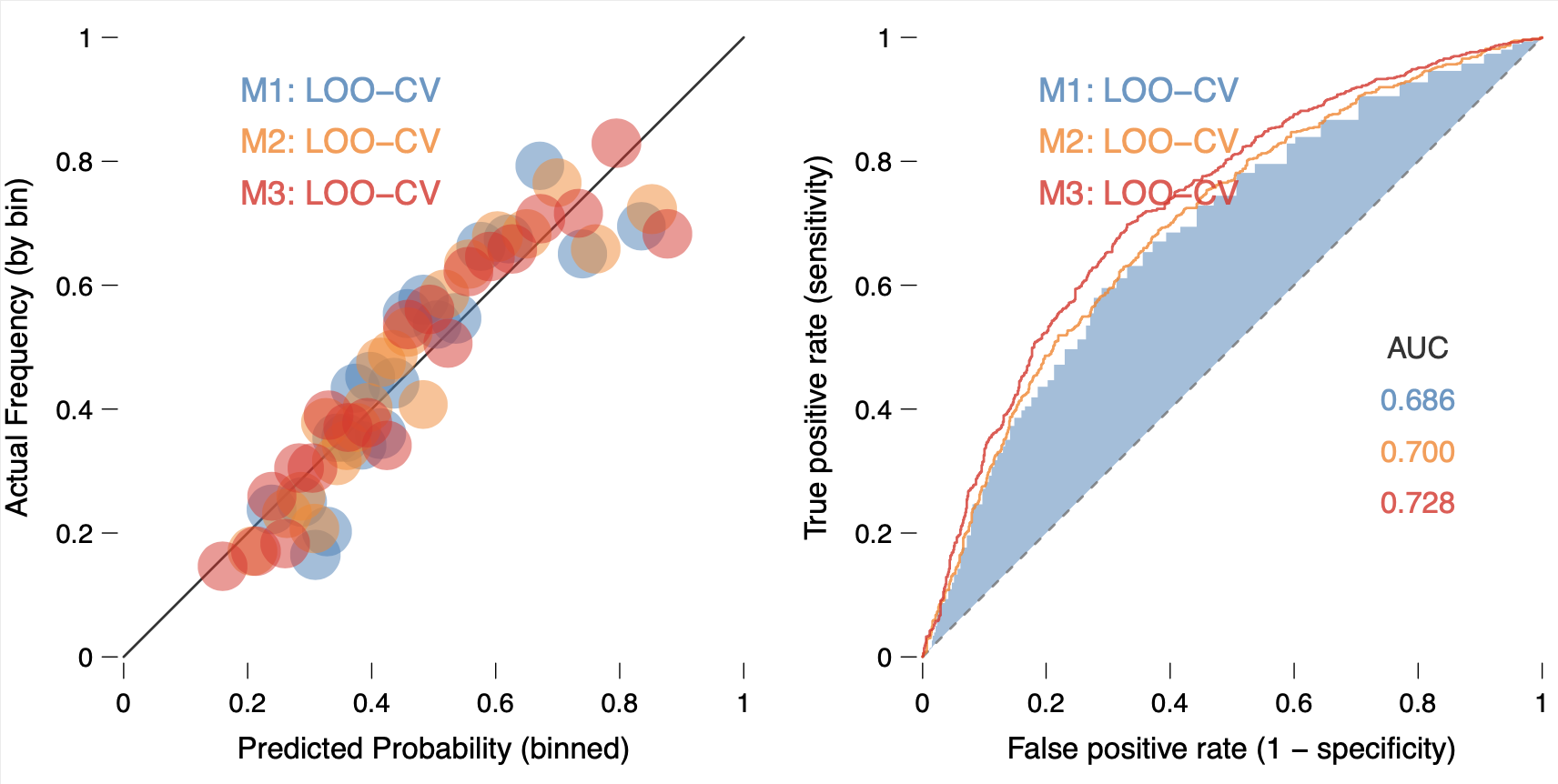
The analyses added each block of independent variables into the regression model successively. The relative importance of the variables in the final model was indicated by the absolute value of the odds ratio and the uncertainty is captured by 95% confidence intervals. The fit of the models across three steps was compared using the likelihood ratio test, AIC, BIC, and Leave-one-out Cross-Validation (LOO-CV). A confidence interval that does not include 0 was considered to indicate statistical significance. All analyses were performed with R statistical packages.
RESULTS
Participants
The characteristics of participants are shown in Table 1. There were 2,651 participants and 1,633 participants were left in the dataset after filtering out HIV-negative participants and incomplete cases. More than half (53.5%) of the HIV positive MSM participants had not initiated ART. The mean age of the participants was 33.0 ± 10.1 years, with a range from 16 to 93. More than half of the participants had a non-local hukou (59.6%), received an education that is college or above (56.2%), and earned a monthly income over 3000 RMB (about US$458.20, 63.0%). The majority (70.6%) of the participants were never married. Almost all participants were of Han ethnicity (97.5%), employed (97.4%), and not retired (97.7%). More than half of the participants (58.1%) had white-collar jobs. Only 14 participants (0.9%) tested positive for Hepatitis Type-C. The mean CD4 count was 395.3 cells/mm3 ± 181.7 , ranging from 4 cells/mm3 to 1600 cells/mm3. More than 60% of participants reported condomless anal sex in the past 12 months. Only 66 participants (4%) reported having more than 10 sex partners over the past 12 months.
Predictors of ART Initiation
The results of the hierarchical multiple regression models for ART initiation are shown in Table 2. A few variables from each block were significant predictors of ART initiation. In the block of predisposing factors, age and ethnicity were significantly associated with ART initiation. Specifically, older participants (OR = 1.08, 95%CI 1.63-1.09) and those of Han ethnicity (OR = 2.23, 95%CI 1.66-5.02) were more likely to report ART initiation. Having a local Hukou was not associated with ART initiation in this sample (OR = 1.21, 95%CI 0.97-1.52). In the block of enabling/disabling factors, staying married (OR = 0.59, 95%CI 0.42-0.81); earning over 3,000RMB (about US$450 in 2016) a month (OR 0.68, 95%CI 0.54-0.86); being retired (OR = 0.33, 95%CI 0.15-0.75); and having a higher depression score (OR = 0.98, 95%CI 0.96-0.99) were all associated with a lower probability of ART initiation. As for the need variance block, only condomless anal sex in the past 12 months was associated with lower initiation of ART (OR = 0.40, 95%CI 0.32-0.50).
The model prediction performance increased incrementally with each block added, according to AUC with LOO-CV (see Figure 1), and other fit statistics (Table 2). The analyses indicated that adding the need factors block improved the model more than adding the enabling/ disabling factors.

DISCUSSION
To our knowledge, this is the first study that used Andersen’s health service utilization model to examine the correlates of ART initiation among HIV-positive MSM in China. Less than half (46.5%) of the participants in this study had initiated ART, even though the national ART coverage among PLWH has increased from 67% in 2015 to 80.4% in 2017.35 This suggests that more targeted interventions are needed to increase ART coverage in HIV-positive MSM populations. The ART coverage rate (60.3%) in a study on a group of MSM in Chengdu and Hangzhou16 is higher than what was found in our study. While the demographic characteristics of our participants are comparable to those in that study, the difference in data collection time frame might explain lower ART initiation rate in our study.16 China only started providing free ART to PLWH regardless of CD4 levels in June 2016.16 In Yang’s study.16 data were collected from February to November 2016, while our data were collected from 2014 to 2016.16 Given that, participants with CD4 levels higher than 500 cells/mm3 enrolled in our study (about 23%) before the new policy was implemented were not eligible for free HIV treatment.
Overall, we found that the strongest predictors of ART initiation in this study were from the predisposing factors and the enabling/disabling factors. This is partially consistent with the prediction of Andersen’s model that more serious medical problems are more strongly associated with demographic characteristics. Within the block of predisposing factors, older age and Han ethnicity are associated with ART initiation. This is consistent with previous studies on MSM done in China.16,24 Although Liu et al.24 found having local Hukou predicts ART initiation, Hukou is not a significant predictor of ART initiation in this study. The current policy in China requires a local Hukou, temporary residential permit, or a permanent residency to receive free ART.36 Therefore, some participants in our study who did not have local Hukou might have residential permits and thus are also able to access ART. Nevertheless, the treatment eligibility based on residential status results in a structural barrier that may discourage some HIV-positive patients to seek treatment due to perceived ineligibility.16 The policymakers could consider modifying the policies to reduce barriers and increase access to HIV care.
As for enabling/disabling factors, we found that currently married, earning a monthly income of 3000 RMB or above, retirement, and higher depression score are associated with a lower probability of ART initiation. A marital relationship could be considered a source of social support, which was found to be associated with greater initiation of ART initiation in other regions.27 However, same-sex marriage has not been legalized in China, which means that the married participants in this study have female spouses. A study estimated that about 70% of MSM in China eventually marry women and have children due to social pressure. Therefore, the need for concealing one’s sexual orientation in marriage results in a stressful rather than supportive relationship.37 Retirement usually means reduced financial resources (e.g., insurance) which could explain the negative association between retirement and ART initiation.
The association between depression symptoms and ART initiation is consistent with previous literature25 and has been reported to contribute to delays in ART initiation in PLWH.38–40 Depression may reduce the perceived effectiveness of HIV treatment, decrease personal motivation, and thus hinders treatment initiation.41–43 However, the findings reported by 29 are the opposite of what we found. The authors of that study explained that severe depression is usually associated with lower CD4 counts, which serves as “an important indicator for ART initiation”.44 Moreover, participants in Tao’s study also received counseling for their depression and anxiety, which might contribute to the early ART initiation for these participants. Depression is common among people who are diagnosed with HIV29 but currently receives little clinical attention in China due to stigma, inadequate insurance coverage, and limited training on assessing mental health illness among providers.45–47 The stigma associated with being HIV-positive and a MSM further compounded the problem.48 More studies are needed to examine the effect of mental disorders on treatment initiation to provide recommendations for intervention and policy.
Within the need factors, unprotected anal sex in the past 12 months was associated with a lower probability of ART initiation. This association might be due to a third variable. For example, some individuals might generally not engage in health promotion activities including using condoms and initiating ART. This is consistent with previous findings that individuals who are not health conscious and have low HIV awareness are less likely to practice safe sex and initiation ART.25,49 It is also possible that participants in this study who initiated ART were subsequently less likely to engage in sexual risk behavior, which is consistent with previous literature.50 Due to the cross-sectional nature of the current study, we could not disentangle the temporal relationship between these two variables. More studies should be done to examine this finding.
While this is one of the few studies that examined the correlates of ART initiation among MSM in China, it has some limitations. First, Andersen’s Health service Utilization model suggests that enabling/disabling factors include individual, family, and community resources. This study focuses on individual resources because family and community recourse related variables are not available in the dataset. Future studies should examine the effects of family and community resources on ART initiation. Second, the participants were recruited by snowball sampling without a sampling frame. Therefore, the results from this study are unlikely to be generalizable to all HIV positive MSM in China. Third, this study used cross-sectional survey data, which limited our ability to draw causal inferences from the analyses. Future studies could design studies to test the effects of manipulatable variables (e.g., depression) on ART initiation. Last, our survey did not include fear of side effects as a barrier for ART initiation. The free ART from the government only covers a certain number of medications. While free ART offered by the government improved access to treatment, the side effects often deter people from initiating treatment.51 Patients can opt for medications that cause fewer adverse reactions, but they are more expensive and require self-pay. This presents as a financial barrier for people who cannot afford the medication cost. The Chinese government should include a wide range of medications into the free care plan so that patients are less likely to defer treatment due to concerns around side effects.
CONCLUSIONS
Although ART initiation rates have been increasing steadily in the past decade, this study found the ART initiation rate in this MSM sample is lower than the national level. This is the first study that uses Andersen’s Health Service Utilization model to conceptualize the correlates of ART initiation among MSM in China. The demographic variables and enabling/disabling factors are most predictive of ART initiation in this sample. Depression is a disabling factor towards ART initiation, while sexual risk behavior might serve as an indicator of lack of ART initiation. More research is needed to examine whether changes at the policy level could reduce structural barriers to treatment and whether providing mental health counseling for HIV-positive patients could be beneficial for ART initiation.
Acknowledgments
The authors thank Dr. Ali Shojaie for his feedback on the analysis.
Funding
This study was funded by Natural Science Foundation of China (grant #: 81361120385) and NIAID/NIH (grant #: R01AI06715), and partially supported by Shanghai Municipal Health and Family Planning Commission (grant #: GWTD2015S05).
Authorship contributions
L.W. conceptualized research question using the dataset, analyzed the data, written up the manuscript. N.H. and F.W. designed the research project and collected data. C.H., J.S., C.L., L.C., and F.W. reviewed and edited the manuscript.
Competing interest
The authors declare that they have no competing interests (includes financial and non-financial). The authors completed the Unified Competing Interest form at http://www.icmje.org/disclosure-of-interest/ (available upon request from the corresponding author) and declare no conflicts of interest.
Correspondence to:
Liying Wang, M.S.
Department of Psychology
University of Washington
3821 W Stevens Way NE
Seattle, WA 98105.
[email protected]; 6507393370.