Cardiovascular diseases have risen to be the top cause of mortality and morbidity globally and at a faster pace in developing countries.1 Global health policies are aimed at reducing premature mortality from non-communicable diseases (NCDs) with goals targeting significant reduction by 2025.2 Obstructive sleep apnea (OSA) is an established common denominator across all societies, severely underdiagnosed, and a potentially modifiable risk factor for NCDs. Therefore, it is imperative to augment worldwide screening and referral efforts for OSA to make diagnosis and treatment more efficient and effective.
OSA is a chronic condition that results in partial obstruction of the upper airway during sleep and/or episodes of collapse of the upper airway with complete obstruction.3 This obstruction results in arousal of sleep and decreased oxyhemoglobin saturation, which may lead to neuro-behavioral and cardiovascular consequences.4 Without treatment, OSA leads to excessive daytime sleepiness (EDS), cognitive dysfunction, decline in work performance, and negative impacts on quality of life.5 Evidence also suggests that OSA is linked to systemic hypertension, cardiovascular disease, obesity, dyslipidemia, and abnormalities in glucose metabolism,3,6 with a growing body of evidence that OSA may be related to many other chronic disease states, as well. In addition to the significant impact on individual health, undiagnosed OSA is recognized as an important public health issue. For example, it has been shown that EDS is associated with road traffic accidents, leading to a significant economic burden for developing countries.7,8
Although many adverse health consequences of OSA are recognized, the majority of patients remain undiagnosed.3 This makes it difficult to adequately study the connections between OSA and the other chronic disease states that are hypothesized to be connected with it.3,6 Estimates that have recently been reported suggest that as many as 75-80% of OSA cases are undiagnosed.9,10 This is especially alarming today with the global rise in obesity and NCDs because of the recognition that undiagnosed and untreated OSA is likely contributing to the severity of other NCDs. Given that OSA is not being adequately addressed, we aimed to evaluate the knowledge and attitudes among physicians about OSA, from a tertiary care hospital in Bangalore, South India, and to understand how it is integrated into their practice of screening and referral for OSA diagnosis and treatment.
METHODS
The study obtained institutional ethics approval from Boston Children’s Hospital. Permission was also obtained from the Group Head of the Department for Clinical Research and Medical Director at the Mazumdar Shaw Medical Center, a unit of Narayana Health located in Bangalore, India. This study incorporated both qualitative and quantitative approaches. A semi-structured interview was conducted with physicians followed by administering a validated and widely used questionnaire termed OSAKA (Obstructive Sleep Apnea Knowledge and Attitudes).11
We had to use a convenient sample based on physician availability, as a random sample of all physicians within the hospital was not feasible. The semi-structured interviews were carried out by a single investigator. The questions asked during the semi-structured interview were designed and validated to compliment the OSAKA questionnaire. These questions were created prior to collecting any OSAKA data from physicians. Prior to official data collection, we simulated the semi-structured interviews with physicians at Narayana Health to ensure the questions were providing face validity. The validation testing informed which questions were asked to each specialist. The data obtained during validation testing were not used in the final analysis. The interview questions have been appended (Online Supplementary Document, Appendix 1).
All of the interviews and the self-administered questionnaire were conducted in English. After obtaining verbal consent, all the interviews were recorded using a voice recorder on a smart phone. The interviews were later transcribed the same day by the investigator who conducted the interviews. Nvivo 12 software for Mac OS was used to code the answers by two investigators using an inductive approach, with the coding based on character count.
The OSAKA questionnaire consists of eighteen knowledge questions, five attitude statements, and basic demographics about the participant. The eighteen knowledge questions cover the following relevant domains: epidemiology, pathophysiology, symptoms, diagnosis, and treatment.11 The attitude statements ask the physician to rate each statement using a 5-point Likert scale; for attitude statements one and two, the choices are not important, somewhat important, important, very important, or extremely important; for attitudes statements three, four and five, the choices are strongly disagree, disagree, neutral, agree, and strongly agree.11 The attitude statements are as follows: (i) As a clinical disorder, obstructive sleep apnea is, (ii) Identifying patients with possible obstructive sleep apnea is, (iii) I feel confident identifying patients at-risk for obstructive sleep apnea, (iv) I am confident in my ability to manage patients with obstructive sleep apnea, and (v) I am confident in my ability to manage patients on CPAP therapy.11
The knowledge score is reported as the number of correct responses out of eighteen (the total possible number of correct responses). The attitude score is reported out of twenty-five (the score from each attitude statement, derived from the 5-point Likert scale, added together). In the end, the individual participants each had an OSAKA knowledge score and an OSAKA attitude score.
RESULTS
During March and April 2018, fifty-four physicians across medical, surgical and anesthesia services were interviewed and administered the OSAKA questionnaire. The demographic details and their mean OSAKA scores are given in Table 1. The qualitative coding using Nvivo 12 software included 74,976 characters and 13,264 words from the fifty-four interviews. The overall unweighted kappa coefficient between the two investigators coding the data was 0.83.
The results of attitude statements one and two showed that all fifty-four physicians in the sample selected a four or five on the 5-point Likert scale (very important or extremely important, respectively) for both of these statements.
The answers to interview question seven (see Online Supplementary Document, Appendix 1) were provided by all fifty-four physicians. The results revealed three critical themes: i) there is poor awareness of OSA among both physicians and patients, ii) OSA is common and increasing, and iii) OSA is grossly underdiagnosed. Twenty-two physicians (40.7%) commented that they believe OSA is underdiagnosed. Twenty-nine physicians (53.7%) commented that the prevalence of OSA is high, common and/or increasing. Twenty-eight physicians (51.9%) commented that OSA is underdiagnosed because physicians, patients or both are unaware of the condition.
Table 2 is a list of relevant quotes that depict the themes mentioned above. It also covers other questions from the interviews. Two additional key themes that emerged and are also conveyed in Table 2 include: 1) agreement that there are currently no standard processes or protocols in place to screen for OSA and 2) a sentiment among physicians that OSA is outside their scope of practice.
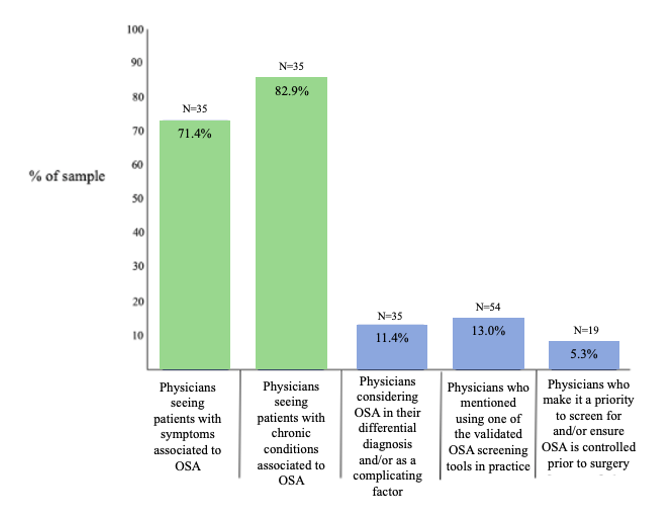
Figure 1 portrays a graphic visualization of the results of interview questions four, five, six, and eight. It also considers the interviews in their entirety to analyze if physicians commented at any point throughout the interview that they utilize validated OSA screening tools. Thirty-five non-perioperative physicians provided answers to interview questions four, five, six B, and six C. The answers to questions four and five revealed that twenty-five physicians (71.4%) were caring for patients with symptoms, and twenty-nine physicians (82.9%) managed comorbidities, strongly associated to OSA. The answers to questions six B and six C revealed that only four physicians (11.4%) were considering OSA in their differential diagnosis and/or as a complicating factor when assessing patients. The results of interview question eight, provided by perioperative specialists, showed that only one physician prioritizes screening for OSA, and/or ensures OSA is controlled, prior to surgery. Additionally, the results of the interviews uncovered that only seven physicians (13.0%) commented that they utilize at least one of the validated OSA screening tools in practice.

DISCUSSION
To our knowledge, this is the first study that utilizes the OSAKA questionnaire in combination with qualitative results from semi-structured interviews with physicians to gain further insight into how knowledge and attitudes about OSA impact clinical care. The mean OSAKA knowledge score across our sample was 12.31 (± 2.7) (Table 1), which is a strong score when analyzing all of the OSAKA studies that have been conducted worldwide (Table 3). Figure 1 shows there is an alarming drop-off in the conversion of this knowledge into practice. Even physicians managing patients with symptoms and/or comorbidities associated to OSA were not screening and referring them for OSA diagnosis and management.
Despite a relatively high knowledge score among the clinicians, it did not influence the clinicians behavior to implement a screening and referral system for OSA in their daily practice. Knowledge and attitudes alone cannot change clinician behavior. Given that OSA is a modifiable risk factor for various NCDs, there is an urgent need to implement better screening and efficient referral systems for treatment and management of OSA.
Our study reveals that physicians expressed several challenges in being able to efficiently screen for patients with OSA. The themes that emerged from the interviews show why it is difficult for them to efficiently screen and refer these patients during their regular practice. For example, one significant barrier is physician daily awareness of this condition. Additionally, there are no standardized OSA screening and referral protocols in place. Interviews also highlighted that there are strong misconceptions among physicians regarding patients who may be at-risk for OSA. This study provides vital information for identifying gaps related to the issue of underdiagnosed OSA. The conclusions reveal that implementation of new hospital policies and protocols across all clinical departments is crucial to convert this knowledge into practice.
India has a very high burden of NCDs and many chronic conditions which are believed to remain undiagnosed in India due to insufficient awareness.21 Research suggests that the level of suspicion for OSA needs to be enhanced among physicians.22 The focus of this study was to not only assess physicians’ knowledge and attitudes about OSA but also to identify if physicians are utilizing their knowledge of OSA during patient interactions. Physicians across the spectrum of clinical specialties are managing and treating patients every day with symptoms and/or chronic conditions that are, or may be, linked to OSA. Therefore, it is critical for all specialists to be regularly thinking about and screening for OSA. This will allow physicians to improve their patients’ other NCDs that they are managing, because clinicians will be able to refer their patients to the appropriate specialist(s) who can treat, manage or surgically correct OSA.23
Attitude statements one and two on the OSAKA questionnaires are particularly relevant for this study, because these statements are related to the importance of OSA as a clinical disorder and the importance of identifying patients at-risk for this condition. The data from these attitude statements underscores that physicians at Narayana Health will likely welcome new hospital-wide policies and protocols that can lead to improved screening for OSA, because these two statements convey that physicians believe OSA is extremely important and that is very important to detect this disorder. The answers to interview question seven provide additional support that physicians will likely be in favor of new strategies being designed and implemented to improve detection, awareness and knowledge of OSA.
It is important to highlight that many physicians think that OSA is outside their scope of practice, because this leads to a diffusion of responsibility. There needs to be continuing education for physicians to teach them about the emerging research regarding the connections between OSA and numerous other NCDs, many of which do fall into the scope of care for physicians who feel that OSA is not within their purview of practice. This continuing education will also help debunk the misconceptions among physicians regarding OSA.
Across the globe, OSA remains underdiagnosed, making studies such as this one paramount for the improvement of screening for OSA; with improved screening will come more efficient diagnosis, treatment and management.1,7 The true prevalence of OSA cannot be accurately estimated until screening and diagnosis are improved worldwide. Improved detection will also enable researchers to better understand the NCDs, and severity of adverse health outcomes, associated with OSA.
The OSAKA scores alone do not provide contextual insight into how physicians are using their knowledge and attitudes of OSA in practice. Therefore, the OSAKA questionnaires were complimented with semi-structured interviews to better understand how knowledge and attitudes are impacting care. This is the first time a mixed-method study such as this one has been conducted and in a middle-income country. The results underscore critical information revealing that OSAKA scores alone are not adequate for determining if physician knowledge is being used on a daily basis. Physicians can be relatively knowledgeable about a topic, yet that information may not be utilized during patient care.
The data in this study provides support for a three-pronged recommendation. Firstly, hospital leadership at Narayana Health, and many institutions alike worldwide, should make it a top priority to implement continuing education to increase knowledge and awareness of OSA among physicians, especially given the growing body of evidence regarding associations between OSA and other NCDs. Secondly, policies and protocols that will create standardized OSA screening and referral across all clinical departments should also be included. Thirdly, a strategic initiative that aims to enhance patient awareness and education about signs and symptoms of OSA is recommended.
Future research needs to be done to help promote awareness and knowledge of OSA among all clinical specialties, especially given the need and growing trend for improved care collaboration across the healthcare spectrum. It is imperative to understand how knowledge is being used in clinical practice to ensure patients are receiving optimal care. As screening and diagnosis continue to improve for OSA, the research analyzing the connections between OSA and other diseases states will be able to provide more conclusive results.
LIMITATIONS
The sampling of physicians for this study consisted of a convenient sample due to time constraints and scheduling rotations of the participating physicians. Ultimately, the sample consisted of a diverse group of specialties and had a similar percentage of female doctors compared to India’s estimated percentage of female allopathic doctors. Out of fifty-four participants, this study included fourteen females (25.9%). As of 2016, India’s percentage of female allopathic doctors was estimated to be 16.8%.24
We acknowledge and understand that the heterogenous sample is a limitation. However, it was by design that we sampled a heterogenous group, because, as we discuss in our paper, OSA falls into the scope of practice for all specialists and needs better attention across the spectrum of specialties. We expected that many clinicians would feel that OSA in not within their purview of practice, which is why we sampled such a diverse group, because we wanted to document this sentiment. Due to scheduling restrictions of the physicians and time commitments of the investigators, we were not able to conduct more interviews during the time period the study took place.
In regard to the attitude statements, we understand that attitude statements 3-5 are not relevant for simply identifying, screening, and referring for OSA. For this reason, we did not focus on these attitude statements in the results section or discussion section. We focused only on attitude statements 1 and 2, because these statements are relevant for screening and referral, regardless of the specialty.
We understand that the lack of standardized screening protocol at this hospital is a limitation. However, this is also what our study was trying to document. We are highlighting that the onus is also on hospital management to identify, create, and implement standardized screening protocols for conditions that are underdiagnosed. We wanted to show that even if the physicians in the hospital are knowledgeable about a topic, hospital leadership cannot expect all of this knowledge to be used effectively on a daily basis. There needs to be better awareness and action taken by leadership to ensure physicians have structured policies to follow to improve patient outcomes.
Acknowledgements:
The study obtained institutional ethics approval from Boston Children’s Hospital. Permission was also obtained from the Group Head of the Department for Clinical Research and Medical Director at the Mazumdar Shaw Medical Center, a unit of Narayana Health located in Bangalore, India.
Funding:
None.
Authorship contributions:
All authors contributed to the draft and final version of the manuscript.
Competing interests:
The authors completed the Unified Competing Interest form at www.icmje.org/coi_disclose.pdf (available upon request from the corresponding author) and declare no conflicts of interest.
Correspondence to:
Alben Sigamani, MD
Narayana Hrudayalaya Foundations
Department of Clinical Research
258/A Bommasandra Industrial Area
Hosur Road, India 560 099
[email protected]