Permanent hearing loss is the most common neurological sequalae among meningitis survivors in low- and middle-income countries.1 The World Health Organization advocates for immunization against the causal pathogens of bacterial meningitis, not only to reduce childhood mortality, but also to prevent the lifelong disabilities associated with the disease.2
The Pacific Island region is estimated to have among the highest rates of hearing loss in the world.3 Although the proportion of hearing loss due to meningitis is not known, encouragingly, the most recent Global Burden of Disease Study report estimated that the incidence, deaths, and disability-adjusted life years (DALYs) for meningitis in the Pacific Islands were in decline.4 The Millennium Development Goals (2000-2015) played a significant role in strengthening childhood immunization schedules against the causal pathogens of meningitis (Haemophilus influenzae Type b, Streptococcus pneumoniae, Neisseria meningitidis), and this agenda continues under the current Sustainable Development Goals (2016-2030). The availability of meningitis immunizations and their coverage rates in the Pacific Islands are summarised in Table 1.5
A review of the literature found that there is little research on meningitis in the Pacific Islands.5 A recent hospital-based study from Fiji was published in 2012, and reported that Streptococcus pneumoniae (55%) was the most common bacterial pathogen for meningitis among children aged 0-5 years, with a case fatality rate of 36%.6 Causal agents Neisseria meningitidis (15%) and Haemophilus influenzae type b (10%) were significantly less common. A further two hospital-based studies were found from Vanuatu and Papua New Guinea,7,8 however, the information is likely to be outdated due to the improvements in routine childhood immunizations. A recent review of meningococcal disease (i.e., Neisseria meningitidis) in the Asia-Pacific region did not include information for any Pacific Island country.9
There is similarly very little in the literature on neurological sequelae among meningitis survivors in the Pacific region. The most cited paper reports a study from Vanuatu in 1994, where permanent hearing impairment was measured among 32.3% of meningitis survivors.10 The interpretation of more recent publications on hearing loss are limited by sample size and methodology.6,11 There were no publications on visual disabilities among meningitis survivors in the Pacific Islands. There was one paper from Papua New Guinea advocating for improved clinical and rehabilitation services for people with physical and mobility impairments following meningitis, especially among people living in rural/remote settings.12
The Ear, Nose, and Throat (ENT) clinic of Tupua Tamasese Meaole (TTM) Hospital is currently expanding their service to include review of all patients at-risk of ear and/or hearing disorders in Samoa (Figure 1). The aim of the proposed study is to implement routine ear and hearing assessments for all meningitis survivors seen at the TTM Hospital, and to report the prevalence and pattern of ear disease and hearing loss among these patients.

Our aim in publishing this study protocol is to facilitate implementation of routine ear and hearing assessments among our Pacific Island colleagues, especially where both ENT and audiology services are available.
METHODS
Planning and preparation
Ethics approval
This study was approved by the Government of Samoa Ministry of Health Ethical Research Committee and the University of Queensland Medical Ethics Research Committee (Approval No. 2020000255).
Aims
The aims of the study are to evaluate the prevalence and pattern of hearing loss among meningitis survivors at the Tupua Tamasese Meaole (TTM) Hospital. The results will guide the development of health promotion activities aimed at reducing preventable ear disease and hearing loss through improved routine immunization population coverage rates. The results will also provide baseline data for comparison with subsequent surveys, and enable the assessment of the effectiveness of health education and health promotion activities.
The study will evaluate:
-
Number, age, and gender of meningitis survivors registered at TTM Hospital,
-
Number, age, and gender of meningitis survivors attending the ENT/audiology Clinic for ENT/audiology assessment, and
-
Prevalence and pattern of hearing loss among meningitis survivors attending the ENT/audiology Clinic for ENT/audiology assessment.
Personnel
The study will be led by the research audiologist (AK) and the Head of the ENT Department (SP), who will both perform the data collection. Data analysis will be performed by the audiologist in collaboration with the Hearing Research Unit for Children at the University of Queensland (Australia) (CD).
Design
The study will use a prospective and observational design.
Setting
The study will be set at the ENT/Audiology Clinic of the TTM Hospital in Apia (Samoa).
Participants
The study population will consist of all patients (children and adults) admitted to TTM Hospital with a meningitis diagnosis from January 2021 to December 2022.
Assessment
Routine ENT and audiology clinical assessment. The ENT surgeon will perform an ear examination for each ear, and, if required, ENT nurses will perform interventions (i.e., wax removal). The audiologist will perform an audiometry assessment to determine the hearing levels for each ear. If a hearing loss is detected, the nature of the hearing loss (temporary/permanent) will also be determined.
The results will be discussed with the patient (or caregiver in the case of children), and recommendations/reviews will follow routine ENT/audiology clinic procedure.
Equipment and consumables
Routine clinical equipment will be used in the study. There is no consumable equipment as probe tips (otoscopy, tympanometry) are sterilized daily and re-used.
-
Otoscope (for ear examinations)
-
Suction machine (for any nurse interventions)
-
Tympanometer (for assessment of the eardrum)
-
Audiometer (for assessment of hearing levels)
The documentation required for the study is listed below, and will be contained within a simple plastic folder for utilization by the research team:
-
Information sheet for participants (English) – Pattern and prevalence of hearing loss among meningitis survivors in Samoa.
-
Information sheet for participants (Samoan) – Pattern and prevalence of hearing loss among meningitis survivors in Samoa.
-
Participant consent form (English) – Pattern and prevalence of hearing loss among meningitis survivors in Samoa.
-
Participant consent form (Samoan) – Pattern and prevalence of hearing loss among meningitis survivors in Samoa.
-
Data collection sheet - Questionnaire (English) – Pattern and prevalence of hearing loss among meningitis survivors in Samoa.
To reduce the cost of record-keeping consumables, the Samoan version of the consent form and the data collection form will be printed back-to-back on the same sheet of paper. To further reduce the cost of record-keeping consumables, a laminated copy of the Samoan version of the information sheet and five non-laminated copies only will be kept in the study folder (information sheets to be kept by individuals only if requested).
Quality control
The following measures will be implemented to ensure maximum quality control for the study:
-
Daily maintenance of all clinical equipment (calibration, sterilization, etc.),
-
All staff will be informed of the record-keeping requirements of the study to ensure optimal documentation,
-
Regular review with the team leader during the study period to enable any clarification of issues if/as they arise,
-
Signature of staff member(s) on the data collection form, and
-
Team leader provides update and feedback on the study at staff meetings, and promotes team input for improvement of the clinical service.
Conducting the study
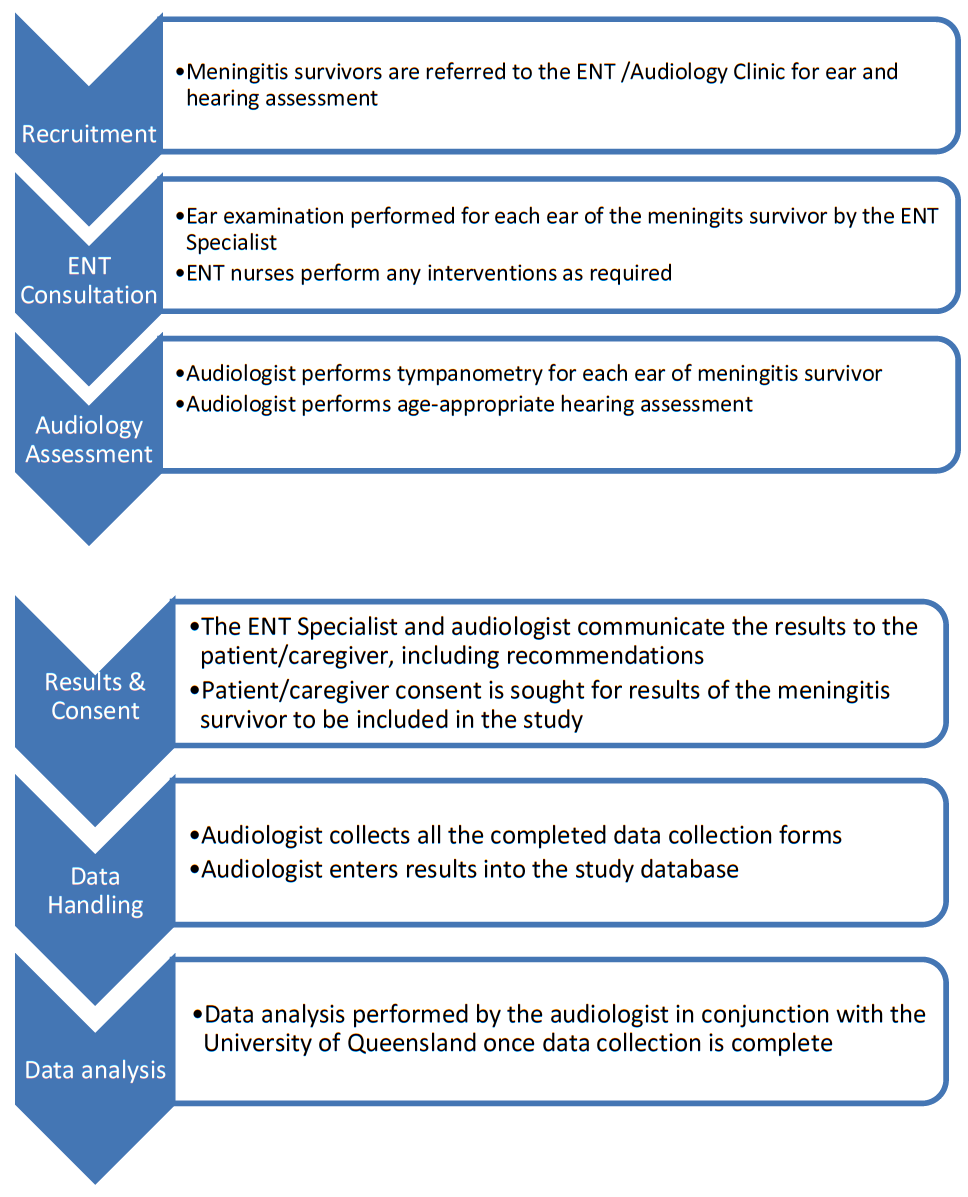
The recommended workflow on the days of data collection is summarized in Figure 2.

Recruitment of participants
The second author (SP) is a senior medical officer at the hospital, and well placed to be alerted to any suspected cases of meningitis admitted to the hospital. When the patient is discharged from the hospital and a review medical appointment scheduled, this visit will also include an ear and hearing assessment.
After completion of the ear and hearing assessments, the patient (or the caregiver of a child participant) will be verbally informed of the present study (Participant Information Sheet available for details), and invited for their de-identified results to be included in the study. Consent is sought at this stage to ensure that the patient has no concerns about their involvement in the study impacting on the clinical care they receive. Should they be willing, the patient (or the caregiver of a child participant) will be asked to sign the Participant Consent Form.
Data collection
The ENT/Audiology Clinic staff members performing the data collection will complete the data collection form purposefully designed for this study.
Demographic information
The following demographic information will be recorded:
-
Patient name
-
Date of birth
-
Age
-
Gender
-
Hearing concerns prior to meningitis infection (yes/no)
-
History of immunization against causal meningitis pathogens (yes/no, Haemophilus influenzae Type b/Streptococcus pneumoniae/ Neisseria meningitidis)
-
History of meningitis: administration of ototoxic medication (yes/no), causal meningitis pathogen (Haemophilus influenzae Type b/Streptococcus pneumoniae/ Neisseria meningitidis)
ENT consultation
All meningitis survivors will undergo ear examination for both ears. An overall diagnosis for each ear is made as per routine ENT clinic protocols:
-
No abnormalities detected: NAD
-
Acute Otitis Media: AOM
-
Acute Otitis Media with Perforation: AOMwiP
-
Chronic Suppurative Otitis Media: CSOM
-
Dry Tympanic Membrane Perforation: Dry TM Perf
-
Otitis Media with Effusion: OME
-
Eustachian Tube Dysfunction: ETD
-
Impacted Cerumen
-
Foreign Body
-
Fungal Otitis Externa
-
Could not assess
The Rhinne and Weber tuning fork tests will also be performed, and an overall diagnosis provided as per the routine ENT Clinic protocols. Should wax removal, foreign body removal, or aural toilet be required, the ENT Consultant will direct the ENT nurses to perform this task. ENT medical or surgical intervention will be recommended as appropriate.
Audiology assessment
All meningitis survivors will undergo an audiology assessment consisting of tympanometry and audiometry. Tympanometry is performed for each ear, and results classified according to the modified Jerger’s system (Table 2).
Play Audiometry or Pure-tone Audiometry is performed as age-appropriate. (N.B. At the time of writing, Visual Reinforcement Orientation Audiometry (hearing assessment for older infants and toddlers) is unavailable in Samoa). Pure-tones are presented to each ear via headphones at 500, 1000, 2000, and 4000 Hz (250 and 8000 Hz for older children and adults). Bone conduction is performed for 500, 1000, 2000, and 4000 Hz. Air-conduction and bone-conduction masking is performed as indicated.
The audiologist will report the degree (Table 3) and nature (conductive, sensorineural, mixed) of hearing loss for each ear. Degree of hearing loss is calculated from the four-frequency average. Based on the results, the audiologist will make recommendations as appropriate (i.e., management by ENT clinic, referral to SENESE for amplification/intervention options).
Data handling and analysis
All data handling and analysis will be done by the audiologist in consultation with the ENT Clinic staff as required. The coding strategy for statistical analysis is provided below (Table 4).
Demographic information
A descriptive analysis will be performed for the total number of meningitis survivors seen by the TTM ENT/audiology clinic from January 2021 to December 2022. The analysis will include age range (mean and standard deviation), and if exact age of participants cannot be determined, the age of participants may be described in decade subgroups (i.e., 20-29 years, 30-39 years). Results will be presented in tabulated form using a cross-analysis (i.e., age subgroup x gender x residence x meningitis history variables).
Analysis of variables
For each ear, descriptive analysis will be provided for ENT consultant diagnosis, nurse intervention, degree of hearing loss, and nature of hearing loss. For each patient, a descriptive analysis will be provided for outcomes of the ENT/audiology assessment.
Chi-Squared Linear-By-Linear Association tests will be performed to investigate for any significant associations between ENT/audiology assessment outcomes, and gender, age, residence, and meningitis history group variables. Any significant findings will be highlighted.
The prevalence of hearing loss among this sample of meningitis survivors will be presented as a percentage (%). The degree of hearing loss in the better ear among this sample of meningitis survivors will also be presented as a percentage (i.e. % normal hearing, % mild hearing loss, etc.). The type of hearing loss will also be presented as a percentage (i.e. % conductive, % sensorineural, % mixed).
DISCUSSION
The results of this study will be prepared as a research paper for submission to a peer-reviewed journal. Similar studies have been published in the International Journal of Pediatric Otorhinolaryngology. The published paper will be also be delivered to the Government of Samoa Ministry of Health, including an action plan for health education and health promotion activities based on the results.
The ENT/audiology clinic will collaborate with health promotion officers to prepare a short media release about the study and the results. This will be done in consultation with the Government of Samoa Ministry of Health to ensure information is appropriate and receives maximum population coverage. The aim of the media release is (1) to promote the role of immunizations in the prevention of illness and disability, (2) to increase community awareness of avoidable ear disease and hearing loss, and (3) to encourage timely attendance at health services for treatment of ear disease and suspicions of childhood hearing loss.
We include the English versions of the participant information sheet and participant consent form as additional files with this publication to further facilitate similar studies of this kind, especially among our Pacific Island neighbors.
Acknowledgments
Thank you to the Government of Samoa Ministry of Health and the Chief Executive Officer of the Tupua Tamasese Meaole Hospital for granting permission for the study. Thank you in advance to all caregivers and child participants.
Ethics approval and consent to participate
This study was approved by the Government of Samoa Ministry of Health Ethical Research Committee and the University of Queensland Medical Ethics Research Committee (Approval No. 2020000255). All participants will sign a consent form prior to data collection.
Availability of data and materials
All data generated or analyzed during this study will be included in the published article.
Funding
None.
Authorship contributions
AK wrote the initial draft manuscript, and all authors provided feedback. AK performed revisions to the manuscript as appropriate, and all authors read and approved the final manuscript.
Competing interests
The authors completed the Unified Competing Interest form at www.icmje.org/coi_disclosure.pdf (available upon request from the corresponding author), and declare no conflicts of interest.
Correspondence to:
Annette Kaspar
ENT Department, Tupua Tamasese Meaole Hospital
Ministry of Health, Apia, Samoa.
[email protected]