


There is a very close link between satisfactory health governance and the benefit of one’s right to health protection, as the first has a direct influence on the second and contributes to Universal Health Coverage (UHC).1 International institutions have identified the reinforced implementation of health democracy as being useful to achieve this objective. Health democracy is “a will to improve health system’s quality, by allowing care recipients to express themselves and participate in the elaboration of health policies and reforms of the health system.”2,3 Its implementation requires the creation of a consultation framework that encourages better citizen participation in health system management. This participation is now identified as an internationally recognized citizen’s right. The international recognition of the participatory principle as indispensable to reinforce health systems dates back, at least, to the Declaration of Alma Ata on primary health care in 1978.4 The Ottawa Charter confirmed it in 19865 and by the recent Astana Declaration in 2018.6 International texts urge States to encourage citizens’ empowerment on health questions by developing their capacity to participate in decision-making processes. The definition of the notion of empowerment is still subject to debate. Yet, this notion can be understood as “the power to act autonomously according to one’s preferences and by controlling one’s destiny. It is a process (reinforce the power to act) as much as a state.”7 This notion can be implemented at an individual, community or organization level.
The success of health reforms depends, among other things, on considering the “opinions and choices of citizens, who must be able to exert a decisive influence on the way health services are designed and operated and share responsibility for their own health.”8 This inclusive citizen policy for better governance of health systems remains weak in sub-Saharan Africa (SSA). Addressing health governance challenges, however, is the subject of national, regional, and international policies. The global movement for Universal Health Coverage (UHC) in 20309 emphasizes the value of using citizen participation and health provider involvement in health decision-making processes. The movement advocates that strong tripartite collaboration between government policymakers, health providers, and health service users is a solution for strengthening sub-Saharan health systems. The value of citizen participation in good governance of health systems has been established.10–13 However, the sustained implementation of participatory mechanisms is still lacking in SSA. Indeed, the collection of grievances from users and practitioners of public and private health services can be organizationally complex. The exponential spread of cell phones in Africa and their ability to interact with other media have created new opportunities for interfaces between individuals and public decision makers.14 Numerous pilot studies suggest that mobile participation practices can contribute to the realization of these principles. Indeed, they constitute an extension and transformation of conventional citizen participation practices,15 to make them more inclusive, efficient and effective through the involvement of vulnerable citizens.16,17 Citizen m-participation is a technology-mediated interaction using the telephone to engage in discourse between citizens and elected or appointed officials on public policy issues.18 This interaction conducted “between the civil society sphere (citizens) and the official political sphere, and between the civil society sphere and the administration sphere”19 and it “may or not take place in an institutionalized setting and may be organized under the initiative of members of civil society or decision-makers.”20 Three models of m-participation can be identified: m-information, m-consultation, and m-collaboration18,19,21 considered as a partnership between the government and citizens.21,22 M-participation is bottom-up, when the flow is unidirectional from citizens to policymakers (state), top-down, when the flow is unidirectional from government to citizens, and inclusive or bidirectional, when the flow is from one to another of the actors in the health system.15,23–25
Mobile phones are mainly used in Sub-Saharan Africa (SSA) for patient information,16,17,26 health data collection, health surveillance and for improving adherence to care.27–30 They are also used in interventions that aim to collect the perceptions and opinions of users and providers on the health system,12 change citizens’ behaviors and strengthen the quality and quantity of health care services.4 However, there is still a lack of knowledge on the use of cell phones for citizen participation reforming and consolidating health care provision in SSA. Thus, this article aims to present the state of knowledge on the use of the telephone for the implementation of citizen participation in the public health policy-making processes in SSA.
METHODS
The method used to review publications is a scoping review following Arksey and O’Malley’s approach.31 The article was written following the PRISMA checklist for scoping Reviews.32
Identifying research question
The following question guided our scoping review of citizen participation in public health policy-making processes in Sub Saharan Africa through telephone: What do we know about citizen m-participation in the processes of formulating, analyzing and revising public health policies in Sub-Saharan Africa?
Identifying relevant studies
We conducted a systematic research of scientific articles, exploratory and systematic reviews, books and research reports on five electronic databases: Web of Science, Medline, PubMed, 1findr and Scopus. These bibliographic databases were selected depending on their fields of specialization and whether they comprised studies on public health policy-making questions. The research was completed by an analysis of grey literature on sites of institutions specialized in citizen participation in health care (WHO),10 on participatory mechanisms (IA2P)11 and new information and communication technologies (ITU).13 The search was conducted from April to August 2020.
Study selection
The collected literature was exported and saved in Covidence software. Two reviewers selected independently the documents according to inclusion and exclusion criteria, first by a selection based on titles and abstracts followed by a selection based on full text reading. After the text-based selection, they cross-searched the references of the included documents for new relevant articles to include. All uncertainties regarding the inclusion or exclusion of a document were discussed and decided collectively by two reviewers. To be included, references had to meet the following criteria: (i) the text is written in English or French, (ii) focuses on the use of the telephone for implementing citizen participation in health policy reform and/or adoption decision-making processes, and (iii) takes place in sub-Saharan Africa.
Data charting process
We first extracted (i) the basic information from the documents (authors, year of publication), (ii) the characteristics of the interventions implemented in the documents (geographical area, target populations, theoretical and conceptual approaches), and (iii) the authors’ limitations and operational recommendations. Then, following a second extraction grid created using Prieto-Martin’s framework for analyzing citizen participation.33
Synthesis of results
We extracted data related to the five following dimensions of citizen participation:
(i) the intensity of collaboration among stakeholders or the What dimension including a conflict, non-participation, consultative participation (levels of advice, consultation, and information) or “administrative participation”34 or “active participation”35 and the collaborative participation (levels of collaboration, delegation of power and delegation of control) categories;
(ii) the moments and stages of participation or the 'When’ dimension;
(iii) the institutionalization of participatory processes or the 'Where’ dimension (functional or organic level,36 episodic, periodic and continuous level and the lowest level is the minimal level said punctual or sporadic);
(iv) the transparency and intensity of the deliberations or the dimension of the How. Transparency favors the access of all the actors in the participatory process to the relevant information available;34,37 and
(v) stakeholders concerned and involved in the participatory process or the 'Who’ dimension. This framework is based on Arnstein’s.38
RESULTS
General characteristics
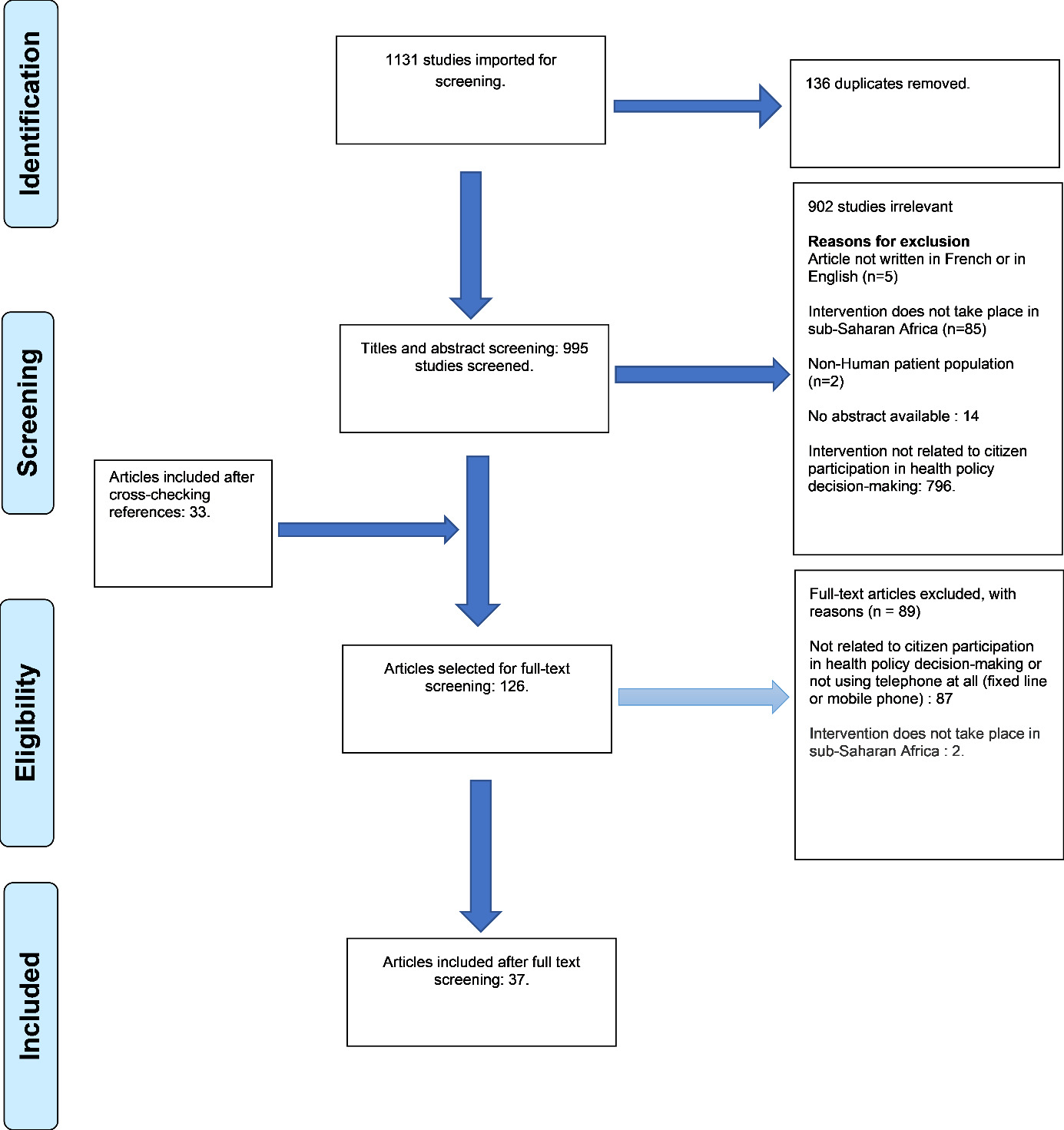
We collected 1131 documents from the implementation of our search strategy, with 136 duplicates. Of the remaining 995 documents, 902 documents were excluded. Reference analysis of the 93 retained documents allowed the inclusion of 33 additional documents. Of the 126 documents, 89 were excluded after full reading. 37 papers that met the inclusion criteria were finally included in our scoping review.
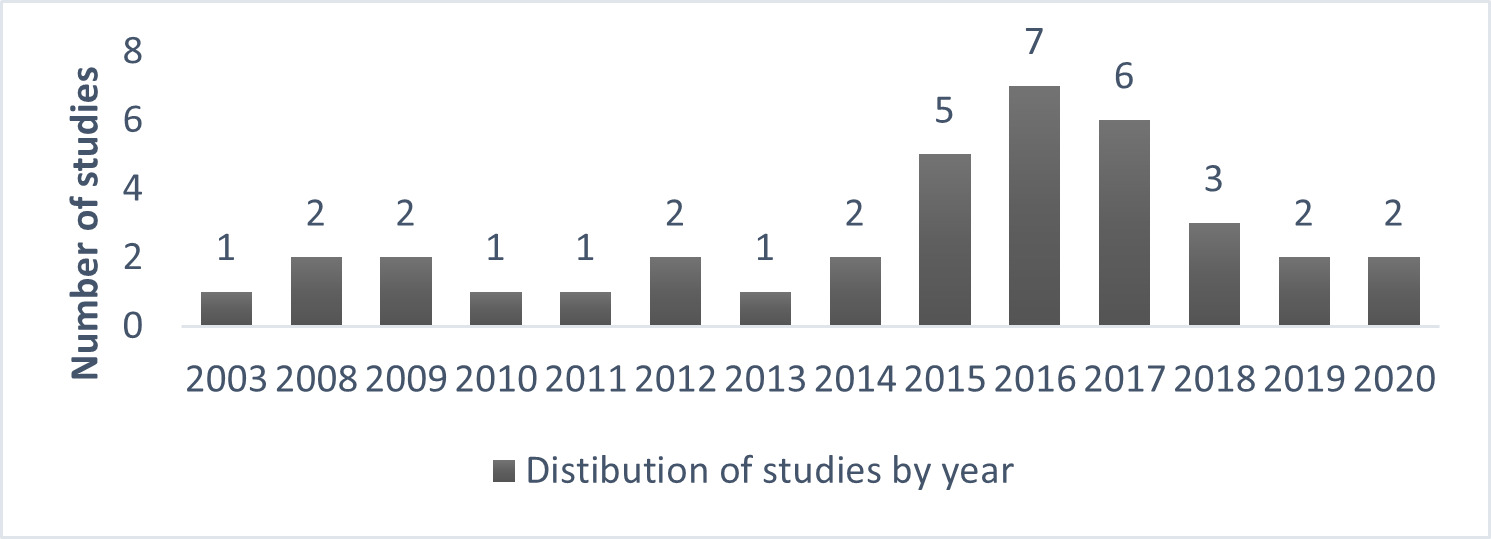
The included papers were published between 2003 and 2020 as shown in Figure 2 on the year distribution of papers.
The documents cover 15 sub-Saharan countries: Uganda, Ghana, Zambia, the Democratic Republic of the Congo, Burkina Faso, Cape Verde, Ivory Coast, Senegal, Kenya, Rwanda, Tanzania, South Africa, Nigeria, Malawi, Cameroon. Ten (10) of the thirty-seven (37) studies were multi-country.16,22,26,39–44 Figure 3 shows a predominance of m-participation interventions in the southern and eastern sub-region of Sub-Saharan Africa. South Africa covers 27% of the documents, East Africa also covers 27%. West Africa accounts for 24% of the documents. 14% of the documents cover Africa without specifying a country and 5% cover the whole world. Only 3% of the documents cover the Central Africa geographical area.

Seven main concepts are used to refer to the implementation of citizen participation through the telephones: mHealth,24,29,30,45–55 m-participation,17,28,39,56 e-participation,15,21–23,25,43,57 m-government,26,41,42,58 participation,27 e-consultation,12 citizen agency through ICT.44
Sixty-five percent of the studies organized a citizen m-participation process that focused exclusively on the telephone and 35% combined several ICTs including the telephone. From the documents specifying the distribution of intervention areas (n= 24), we can see that the participation processes set up in rural areas (n=6) and in urban areas (n=7) were almost equal. In addition, 11 of the 24 studies organized a comparative mechanism between rural and urban areas. In terms of methods, qualitative studies (n=18) and mixed studies (n=11) predominate, particularly in participation-action-research processes. Quantitative studies (n=5) and reviews (1 synthesis note, 1 literature review and 1 report) were less numerous. Refer to Online Supplementary Document for details.
The various interventions of implemented citizen m-participation had 5 distinct objectives.
-
Modeling m-participation: the first objective of its interventions is to elaborate a citizen m-participation model.17,21,23,27,57,59 For example, NGO ToroDev28,30,60 proposes a participatory model based on the ICT convergence approach to promote the defense of democracy by citizens in three East African countries: Uganda, Kenya and Tanzania. It is a hybrid model combining consultation (information + consultation) and collaborative participation (participation, action, and research.).
-
Evaluating pertinence: the second objective is to evaluate the pertinence of telephones as citizen participation tools.12,14,16,22,24,25,29,39,40,43,44,51–53,58 Lechat et al. demonstrate the technological and instrumental relevance of the telephone in the Burkinabe context (strong geographical disparities in health infrastructures, predominantly rural population) for collecting the opinions of users and health workers.52
-
Collecting opinions: the third objective is the implementation of a participatory mechanism to collect citizens’ perceptions on the advantage of resorting to health m-participation.28,30,45–47,54–56 Brinkel’s 2017 study collects the perceptions of health workers on the use of the telephone tool in two urban (Accra and Tema) and two rural areas (Shai Osudoku Municipal and Ga West) in Ghana. The analyzed intervention deploys a toll-free telephone number with an interactive voice server to assist health carer of children under five.56
-
Requirements for m-participation processes: The fourth objective identified in the 37 papers is to highlight the social, political, technological, and financial requirements for citizen m-participation.41,42,50,57 Bwalya’s 2009 paper analyzes these factors for Zambia.
-
Empowering citizens: Citizen Empowerment: The fifth objective we note is the empowerment of citizens in monitoring the quality of health care provision. Hrynick’s 2017 article presents an example of empowerment of journalists in South Africa that is presented in the box below.
The intensity of participatory processes: the WHAT dimension
Eighty-seven percent of the 37 documents (n=29) fall into the category of consultative participation. The documents implementing consultative m-participation collected citizens’ opinions on the health offer, their perceptions on the use of cell phones for health care delivery. These processes were all preceded by information on the participatory mechanism. For example, in the m-participation mechanisms,45–47,53 a preliminary phase of information and exchanges with the stakeholders on the projects was initiated to better adapt the participatory tool and explain its purpose. Focus groups were also set up to inform participants. The requirement of prior information of the concerned actors was thus fulfilled.
Weinman’s ICT work gathered the views of South African citizens on a proposed national health insurance bill and raised awareness of their rights to free, quality health care.12
Most of the documents deal with m-participation initiatives that result from private initiatives, including civil society organizations and non-state structures. For example, these were initiatives of structures specialized in citizen participation like ToroDev,23,61 Making All Voices Count,24,40 Grassroot Soccer,48 Text to change,27 Save The Mothers49 or initiatives of researchers14 or even research structure consortiums.29,45,52 Policy makers, however, are stakeholders in the processes, and the results are intended to be transferred to them as a basis for future health reforms and legislationl.28,57 Considering the information, opinions and views of health care users and providers requested through participatory mechanisms remains highly dependent on policy makers. Indeed, despite the suggestions and results of participatory processes, they retain the ability to make the decisions they deem appropriate.
Regarding the flow of exchanges, out of the 37 documents, 30 implemented a bi-directional or inclusive flow of exchange, 6 a bottom-up flow, and only one study39 had a top-down flow. Most of the documents therefore promote information sharing and citizen feedback through the expression of opinions, perceptions or recommendations/advice. Mwase’s 2020 document discusses a two-way exchange between the project NGO, health workers, and community members in Uganda on the issue of using a toll-free number to access maternal and newborn care.49 The health workers and community members receive questions from the NGO over the phone. They then send their opinions to the NGO through the telephone.
Moments and steps of m-participation: the WHEN dimension
All the papers analyze projects implemented by civil society organizations and non-governmental organizations. This limits the applicability of Martin-Prieto’s framework for analysing the moments and stages of m-participation. Only one paper, Hellstrom’s 2008 article, mentions a telephone-based citizen participation initiative implemented directly by governments (Tanzania, Uganda and Kenya).39
The documents analyzed highlight the fact that the decision-making stage of public policy reform partly eludes two of the health system actors solicited in m-participation processes: health workers and health system users. Indeed, the participatory processes described in the thirty-six documents (n=36), solicit citizen m-participation in the process formulation phase,12,25,27,29,43,46–48,55 in its implementation phase,21,23,45,49,54,57,58,61 or in its monitoring and evaluation of the participatory process14,16,17,24,40,44,56,59 prior to transfer of evidence to policy makers. There is no mention of inclusion in the adoption or non-adoption of the final decision or its amendment prior to implementation. Six (n=6) do not enter any of the stages.15,22,26,41,42,57 The following box describes a citizen participation initiative in Uganda that, despite the lack of binding power of the citizens who initiated it, resulted in a decision that met the expressed need.
The level of institutionalisation of participatory processes (WHERE)
The most representative level is minimal or sporadic institutionalization with 34% of the records (n=13). This is the lowest level of institutionalization in Prieto-Martin. The participatory processes there are punctual, carried out with an exceptional character in the example of Diese 2018 or Greenleaf 2019.29
Following the minimal level, the periodic, episodic, and continuous level of institutionalization (n=11) has 29% of the included documents. Brinkel 2020 analyzes the implementation of periodic citizen m-participation. It is part of a concept and pilot study for a mobile phone-based electronic health information and monitoring system conducted between 2014 and 2020 in Ghana.17,60
The organic level (n=7) accounts for 18% of the documents. Baguma’s three papers activate the organic level of institutionalization. Indeed, the participatory process in these three documents is implemented by a participatory institution, ToroDev, an organization specialized in the empowerment of citizens through ICTs.21,23,61 ToroDev is an organization specialized in the question of citizen empowerment thanks to ICTs. This non-governmental organization has a permanent character.17,60 The least represented level in the documents is the functional level with only one study.41
It mentions the Mobile Information Data Collection Analysis System (MIDAS) application adopted by the Ugandan government to facilitate health data collection and exchange with its citizens from the villages to the ministry via SMSes. Six descriptive studies are omitted in the classification.
The transparency and intensity of deliberations: the HOW dimension
Regarding transparency, m-participants were provided with available, clear, appropriate, and understandable information at the beginning of each participatory mechanism. Indeed, almost all of the 37 studies had consent forms or focus groups. In addition, the intensity of deliberation was satisfactory.33 The deliberative spaces met the evaluation criteria of Gutmann and Thompson.37 The channel of exchange was the cell phone with physical places of exchange (focus groups and physical qualitative interviews). The discussion spaces therefore met the criteria of openness, diversification and inclusiveness. They allowed the parties involved to exchange their opinions and the citizens to be really put to contribution.
The involved’ stakeholders: the WHO dimension
The need to include all stakeholders relevant to the issue at hand with citizen m-participation was largely addressed by 31 studies implementing a participatory process and clearly mentioned by another six studies describing criteria for implementing citizen participation. In 5% of the documents, the exclusive stakeholders were policy makers (n=22). In 22% of the cases, health system users were the only stakeholders (n=8). For example, the participatory process analyzed in the 2015 Thinyane document58 aimed to explore how residents used technology and participated with local government in service delivery. The stakeholders included were therefore the residents of Grahamson Town involved in the participatory process. 14% were oriented to health care providers (n=5). In Macharia’s 2015 paper, the objective was to analyze how ICT could play a role in improving health care. The stakeholders included were only health care workers.26 More than half, i.e., 59%, included at least two or all the stakeholder categories (n=22). To analyze the acceptability of using the telephone to deliver maternal and newborn health care in Uganda, Mwase used citizens and health workers who are the primary actors affected by such a policy. The results show that there is a strong emphasis on inclusiveness of all stakeholders.
DISCUSSION
Implementing health democracy to strengthening health systems requires the adoption of practices related to citizen empowerment. To have a wider reach while including the different social strata of sub-Saharan Africa, the use of communication technologies, namely the telephone, is one way. The aim is to establish m-participation among stakeholders in the formulation of public health reforms and policies.
The analysis of the current state of knowledge identifies three benefits of using m-participatory processes in decision-making processes in SSA: 1) it can improve the quality of the design of public health system reforms 2) it can mitigate the risks associated with implementing health sector policies by reducing the gap between needs and the health reforms implemented23 3) adopting quality reforms that consider real needs can only strengthen health systems and health governance.62
This scoping review demonstrates the adoption in SSA of citizen m-inclusion in public health policy processes. It sheds light on the weakness of government commitment to this issue. In sub-Saharan countries, citizen m-participation focuses are mainly on improving the delivery of administrative services via ICT. The study also provides useful insights into implementing m-participation in SSA: the intrinsic benefits of using m-participation compared to traditional participation practices, and the challenges to be considered before and during the m-participation process.
Why opt for citizen m-participation?
From a technological viewpoint , telephone tools have a high penetration and acceptance rate in sub-Saharan countries. It removes multiple communication and geographical barriers specific to Sub-Saharan Africa thanks to its accessibility, its reach (coverage of remote rural areas). Besides, it facilitates interactions between actors.39,61 For example, in Burkina Faso, the telephone penetration rate was 99% at the end of 2020.63–65
In addition, the versatility of the telephone tool is also an incentive to use m-participation. The telephone can simultaneously fulfil three technological functions: it is used for the transmission and collection of information (circulation of information in space); it allows the storage of information (circulation of information in time, allowing the sharing of data on a web-based system); and it allows for the calculation of information (transformation of information), including data aggregation, validation and data validation and manipulation/calculation/analysis to generate reports.42,54
From a socio-political point of view, the first advantage of m-participation is that it contributes to the empowerment of citizens by facilitating their access to reliable and adequate information and by creating tools for knowledge sharing. This mechanism allows stakeholders to initiate interactive or bidirectional, top-down or bottom-up dialogues. The stakes are high. Indeed, the participatory process will help build trust among stakeholders and implement public health policies by giving citizens a channel to express their opinions, dissatisfaction, and proposals for reform to policymakers.14,61 In addition to empowering health system users,40,51,59 public opinion expressed through m-participation also contributes to improving the system’s responsiveness, particularly for health workers and policy makers.52,53 It calls for increased professionalism in the performance of their duties.57
The second socio-political benefit of m-participation is its contribution to the transparency and accountability of government and governance. It provides citizens with a means of monitoring the management of public affairs and allows them to keep an eye on elected officials and other policy-makers.12,23,44
What are the challenges related to citizen m-participation?
From an economic perspective, the limited financial resources of Sub-Saharan African states hinder their ability to implement citizen m-participation.61
From a technological perspective there are three major challenges: 1) the application development processes are slow, especially the choice of m-participation approaches that would be feasible in terms of interoperability.26 This challenge is compounded by the complexity of finding a financially acceptable agreement in negotiations with technology partners in the project design process.52 2) in the deployment phase of the project, the instability of the Internet connection when needed limits the scope of participatory processes. 3) the length of the questionnaire sent over the phone can be a deterrent. Indeed, when the process is long, the dropout rate before completion is higher.
From a political point of view, the main challenge is the weakness of political will with the absence of government leadership on the issue. Indeed, almost all the initiatives analysed were carried out by non-governmental actors. This explains the high rate of pilot projects and their dependence on external technical and financial support. The weak leadership of sub-Saharan states also leads to a lack of sustainability of citizen m-participation projects as well as a lack of alignment and integration of participatory mechanisms in health sector plans and strategies.15,26
From a legal perspective, there is the issue of protecting the privacy of individuals taking part in m-participation mechanisms.57 Besides the need to protect the participants’ privacy, there is also the need to guarantee their security. In some Sub-Saharan states, despotic tendencies have been noted that can undermine the expression of citizens’ opinions in such participatory processes.39,61 Citizen m-participation can therefore be impeded by the fear of reprisals in case of interception of opinions.
From a social point of view, there are multiple challenges related to the tool’s degree of understanding and accessibility. First, the understanding of the tool plays a key role in the ability of citizens to interact with the technological mechanism implemented. This makes it a potential barrier to the quality and quantity of information collected. For example, many of the calls collected in the studies analyzed resulted in invalid and irrelevant content: curious callers, requests for explanations, encouragement, health information, etc.52,53 The overestimation of people’s ability to use technology is a second understanding challenge that must be anticipated for better reach of m-participation mechanisms. For example, the high level of basic and technological illiteracy in rural and urban communities may result in low access to and use of m-participation mechanisms.61 Also, skepticism about the potential of mobile technology to improve government services limits the reach and rate of m-participation. This skepticism is partly due to the digital gap, including aspects of electronic illiteracy.25
Second, regarding accessibility, there is a gender digital divide in SSA that hinders women’s participation by phone. This gender-related inequitable access to technology is a reality in both rural and urban areas.29 Greenleaf’s 2019 paper analyzing phone use in Burkina Faso to expand access to family planning services shows disparities in ICT access and use. Of 3215 women surveyed, 47% had a cell phone. This reality is endorsed by the 2019 GSMA report which pegs the cell phone ownership gap between men and women in sub-Saharan Africa at 15% in 2018 meaning 86 million of Sub-Saharan women not connected.66
From a social perspective, we propose four groups of recommendations to address the social challenges of m-participation in SSA.
First, in the context of the implementation of mobile applications or the creation of a toll-free number allowing citizens to express their opinions, several solutions: a better consideration of language and literacy factors is needed to reach the largest number of people; a participatory process that allows the inclusion of all social strata, especially those with visual and hearing disabilities. Indeed, the use of a voice service (voice messages) in several languages can compensate for visual and auditory disabilities and illiteracy that hinders m-participation.24,53 It is also essential for these services to be accessible and usable for free, to allow the principle of equity.
Second, it is necessary to create online applications and forms that will facilitate and increase the rate of citizen participation.49
Third, for more intense deliberations, it is recommended to collect participation in supportive environments. A contextual analysis should be conducted beforehand to ensure that the m-participation implementation process is appropriate for the target population.
Fourth, telephone messages (SMS, IVR) should be relevant, positive, simple, sparse, and created to fit the context of the target audience.28,51
From a technological point of view, three major recommendations stand out. First, to address the technological challenges, increased interest should be given to developing mobile and wireless networks and associated infrastructure, promoting cell phone penetration and therefore increased accessibility of telephony tools. Second, it is recommended that simple tools be developed to assess e-readiness prior to implementing a m-participation health project. This will counteract the negative consequences of overestimating citizens’ ability to use this tool.52 Adopting an ICT convergence strategy, such as communication via different media.49 In addition to the telephone, increases the m-participation rate. A project for a technological platform for citizen participation in health called TOPICs deployed since 2020 in three SSA countries (DRC, Benin, Burkina Faso) has established the stimulating role of the convergence of ICTs in m-participation mechanisms. Indeed, the project has observed an increase in the number of daily calls to the toll-free number after radio spots, interactive broadcasts.67
From a political point of view, four major recommendations emerge. First, in formulating the policy for citizen participation, it is necessary to use the services of specialized business analysts in the field of mobile telecommunications and to incorporate a “modeling” mechanism. This will allow for testing how the m-participation system will work before it is adopted and implemented. The objective here is to avoid overly ambitious interventions.30 Second, states need to support and promote research on m-participation. Indeed, through the production of knowledge, methods and good practices, participation mechanisms will be better understood and implemented.59 In defining the mechanism of m-participation, it is essential to take a systemic perspective that does not separate the technology to be deployed (phone) from the environment where it will be deployed when assessing the value of m-participation to citizens.
Third, because it is essential to include everyone and improve the m-participation of socially excluded groups, it is recommended that local forms of organization be linked to the formal institutional forms of governments organization. To do so, it is necessary to link the different forms of organization and the administrative institutions of governance.
Fourth, it is essential that governments take the lead on the issue of m-participation42 and the implementation of efficient education programmes to ICTs. These programs will need to encompass digital literacy, in formal educational structures, and professional practices to counteract skepticism about the potential of mobile technologies to increase government services and accountability.22 To this end, giving more information and raising awareness on implemented governance and online participation tools is also a necessity. Citizens’ participation to electronic governance has to be explained and understood both by citizens and national leaders to be efficient and effective.39
From a legal perspective, it is suggested that legal measures be adopted to protect the privacy of m-participants and to ensure the security of data and interactions. This will also lead to better regulation and development of the legal aspects of mobile applications.22,46,54
Limitations of the Scoping review
This scoping review, despite its innovative nature, is not without its limitations. First, the presence of a selection bias is possible. In the data selection process, we only selected articles written in English and French. A similar limitation affects the selection of databases. However, we tried to minimize selection bias by exploring both general and specific databases.
Second, this scoping review does not evaluate the methodologies used in m-participation experiments but focuses on exploring the challenges and benefits in the decision-making process. Despite its limitations, the scoping review was the most appropriate method to reflect our research question’s exploratory nature and general focus. It will serve as a general mapping for empirical research on citizen m-participation in health decision-making in Sub-Saharan Africa.
CONCLUSIONS
Citizen m-participation in health encompasses citizen m-information, m-debate on health issues, and m-participation in deliberation and decision-making for public health policies. The m-information of citizens highlights the low level of citizens’ information on the health decision process, the m-debate underlines the closed nature of the public space. Finally, m-deliberation and m-participation in decision-making highlight the low level of inclusion of citizens in decision-making processes.68
In SSA, the recurring scale of citizen participation is advisory participation. It is not irrelevant but calls for more projects to test the real benefit of this participation depending on the willingness of decision makers for the quality and effectiveness of reforms and laws affecting collaborative health systems.
The scoping review shows that in sub-Saharan African states, access to and use of ICTs are now seen as mechanisms that can potentially facilitate inclusive health governance processes. The development of participatory action research processes will allow us to continue to test the effectiveness of such innovation in strengthening health systems.
Acknowledgements
Our thanks to Laurence GOURY, librarian at IRD Bondy, to Sarah LOUART, Lola TRAVERSON and Ludovic AUVRAY for their help in the realization of this article.
Funding
This work is supported by Global Affairs Canada (grant number: D003027/P01475) and stems from the call for proposals “Technological Platforms for Strengthening Public Sector Accountability and Citizen Engagement”. The project was selected by Global Affairs Canada through a competitive process. (The funding body had no role in the design of the study, the collection, analysis and interpretation of data, nor the writing of the manuscript.)
Authorship contributions
Conception and design: OWAS, VR, EB, SB. Acquisition of data: OWAS, SB, VR, EB. Analysis and interpretation of data: OWAS, SB, VR, EB. Drafting of the manuscript: OWAS, SB, VR, EB. Critical revision of the manuscript for important intellectual content: VR, SB, EB, OWAS. Statistical analysis: OWAS, EB, SB, VR. Administrative, technical, or material support: VR, SB, EB. Supervision: VR, EB, SB.
Competing interests
The authors completed the Unified Competing Interest form at http://www.icmje.org/disclosure-of-interest/ (available upon request from the corresponding author) and declare no conflicts of interest.
Correspondence to:
Wendkouni Adelphe Sabine OUEDRAOGO,
Affiliation: Unité Mixte Résiliences, Institut de Recherche pour le Développement, Bondy, France
Personal address: 7 place Miollis, 13100, Aix-en-Provence
Email: [email protected]