Maternal mortality is a global health priority. An estimated 295,000 deaths occur annually due to causes related to pregnancy and childbirth.1 While substantial progress was made from the 1990s to 2015, with maternal deaths decreasing 44% from 385 to 216 deaths per 100,000 live births, the world failed to meet the Millennial Development Goal (MDG) targets of reducing deaths by 75% by 2015.2 Large disparities exist between and across regions and countries, with 99% of maternal deaths occurring in developing countries.2 The majority of maternal deaths are preventable if a woman has skilled care at and around the time of birth.3 As such, the World Health Organization recommends that all women receive care with skilled health personnel for childbirth.4,5
Developing countries’ efforts to increase births attended by skilled health personnel have aimed at reducing barriers to access by measures, such as increasing the provision of skilled health personnel and implementing low or no cost maternal health services.6,7 Despite these efforts, global maternal rates of births attended by skilled personnel remain suboptimal, particularly in rural areas where only two-thirds of women utilise skilled health personnel for delivery, considerably lower than urban rates of nearly 90%.8
New targets set for 2016-2030 with the United Nations Sustainable Development Goals (SDG) call for a global rate of fewer than 70 maternal deaths per 100,000 live births by 2030 (SDG 3.1).2 Emphasising the importance of women receiving skilled delivery care in reducing maternal mortality, SDG 3.1.2 measures the proportion of births attended by skilled health personnel.8
Lack of utilisation of health services among rural women has been a critical issue in maternal deaths,6,9 making increasing demand and utilisation for essential maternal health services one of the most significant challenges in global health today.6 Key to increasing rural uptake of skilled health personnel for delivery is understanding variations in care-seeking behaviour and why some rural women uptake skilled health personnel for delivery while others do not, given they likely face similar barriers.
Ghana context
Ghana currently has a maternal mortality rate of 310 deaths per 100,000 live births10 and, like many other developing countries, is presently not on track to meet the SDG of no more than 70 deaths per 100,000 live births by 2030.1,11 Ghana is a country that has taken significant measures to reduce barriers to maternal health services through the expansion of health services to rural areas through the Community-Based Health Planning and Services (CHPS) program, initiated in 1999,12 and by offering free enrollment in the National Health Insurance Scheme (NHIS) since 2008, which provides free coverage of maternal health services, including childbirth.13,14 While most rural women enrol in maternal health insurance coverage, and 97% attend antenatal care visits, nearly one-third (31%) of women still do not utilise skilled health personnel for childbirth.15
Research needed
Research is limited in applying theoretical models to understand maternal behaviour to utilise skilled health personnel for childbirth. This study’s contribution is applying a theoretical model to understand rural maternal behaviour better, detect differences between rural women who do and do not uptake skilled health personnel for delivery, and identify targets for interventions to increase rural women’s utilisation of skilled health personnel delivery.
Health Belief Model
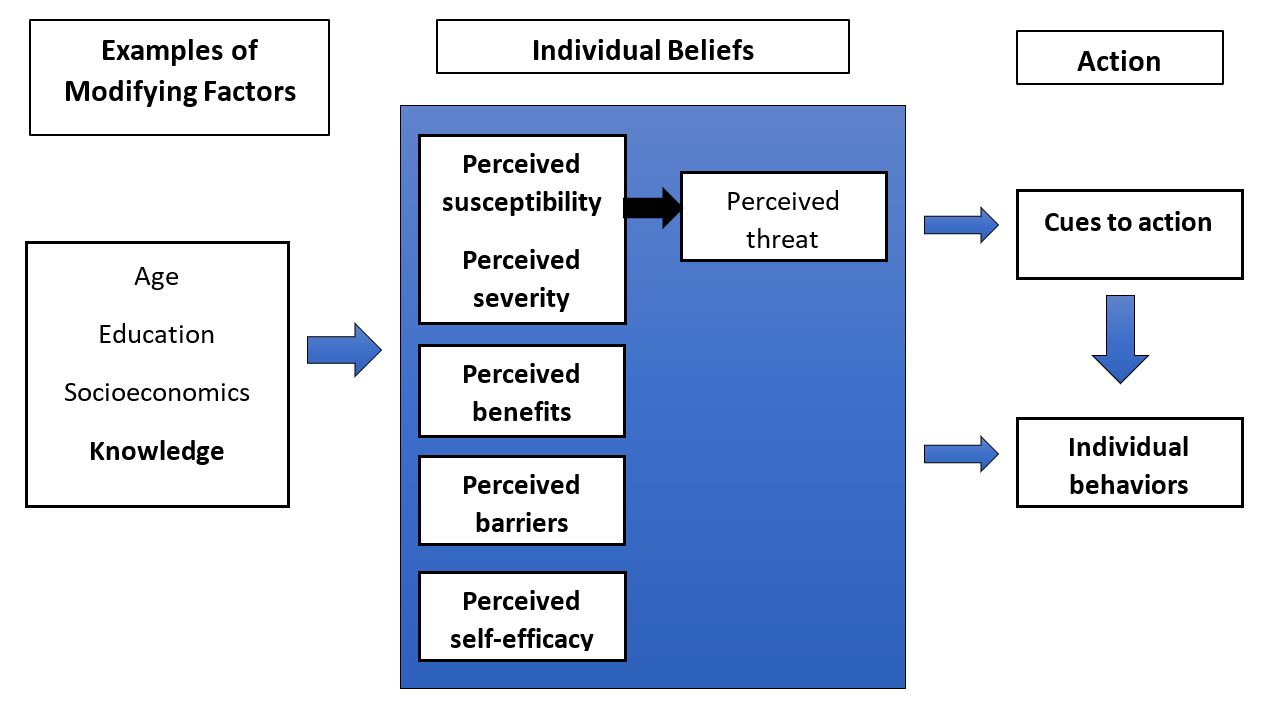
The Health Belief Model (HBM) is one of the most widely used theoretical frameworks to understand and predict health behaviours. Social scientists initially developed HBM during the 1950s to understand why people failed to take up behaviours to detect or prevent diseases, such as screening tests.16 The HBM asserts that individual behaviour is based on 1) desire to either avoid or recover from an illness condition for which an individual believes they are susceptible, and 2) belief that taking a particular action will prevent or mitigate the situation.17 Whether an individual embraces a health behaviour is related to perceptions of whether benefits outweigh barriers to taking the necessary action, providing barriers are not so powerful to prevent action.16,17
Core components of the HBM (see Figure 1) include perceptions of susceptibility and severity to an illness condition, benefits and barriers to taking action, cues to action to set in motion the decision to act, and self-efficacy, which refers to an individual’s confidence to perform a behaviour successfully leading to an outcome.16 Additionally, the HBM assumes factors such as socioeconomic status and educational level can alter perceptions of susceptibility, severity, benefits, and barriers, thereby indirectly influencing behaviour.16

METHODS
Study design
We used a qualitative descriptive phenomenology approach to explore differences among rural women to uptake skilled delivery care. The descriptive process uses individual in-depth interviews to explore individual experiences, identifying poorly understood aspects of practices related to a phenomenon of interest.18 The underlying worldview in this research is pragmatism since this philosophy uses a practical approach and allows for more than one perspective of participants’ experiences.18 The HBM was employed as the theoretical framework to explore maternal behaviour differences since the HBM has been used extensively to understand health behaviours better.16 The study was approved by the Ethics Review Committee from Ensign College of Public Health in Ghana. Additionally, this qualitative study was planned to inform a quantitative study on the same topic.
Research setting
The research took place in the Eastern Region of Ghana, a primarily rural region, with nearly two-thirds of the population of 2,106,696 residing in rural areas.19 The primary industry is agriculture, followed by wholesale or retail trade.19 The most common type of home is constructed of mud entailing one to two rooms.19 The Region is divided into 26 administrative districts. Three districts were selected to be included in our study based on proximity and accessibility to researchers: Lower Manya Krobo, Yilo Krobo, and Asuogyaman Districts. Six communities, two rural communities from each of the three districts, were purposively selected based on input from Municipal Health Directors. Interviews were conducted at participants’ homes in December 2019. Two female researchers and the participant were present during the interviews. Other individuals initially present were respectfully asked to allow privacy due to sensitive discussions on maternal health issues.
Study population
The target population was rural Ghanaian women aged 15 to 49 who had delivered a child in the past two years and are residents of the participatory community. Participants were purposively selected for in-depth face to face interviews. Nurses at the CHPS, informed of the study in advance, directed researchers to areas where women resided who had and had not delivered with skilled health personnel. When no CHPS nurse was available, researchers asked older women in the community where women meeting the study criteria resided. Participation was high, with only two women declining to be interviewed due to prior commitments.
Data collection
Data were collected through 24 individual in-depth single interviews, 12 mothers who did and 12 mothers who did not utilise skilled health personnel for delivery. Each face-to-face interview lasted approximately 45 minutes. The authors developed a semi-structured guide based on questions generated from a literature review. Women were asked to describe perceptions related to their most recent pregnancy and delivery experience with open-ended questions. The guide was field-tested and revised (JN, RA, YA) prior to data collection. The three female researchers (JN, RA, YA) were knowledgeable in reproductive health issues and had previous training and experience in qualitative interview techniques and qualitative research procedures.
The research purpose was explained to participants, and informed consent was obtained prior to interviews through a signature or thumbprint. Researchers had no preexisting relationship with participants. All interviews were conducted in the local languages (Krobo, Twi, or Ewe) predominantly spoken in the study area by one researcher (RA) to maintain interview quality and consistency, while a second researcher (JN) took field notes. Saturation was achieved, which was the point at which interviews did not reveal new themes or information. Interviews were audio-recorded and later translated into English by a researcher (RA), based on topic and question, capturing the essence of what participants said, translating representative quotes verbatim. A second researcher (JN) recorded responses. A third researcher (YA) independently listened to recordings and reviewed transcripts to ensure accuracy. Where differences occurred, two researchers (RA, YA) discussed until reaching consensus.
Data analysis
Data were analysed following data analysis and representation for phenomenology research in Creswell & Poth.18 First, after researchers (JN, RA, YA) reviewed all responses, a researcher (JN) created data files, compiling participant responses, and field notes from each topic and question. Second, researchers (JN, RA, YA) read through texts several times, making notes and coding text lines broadly, then iteratively modifying as patterns emerged. Third, themes were generated within the context of the HBM framework common to both groups and differentiated women based on the utilisation of skilled delivery care. Fourth, explanatory quotes were highlighted, revealing insight into women’s individual experiences and beliefs. Fifth, descriptions were developed that represented everyday, and differentiating experiences among women who did vs did not utilise skilled health personnel for delivery. Data were entered into Excel by one researcher (JN) and reviewed by two researchers (RA, YA). Results were reported following the guidance of the Standards for Reporting Qualitative Research (SRQR) checklist.20
RESULTS
Characteristics of participants
The sample consisted of 24 participants, 12 women who utilised skilled health personnel for their last childbirth, and 12 who did not. Demographic characteristics are presented in Table 1. Participants were aged 16-36 years (median 25), and most were married or cohabitating. Most women had either a primary or middle school education and were employed in trading or farming. Parity ranged between 1-6 children (median: 3).
Self-reported obstetric characteristics of participants are presented in Table 2. Nearly all women possessed health insurance with their last pregnancy and attended antenatal visits. The number of four or more antenatal visits was selected based on the recent Ghana Maternal Health Survey.10 Almost half perceived that they had ever had a pregnancy or birth complication. The primary mode of transportation to the health facility was walking, and travel time ranged from under 30-minutes to considerably longer times of one to two hours.
Findings related to the Health Belief Model
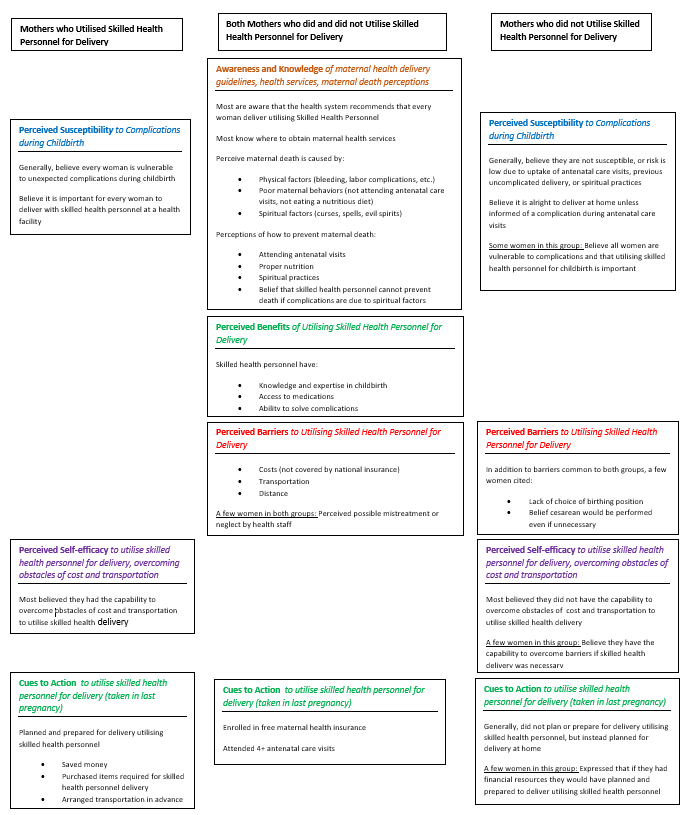
A summary of the main findings is provided in Table 3 and Figure 2. Based on the HBM framework, essential differences emerged between women who did and did not utilise skilled delivery care in the following areas: perceived susceptibility, perceived self-efficacy, and cues to action. Common themes emerged among both groups of women of perceptions of benefits and barriers to skilled delivery care.

Modifying factors
Knowledge and awareness
Women were asked questions about knowledge and awareness of recommended guidelines to uptake skilled health personnel for delivery, where to obtain maternal health services, and causes/prevention of maternal death.
Most women, regardless of whether they delivered with skilled health personnel or not, were aware of recommended guidelines to deliver using skilled health personnel, responding that Ghana Health Services recommends that 'you should go to the hospital or [health centre] and have a nurse or midwife deliver your baby. However, a couple of women were not aware of the recommended guideline that all women should utilise skilled health personnel for delivery. Additionally, nearly all women knew where to obtain maternal health services. Women from both groups generally believed that maternal death could be caused by physical, behavioural, and spiritual factors. Perceived physical causes include examples such as bleeding, disease, and difficult labour. Perceptions of maternal behavioural causes include examples such as lack of uptake of recommended antenatal healthcare visits and poor diet.
Beliefs of spiritual causes include spells, curses, and evil ancestral spirits. Women generally believed measures to prevent maternal death included attending antenatal visits, proper nutrition, or spiritual practices. However, women thought skilled health personnel could do nothing to prevent or treat childbirth complications related to spiritual factors as only a religious leader such as the fetish priest or pastor might be able to intervene if discovered soon enough. There were no major differences observed between groups.
“Disease, not eating good food or some people who hate people can cast a spell on a pregnant woman [to die in childbirth]. Pregnant women should go to antenatal [visits], eat well, and go to church and pray a lot to offset [evil] against them to have a safe delivery.”-Skilled health personnel delivery, participant 11
“It might be that it is the person’s destiny. People cast spells to intentionally kill pregnant women to hurt the family. The hospital can’t help you if someone casts a spell on you. You need to go the fetish priest.” -Non-skilled delivery, participant 20
Individual beliefs
Perceived susceptibility, severity, and threat
Women were asked questions about their belief in personal susceptibility to childbirth complications and the importance of using skilled health personnel for childbirth delivery. A question exploring beliefs of severity was excluded after field-testing the interview guide and consulting local researchers. We were informed that women often hold superstitions; it is ‘bad luck’ to discuss adverse outcomes such as maternal death when implicating self.
Generally, women who delivered with skilled health personnel and a few who did not deliver utilising skilled health personnel indicated they believed every woman is susceptible to complications and that it is essential for every woman to deliver with skilled health personnel.
“Yes, every woman can have it–complications can occur even if she does not expect it.” -Skilled health personnel delivery, participant 9
“Yes, it [skilled health personnel delivery] is important for all women. They have medications that can help you, if needed .”-Skilled health personnel delivery, participant 14
In contrast, most women who had not delivered with skilled health personnel did not believe they were susceptible to complications related to childbirth or that the risk was very low due to antenatal healthcare visits, previous uncomplicated delivery, or spiritual practices. Regarding the importance of utilising skilled health personnel for delivery, women who did not use skilled health personnel for delivery initially responded “yes” although a few responded “no.” However, upon probing, we found that most women who did not utilise skilled health personnel for delivery believed it is only important if women are told at antenatal care visits that they have a complication that requires hospital delivery.
“If you go to antenatal, they can see all complications and solve them. Women who don’t go to antenatal care, they don’t know that they have complications, so when they deliver their baby in the house, they bleed, and they die.” -Non-skilled delivery, participant 12
“It is [a complication] possible but less likely, since I haven’t had any complications with my other deliveries.” -Nonskilled delivery, participant 23
“No [I am not susceptible to complications], I fortify myself spiritually.”-Nonskilled Delivery, participant 18
“If you don’t have any complications then you can deliver in the house.” -Nonskilled delivery, participant 19
Additionally, some women who did not utilise skilled health personnel believed it was necessary only for those who did not fortify themselves spiritually through spiritual practices.
“Only those who don’t fortify themselves spiritually go to the hospital.” -Nonskilled delivery, participant 16
Perceived benefits
Women were asked if they believe there are benefits to delivery with skilled health personnel.
Most women responded that they believed there were benefits to delivering with skilled health personnel, including that skilled health personnel had knowledge and expertise in childbirth, the ability to solve complications, and give medications, intravenous fluids, and blood transfusions if necessary. There were no major differences observed between groups.
“Nurses can give you medications and solve complications.”- Skilled health personnel delivery, participant 9
“The nurses have a lot of knowledge, and they can give you IV fluids when you need it or transfuse you if needed.” Non-skilled delivery, participant 7
Perceived barriers
Women were asked questions regarding the main barriers for women to deliver with skilled health personnel.
Common barriers indicated by both women who had and had not delivered utilising skilled health personnel include cost, transportation, and distance. Additionally, perceived possible mistreatment or neglect by health staff was a barrier mentioned by some women who had and had not delivered with skilled health personnel.
The most common barrier mentioned was associated costs of delivering with skilled health personnel not covered by maternal health insurance. Costs mentioned include a list of required items by the health system a woman should bring for skilled delivery care, food, and transportation. Women also reported transportation and distance as barriers due to the difficulty of arranging transport, particularly at night and the mode, which is usually a motorcycle.
“If you have to deliver in the hospital, they can give you a long list of things you must buy like towels, powder, bleach. Some women don’t have the money, but others also have money but can’t go because if the labor falls in the night, you can’t get a lorry.” -Non-skilled delivery, participant 15
Perceptions of potential mistreatment during childbirth included forms of physical, verbal, or neglect mistreatment by health staff.
“In the hospital, women are mistreated and yelled at, and treated with a lot of impatience.” -Non -skilled delivery, participant 3
“Some midwives at the CHPS treat you well and some don’t. They can neglect you to develop complications.” -Non-skilled Delivery, participant 12
“The nurses sometimes cane women when they are screaming in labor.” -Skilled health personnel delivery, participant 5
A few women who did not utilise skilled health personnel for delivery cited barriers of lack of birth position options or belief that health personnel would perform an unnecessary cesarean section.
“I can’t deliver lying on my back as the nurses require.” -Non-skilled delivery, participant 23
“If you go to deliver in the hospital, even if it is not necessary, they will do a cesarean.” -Non-skilled delivery, participant 18
Perceived self-efficacy
We asked women to rate themselves in their confidence to adhere to recommendations to uptake skilled health personnel delivery, including overcoming obstacles of cost and transportation.
Most women who utilised skilled health personnel delivery reported ‘high’ self-efficacy to overcome cost and transportation obstacles to obtain skilled health personnel delivery. In comparison, most women in the nonskilled delivery group reported ‘low’ self-efficacy due to the cost of items or lack of transportation. The few women reporting ‘high’ self-efficacy indicated they could overcome obstacles to uptake skilled health personnel delivery if necessary.
Action
Cues to action
Women were asked questions about their actions taken related to birth preparedness.
Most women who delivered with skilled health personnel prepared for birth in advance. Women reported husbands and themselves saving money, buying items on the list required for delivery, husbands arranging transportation in advance, and planning other children’s care.
“My husband saved money and gave it to me. Furthermore, I also saved money. I bought the items on the list, and my husband made arrangements for transportation for me in advance” -Skilled health personnel delivery, participant 1
By comparison, most women who did not utilise skilled health personnel delivery did not take any actions to prepare for birth using skilled health personnel. A few women indicated they would have prepared for the delivery utilising skilled health personnel if not for the lack of financial resources.
“No [I did not prepare for skilled health personnel delivery], I knew I could deliver at home.” -Non-skilled delivery, participant 23
“I didn’t have the money to buy the items on the list required to be bought. If I had money to buy the items, I would go.” -Non-skilled delivery, participant 12
DISCUSSION
This study provides insight using a theoretical model to reveal differences between rural women who utilise skilled health personnel for childbirth and those who do not. Our research shows that rural women differed on the HBM constructs of perceived susceptibility for complications during childbirth, perceived self-efficacy to overcome barriers for skilled health personnel delivery, and cues to the action of birth preparedness for skilled health delivery. Women in both groups generally agreed on common benefits of skilled health personnel expertise, medications, and the ability to solve complications and agreed on barriers of cost, distance, transportation, and mistreatment by some health staff.
The critical role of knowledge and susceptibility
A key difference between women who did and did not utilise skilled health personnel for delivery was perceived susceptibility to complications and, subsequently, the importance of skilled health personnel delivery. Our research suggests that knowledge of maternal risk may alter perceptions of vulnerability. We found that women who did not believe they were susceptible to complications lacked knowledge of childbirth risk, overly trusted antenatal care visits to detect complications, thought skilled delivery unnecessary unless informed during antenatal visits of a complication, or believed spiritual rituals practised during pregnancy would ensure safe delivery. These findings agree with other studies that knowledge is an important factor in the uptake of skilled delivery care, often referred to as lack of health literacy, low perceived need, or lack of seriousness.21–25
This study differs in that it identifies specific components of maternal knowledge as influencing perceptions of “susceptibility,” underscoring the importance of maternal understanding of risk. The essential course of action is utilising skilled delivery care, irrespective of other actions related to individual beliefs. It also adds insight to the perplexing pattern as to why some rural women adhere to recommended guidelines to uptake antenatal care but not skilled delivery care, as seen in Ghana26 and other countries.27,28 Similarly, Wallace found that rural women and their husbands may perceive antenatal care assuring a healthy pregnancy means everything is fine. Therefore, it is unnecessary to seek skilled health services for labour and delivery.29
While knowledge is essential, an intervention aimed at singularly increasing maternal knowledge is likely to have limited impact in increasing births attended by skilled health personnel21,30 since decision making for childbirth is often determined by or influenced by others.29,31 A more effective approach would likely be to increase community knowledge, including influencers such as community and traditional leaders, religious leaders, elders, men, and other women who women may rely on for social, spiritual, or financial support.23
Weighing benefits and barriers
We found that women from both groups generally agreed on common perceived benefits and barriers. Our findings suggest that maternal risk knowledge may affect the weights of perceived benefits and barriers of skilled health personnel delivery.16 This finding may provide insight into why some women seek skilled health personnel delivery while others do not in the same setting facing similar barriers. Suppose women and their families are educated to know that all women are susceptible to unanticipated complications during childbirth that may result in the mother’s death unless treated promptly by skilled health personnel. In that case, they may be willing to take actions to overcome barriers to minimise risk, such as allocating financial resources for the benefit of skilled health personnel delivery, while those who do not know maternal risk may be less willing.
Barriers of cost and access persist
Our study found that cost and access barriers too substantial to overcome persist for some rural women, even though Ghana provides free coverage of maternal health services, including delivery with skilled health personnel,14 and expanded maternal health services to rural areas through the CHPS program.12 Women cited barriers of lack of money for associated costs of skilled health personnel delivery, such as the cost of the items required by GHS and transportation, a finding corroborated in a recent study by Boah.32 These findings suggest that the least advantaged women may be too poor to access skilled health personnel delivery.
Barriers beyond cost and access
We found that while women valued skilled health personnel expertise and medical interventions, the possibility of mistreatment during labour and childbirth by some health staff was a barrier cited by both groups of women. Possible mistreatment by health staff was a barrier that influenced women’s choice of nonskilled delivery over skilled delivery care, exemplified by the following quotes, “Some midwives at the CHPS treat you well and some don’t. They can neglect you to develop complications” (nonskilled delivery, participant 12) and “In the hospital, women are mistreated and yelled at, and treated with a lot of impatience” (nonskilled delivery, participant 3). Other studies have reported mistreatment of women during childbirth is common.33,34 Additionally, the lack of birthing position options and fear of unnecessary cesarean were barriers for a few women. These findings provide insight into why some women, even when cost and access barriers have been addressed, do not uptake skilled delivery care. A health system intervention of training healthcare workers in interpersonal relations may be a feasible approach to increasing the respectful treatment of women.
Implications
Improving births attended by skilled health personnel is a multifaceted issue and may require a combination of efforts at the community, health system, and national levels, depending on the context. Interventions should aim to increase community knowledge of maternal risk during childbirth, the importance of skilled health personnel delivery, overcoming barriers, and birth preparedness, as decision making occurs in the context of the community and women often need support from men and others to uptake skilled health personnel delivery. Previous research has shown that community-based interventions may be effective at increasing maternal utilisation of skilled health personnel for delivery.35–37
This research points to the health system’s tremendous opportunity to improve maternal health outcomes at several different leverage points. First, there is an opportunity to engage communities to increase community knowledge of maternal risk and overcome barriers to access skilled health personnel delivery. Second, antenatal care visits provide an opportunity to reinforce messaging of the importance of delivery with skilled health personnel, to educate women on maternal health, and work with women and their partners to increase birth preparedness. Third, there is an opportunity for the health system to improve women’s childbirth experience by training health staff on interpersonal skills and implementing policies that promote a comfortable and supportive environment for women during childbirth.
At the national level, pro-equitable policies should be established, providing pathways to overcome barriers to access skilled health personnel delivery care for the least advantaged women, including subsidising the cost of supplies women are required to bring to the health facility for childbirth. Finally, countries must plan strategically to improve education levels for both girls and boys and reduce poverty in rural populations by increasing economic opportunities since both are strong determinants of skilled delivery care uptake. Further research should focus on developing community-based interventions to increase birth preparedness, approaches to improving health staff treatment of women, and reducing inequities to ensure all women, including the least advantaged, benefit from skilled health personnel delivery.
Strengths and limitations
To our knowledge, this is the first study to identify key differences between groups of rural women residing in the same setting who did and did not utilise skilled health personnel delivery using a theory-based model. The study identifies the constructs of perceived risk for complications during childbirth, perceived self-efficacy to overcome barriers of cost and transportation, and cues to action of planning and preparing in advance for delivery utilising skilled health personnel as key differences and important factors of whether a woman will utilise skilled health personnel for delivery.
Furthermore, this research provides valuable insight for policy makers and program planners into potential leverage areas for creating pro-equitable policies and designing future interventions. Despite strengths of the research, there are some limitations. Although comparison of groups is beneficial to identify important differences between and within groups, there is currently no standardised methodology for making comparison in qualitative research.38 We cannot rule out the possibility of selection and recall bias. It is possible participants may not have accurately recalled information, or that they did not fully share information, or that women may have selectively rejected participation since maternal attitudes and experiences may be a sensitive topic for women. Additionally, we faced limitations inherent in conducting a collaborative study in a low-resource setting, including time constraints which is why researchers coded and generated themes together arriving at consensus, rather than independently-although we made efforts to limit bias by reviewing the data texts and themes several times. Furthermore, findings from this study may be specific to this area and not transferrable. There is a need for confirmation of results in future research including through larger quantitative studies to measure effect and impact.
CONCLUSIONS
Application of the Health Belief Model reveals both commonalities and key differences in perceptions and behaviours between groups of women residing in the same rural setting who did and did not deliver utilising skilled health personnel, providing valuable insight for policymakers, the health system, and program managers. Policies and interventions should focus on increasing maternal knowledge and perceptions of risk, the importance of skilled health delivery, birth preparedness, and overcoming cost and access barriers that still persist for some rural women.
The main similarities between both groups of women included that both were aware that the health system recommends women deliver utilising skilled health personnel. Both perceived that main barriers to skilled health delivery included cost, transportation, and distance while the main benefits were that skilled health personnel have childbirth expertise and knowledge, access to medications, and the ability to solve complications. Key differences between groups of women included perceived risk of experiencing complications during childbirth and importance of delivering with skilled health personnel, perceived self-efficacy to overcome barriers, and birth preparedness–although some women in the group not utilising skilled health personnel had risk perceptions similar to those who utilised skilled health delivery, but believed the barriers they faced as too substantial to overcome for them to utilise skilled health personnel for delivery. Thus, this research also provides insight into why maternal rural utilisation rates of skilled health personnel for delivery are suboptimal despite commendable country efforts to reduce cost and access barriers.
Acknowledgements
We express gratitude to Ensign Global College administration and staff for logistic support and to Ghana Health Services, the District Health Directors, and health personnel for their assistance in selecting the study communities and coordinating the research with communities. Additionally, we wish to thank Health 2 Go for coordination efforts, recruiting our research team in Ghana, and for their support in carrying out this international study. We thank our entire research team for their dedication and commitment. Finally, we wish to thank the communities and women who participated in the study from the Eastern Region in Ghana.
Funding
This study was funded by Cast a Pebble Foundation.
Authorship contributions
Study design: JN, SA; data collection and analysis: JN, RA, YA; writing: JN; review and revision of study design, manuscript drafts, and approval of the final manuscript: JN, TD, LG, SB, SM, and SA.
Competing interests
The authors completed the Unified Competing Interest form at http://www.icmje.org/disclosure-of-interest/ (available upon request from the corresponding author) and declare no conflicts of interest.
Correspondence to:
Jeanette R Nelson, PhD
Center for Business, Health, and Prosperity,
David Eccles School of Business
University of Utah, Salt Lake City, Utah, USA
[email protected]