Human Immunodeficiency virus (HIV) is a threat to global public health with almost 40 million people living with the virus worldwide.1 With the advent and scale up of anti-retroviral therapy (ART), HIV has become a manageable chronic condition with life expectancies of people living with HIV (PLWH) comparable to those living with other chronic conditions.2 This increasing longevity among PLWH, and the premature aging effect of HIV is increasing the prevalence of non-communicable disease (NCD) comorbidities such as Diabetes Mellitus Type 2 (DM) and hypertension (HTN).3,4 High rates of NCDs among PLWH have been reported in high HIV-burden, and low-resource settings5–7 placing strain on the health systems in these settings which are ill-equipped to cope with the inherent complexity of multi-morbid patients.8
The growing dual burden of HIV and NCD syndemics (epidemics occurring in the same population at the same time) has necessitated exploration of integration of HIV and NCD care in primary health care to leverage existing HIV care infrastructure for NCD care in high HIV-burden settings.9,10 Integrated care has been defined as the coordination, co-location, or simultaneous delivery of HIV and NCD services to patients who need it, when they need it.11 Three models of integrating HIV and NCD care in primary health care have been previously described12 as follows: model 1: Integration of NCD screening and treatment services into established HIV centres; model 2: Integration of HIV screening and treatment services into established NCD centres; and model 3: simultaneous integration of HIV and NCD services at integrated health centres. As these models do not pre-suppose multi-morbidity, a fourth model proposed by Njuguna et al9 includes integrated HIV and NCD care for PLWH with comorbid DM or HTN or both, which may be delivered at group (using medical adherence clubs-MACs) or individual levels.
Despite increasing evidence to suggest feasibility of integrating HIV and NCD care, little is known about the effect of such integration on long-term patient outcomes.9,12,13 These long-term outcomes include, but are not limited to, medication adherence, retention in care, loss to follow up, HIV viral load suppression / improvement in CD4 counts and markers of NCD control. It is not known if integration of HIV and NCD care in primary health care improves or at least maintains these outcomes among PLWH with multimorbidity receiving integrated HIV and NCD care. Such evidence is needed to inform program managers and health policy makers in order to adopt, implement and scale up integrated HIV and NCD care for multi-morbid patients.
This review aims to identify literature that describes the effect of integrating HIV and NCD care on long-term patient outcomes.
METHODS
We conducted a scoping review14,15 of literature that described the effect of integrating HIV and NCD care on long-term patient outcomes. This typology of literature review has been noted to be appropriate where there is a need to identify and map the amount of literature and studies available on a given topic, or where evidence is emerging but remains unclear.16 Nonetheless, a rigorous and transparent methodology is required. This review followed the Arksey and O’Malley methodological framework for conducting scoping reviews comprising five stages: identifying the research question, identifying relevant studies, study selection, charting the data and collating, summarizing and reporting results.17,18 The reporting of the review findings follows the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) checklist (Figure S1 in online supplementary document).19
Research question
This review was guided by the question 'What are the effects of integrating HIV and NCD care on long-term patient outcomes?’
Search strategy
We conducted a preliminary search of the terms ‘outcomes, effects, successes, effectiveness, impact, integrated HIV, non-communicable disease, chronic disease care’ in PubMed. We then analysed key studies for potential broader search terms and refined the search strategy (Table 1).
Information sources
We performed a literature search, using the final search strategy in PubMed, Scopus, EBSCOhost and Web of Science. We also conducted a manual search of abstracts in the International AIDS Society and the Journal of Acquired Immunodeficiency Syndrome. Grey literature was sourced from Mednar and Open Grey. Bibliographies of relevant papers were also carefully searched to source journal articles unidentified through database searches.
Inclusion criteria
We included articles that reported the following patient outcomes after receiving integrated care for at least 6 months: adherence to medication, retention in care, loss to follow up, viral load measurements, CD4 counts and markers of NCD treatment outcomes including blood pressure (BP) for HTN, and glycosylated haemoglobin (HbA1c) for DM.
Studies were considered for this review if and only if they had enrolled patients older than 18 years of age into integrated care, with a diagnosis of either HIV alone, HIV and HTN or HIV and DM or both. Longitudinal studies, case-control and cross-sectional studies published between 01 January 2000 to 25 September 2019 were included for review. This time frame was selected as there was minimal roll-out of ART programs in low- and middle-income countries, where the burden of HIV is highest, prior to 2000.
Exclusion criteria
Literature not published in English, and that did not report patient outcomes of interest were excluded. Literature reviews were also excluded however, their reference lists were carefully hand -searched for eligible studies that might have been missed in previous steps.
Study selection
Articles retrieved using the search strategy were exported into EndNote version 9 for removal of duplicates. Thereafter, two authors (BG and PO) independently screened articles by title or title and abstract to determine if articles met the eligibility criteria. A full-text screening was then carried out. Ambiguous abstracts were also evaluated via a full text review for eligibility. Disagreements between the two reviewers were resolved through discussion to reach consensus.
Ethical considerations
As reviewed literature were published and available in the public domain, ethical approval was not sought for the purposes of conducting this review.
Data collection and synthesis
The following outcomes were collected and charted from selected articles using a standardized form: Author, place, setting of intervention/study, model of integration utilized, intervention (services integrated), duration of intervention, study population, and outcomes (Table 2). A narrative synthesis of the results was also performed on included studies.
RESULTS
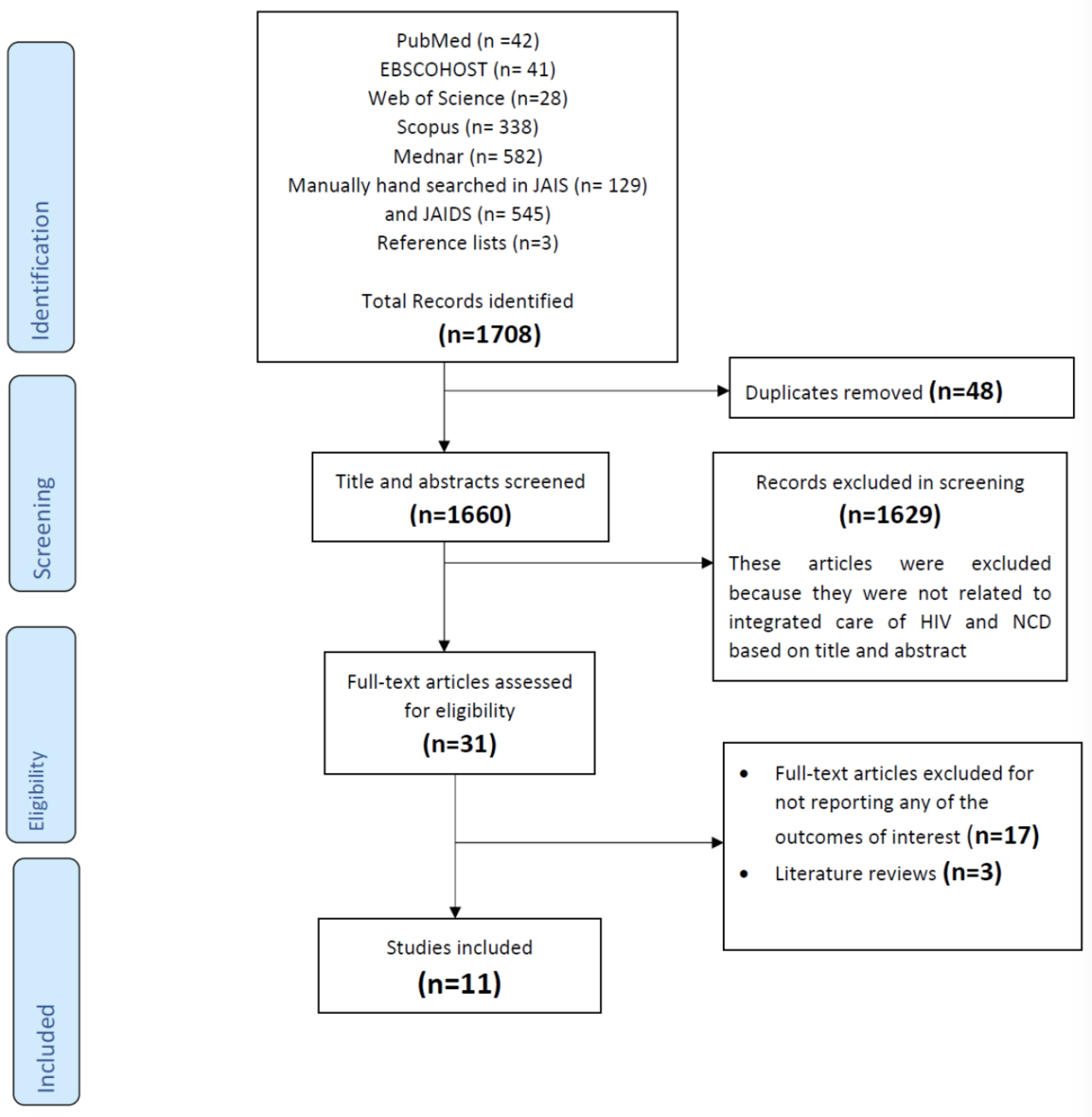
A total of 11 studies were included in the review. Results of our search strategy and process are shown in a PRISMA flow diagram in Figure 1.

Characteristics of included studies
Of the 11 studies included, one was an abstract article20 whereas ten were full text articles.21–30 Eight studies (72.7%) were published later than 2010, the majority of which (n=7) were cohort studies (Table 2). There were no randomized clinical trials identified. Six of the 11 studies were conducted in high-income countries (United States of America and United Kingdom) with five conducted in low- and middle-income high HIV-burden countries (Cambodia, Uganda, Kenya and South Africa) (Table 2).
Models of HIV/NCD integration
Applying the four model categories of integration described by Duffy and Njuguna,9,12 we found that three of the studies that were identified described NCD services integrated into established HIV care centres (model 1), no study reported integration of HIV services into established NCD programs (model 2), five studies described simultaneous integration of HIV and NCD services (model 3), and three studies reported integration of HIV and NCD services among PLWH with multimorbidity (model 4) (Table 2).
Patient outcomes
All studies reported HTN outcomes, 60% reported DM outcomes and 50% reported HIV outcomes. Only one study (Janssens et al24) reported patient outcomes for all three diseases (Table 2). Eight of the 11 studies (72.7%) reported integrated care based in primary care facilities (Table 2).
Patient outcomes by model of integration
Model 1: Integration of NCD services into established HIV care centres
The three studies that reported patient outcomes in the context of integration Model 1 offered NCD screening and treatment services to PLWH in established HIV treatment centres. Prevalence of comorbid HTN among PLWH studied was 26% (USA), 47.8% (Uganda) and 43% (USA) respectively.21–23 Chu et al21 conducted a descriptive cross-sectional study among PLWH with comorbid DM or comorbid HTN. They found that 90% (N= 223) of PLWH with comorbid HTN had controlled BP (BP ≤140/90) and 59% (N= 103) of PLWH and DM had HbA1c < 7%. However, HIV related outcomes (HIV viral suppression or CD4 counts) were not reported. Muddu et al22 compared HIV control rates among PLWH with no comorbidity to PLWH with comorbid HTN. They found that after 1 year of follow up and integrated management, 24.3% of those with comorbid HTN (N= 218) had controlled BP. HIV-related outcomes and retention rates did not differ between PLWH without (viral load (VL) suppressed in 90.2%; retention 71.4% (N=906)) or with comorbid HTN (VL suppressed in 91.6%; retention 65.9% (N=218)) respectively. Myerson et al23 conducted a cross-sectional study in the USA examining control of HIV and HTN among PLWH. They found that among PLWH with comorbid HTN, 57% (N=1840) had controlled BP. In terms of HIV control, 88% of the overall cohort (N= 4278) were on ART and 67% of these had suppressed VL (mean CD4 count 468 cells /mm3).
While these studies reported high rates of control of HIV and comorbid NCDs among patients who received Model 1 of integrated care, they were not designed to show benefit of integrated care compared to non-integrated care. Instead, they merely reported patient outcomes upon integrating NCD screening and treatment services in established HIV programs. Comparison was not made to patient outcomes either before integration or to patient outcomes in non-integrated care.
Model 3: Simultaneous integration of NCD and HIV services
Five studies reported patient outcomes upon simultaneous integration of HIV and NCD care.24–28 Full details on study design, integrated services and results are shown in Table 2. Janssens et al24 reported treatment outcomes from 8850 participants receiving integrated care for 24 months. Of the 8850, 1419 were HIV-uninfected and received care for HTN only, 2638 were HIV-uninfected and received care for DM only and 4793 were PLWH without comorbidities. Among PLWH followed up, 87.7% (N=4793) were retained in care, 9.3% had died and 3% were lost to follow up. Median CD4 counts after attending integrated care for 24 months had risen from 53 to 316 cells/mm3. However, viral suppression rates were not reported. Among people with HTN, 68% (N=1419) had controlled BP. Among people with DM, median HbA1c fell from 11.5% to 8.6% and 57% had HbA1c ≤ 9%. Khabala et al25 conducted a descriptive retrospective cohort study of 1432 HIV-infected and uninfected participants. Of the 1432, 1020 were PLWH, 352 had HTN only and 60 had DM only. Participants were clinically stable for at least 12 months and recruited into MACs of 25-30 patients each. They reported an overall loss to follow up of 3.5% and high rate of compliance to clinical procedures, however, patient outcomes related to control of HIV or NCD were not reported. Kwarisiima et al26 conducted a descriptive cohort study which examined BP control among people with HTN without HIV and PLWH with comorbid HTN in a rural Ugandan community. After screening 34,704 individuals for HIV and HTN, 2071 were found to have HIV. Of the 4355 patients found to have HTN without HIV, 1949 were linked to care at baseline. Of the 2071 PLWH, 199 had comorbid HTN and only 89 were linked to care at baseline. Control of BP among PLWH with HTN (48%) and people with HTN only (46%) did not differ. In this study, the authors noted that NCD care was interrupted with significant hypertension drug stock outs during the study which may have influenced their results. Of note, investigators observed that HIV-infected patients were more likely than uninfected patients to have controlled BP at follow-up visits (adjusted odds ratio, aOR=1.28; 95% confidence interval, CI=1.00–1.77).
Ameh et al27 conducted a controlled interrupted time series study in rural South Africa that compared the likelihood of control of HIV and HTN before and after a pilot implementation of an integrated chronic disease management (ICDM) model by the National Health Department in selected primary health care facilities. A sample of 435 participants were enrolled in intervention facilities using proportionate sampling of which 210 had HTN and 141 were PLWH. Similarly, a sample of 443 participants were enrolled in control facilities, of which 91 had HTN and 282 were PLWH. Results showed that after 30 months of follow up, patients at intervention facilities had a 6% greater likelihood of having CD4 counts >350 compared to control facilities (coefficient=0.057; 95% CI=0.056-0.058; P<0.001). In addition, patients at pilot facilities had a 1.0 % greater likelihood of having patients with controlled BP (coefficient=0.010; 95% CI=0.003-0.016; P=0.002). However viral suppression, retention in care and loss to follow up were not reported.
The fifth, model 3 study was conducted by Edwards et al28 at a primary care centre in an urban informal settlement in Kenya. This was a retrospective descriptive study of 2206 participants that compared BP and diabetes outcomes among PLWH with comorbid HTN (N=200) or DM (N=10), with people with HTN (N=1697) or DM (N=299) only. At 30 months of follow-up, the median systolic blood pressure (SBP) reduced from 151 (Interquartile range, IQR=136-164) mmHg at baseline to 143 (IQR=129-159) mmHg, while diastolic blood pressure (DBP) reduced from 97 (IQR=86-105) mmHg to 85 (IQR=74-95) mmHg for PLWH and comorbid HTN. For people with HTN only, median SBP reduced from 160 (IQR=144–177) mmHg at baseline to 141 (IQR=129–158) mmHg while DBP reduced from 100 (IQR=90–110) mmHg to 87 (IQR=75–95) mmHg. For PLWH and DM, mean HbA1c at last visit was 8.2% (95% CI=7-11%) while among people with DM only HbA1c at last visit was 8.8% (95% CI=7-11%). Neither HbA1c at baseline nor HIV outcomes were reported. In summary, control of HIV and comorbidities was achieved in this model of care despite logistical challenges experienced by some. Majority of studies describing this model of care did not report key HIV-related outcomes such as viral suppression. Only one study (Ameh et al27) compared outcomes among patients who attended integrated care with those who attended non-integrated care. The study showed some evidence that patients who attended IC were more likely to have controlled HIV or NCD compared to non-integrated care patients, suggesting superiority of IC over non-integrated care for control of comorbidities.
Model 4: Integrated care for patients with multimorbidity
Three studies reported patient outcomes among PLWH with comorbid HTN or DM or both (Model 4)20,29,30 (Table 1). Two of these studies (Bury et al29 and Oluwatoyin et al30) undertook descriptive retrospective cohort studies among PLWH with comorbid DM who attended integrated care at HIV specialist clinics in the USA. At the end of follow up, Bury et al29 and Oluwatoyin et al30 reported that 50% and 54% of participants respectively, had achieved ADA(American Diabetes Association) targets for BP and HbA1c at last visit.31 These outcomes were found to be similar to those in studies with HIV-uninfected populations in the same setting. Noble et al20 conducted a cross-sectional review of PLWH with comorbid HTN in a secondary healthcare settings in Birmingham, United Kingdom. Findings showed that 63% (N=36) had controlled BP.
In summary, patients attending model 4 of integrated care were reported to demonstrate high rates of NCD control similar to HIV-uninfected populations in comparable settings. However, neither key HIV outcomes, outcomes before integration, nor comparison with patients in non-integrated care, were reported in all three studies.
DISCUSSION
Studies included in our review sought to evaluate long- term patient outcomes in various models of integrated HIV and NCD care. Eleven studies were identified and of these, three reported outcomes under Model 1 (integration of NCD screening and treatment services into established HIV),21–23 five reported outcomes using model 3 (simultaneous integration of HIV and NCD services at integrated health centre)24–28 and three studies applied model 4 of integrated care (integration of NCD and HIV care for patients with multi-morbidity).20,29,30 Notably, no study was found that reported outcomes using model 2 of integrated care (integration of HIV screening and treatment services into established NCD centre). Results from the three Model 1 studies showed that after receiving integrated care, patients achieved high rates of control of their comorbidities.21–23 Furthermore, HIV-related outcomes in these studies were found to be similar among comorbid and non-comorbid PLWH.22 This suggests that when managed appropriately, comorbid PLWH can attain equally high levels of HIV control comparable to PLWH with no comorbidities. However, even though these studies reported high rates of HIV and NCD control after integration, a noteworthy finding was that none of these studies included a comparator group e.g., co-morbid PLWH attending non-integrated care. As such, it is not known if the reported treatment outcomes in this model of care are higher than treatment outcomes in a non-integrated setting.
Simultaneous integration of NCD and HIV services (model 3) also appeared to confer clinical benefits to PLWH.24–28 Ameh et al showed that participants who attended integrated primary care facilities were found to have higher likelihood of control of their immune status as well as their NCD compared to participants who never utilized integrated care.27 This was the only study identified that demonstrated that integration may have a positive effect on patient outcomes using a well-defined comparator group. However, while NCD outcomes were reported, the absence of key HIV outcomes such as viral load suppression means the effect of this model on HIV control remains unknown.
Studies in our review also reported outcomes after integrating care of PLWH with comorbid DM or HTN (model 4).20,29,30 It is encouraging to note that patients with multimorbidity who attended this form of integrated care achieved good clinical control of their comorbidities at rates comparable to those of HIV-uninfected people in similar settings.32–35 However, similar to studies that reported patient outcomes in model 3, key HIV-related outcomes were not reported in these studies. Consequently, it also remains unknown if this model of care is more effective for control of HIV among patients with multimorbidity. Furthermore, these studies also did not include control groups to which patient outcomes after integration could be compared against. Comparison could take the form of before/after integration studies including the same PLWH with multimorbidity or comparison to multimorbid PLWH who received non-integrated care.
Patient outcomes in PLWH without NCD comorbidities receiving ART care through adherence clubs (MACs) have been described in literature.36–38 However, our review confirms a lack of evidence on the effectiveness of integrated MACs (that offer combined HIV and NCD care) for PLWH with multimorbidity who have more complex healthcare needs. Our review further highlights paucity of evidence from sub-Saharan Africa, where the burden of the HIV/NCD syndemic is greatest, with only five studies identified.22,25–28 Given that more than two-thirds of PLWH live in sub-Saharan Africa,39 studies evaluating the effectiveness of integrated HIV and NCD care are urgently needed in this setting to guide health care policy.
Our study has some limitations. Notably, due to heterogeneity of measures of disease outcomes used and diversity of the case mix and sampling strategies of included studies, we could not make meaningful comparisons both within and across the identified integrated models of care. For example, the diverse and non-uniform age range of adults in the included studies meant that it was not possible to compare integrated care outcomes of different adult age groups. In addition, as the inclusion criteria for the review focused on patients over 18 years old, the review was unable to explore age-dependent models of integrated care.
To evaluate non-inferiority of integrated care models, there is a need for randomised controlled trials that compare clinical outcomes for HIV and NCD in patients receiving integrated versus non-integrated models of care among PLHW with multimorbidity. Given the evidence of multimorbidity emerging at increasingly younger ages in sub-Saharan African PLWH,6 further research will also need to include adolescents in order to ensure integrated models of care are tailored to different age-groups. Lastly, our findings of highly heterogenous studies demonstrate the need for future studies to capture both HIV and NCD outcomes using comparable indicators in order to facilitate comparisons in future evidence synthesis research. To our knowledge, this is the first review to assess evidence on long-term patient outcomes in the context of various integrated HIV and NCD models of care; and we highlight the potential to leverage resources from HIV service platforms to provide effective integrated chronic disease care.10,13,40
CONCLUSIONS
The potential to leverage existing HIV infrastructure to provide NCD care to multimorbid patients without jeopardizing quality of care is a key consideration for health service delivery, particularly in high HIV-burden settings undergoing rapid epidemiological transition with a rise in NCD co-morbidity. Our review has identified evidence on integration of HIV/NCD care across diverse models of care, and the potential for integration to contribute to desired long-term patient outcomes. However, we highlight the need for the use of comparable indicators to assess both HIV and NCD outcomes in future studies. Furthermore, randomized controlled trials are urgently needed to compare clinical outcomes for HIV and NCD control in patients receiving integrated versus non-integrated models of care in order to evaluate non -inferiority of integrated care among PLHW with multimorbidity.
Acknowledgments
The authors would like to thank Prof Gill Morgan, a renowned reference librarian at the University of Cape Town Health Sciences Library for her immense assistance towards development of the search strategy for this review.
Funding
None.
Authorship contributions
BG: Conception and design of the study, literature search, article screening, data extraction and collation, synthesis and interpretation of data, manuscript drafting and revision, final approval and agreement to be accountable for all aspects of the work.
PO: Literature search, article screening, data extraction and collation, synthesis and interpretation of data, manuscript drafting and revision.
NJ: Conception and design of the study, interpretation of data, manuscript drafting, revision and final approval.
TO: Conception and design of the study, interpretation of data, manuscript drafting, revision and final approval.
Competing interests
The authors completed the Unified Competing Interest form at http://www.icmje.org/disclosure-of-interest/ (available upon request from the corresponding author) and declare no conflicts of interest.
Correspondence to:
Blessings Gausi MD MPH
School of Public Health and Family Medicine,
Faculty of Health sciences,
University of Cape Town,
South Africa.