Zimbabwe is one of the countries most affected by human immunodeficiency virus (HIV), with over a million people living with HIV (PLWH).1 Nearly 15% of the adult population are HIV positive.2 In 2018, 90% of PLWH knew their status and 88% had been prescribed treatment1; however, the prevalence of viral load suppression (VLS) among HIV positive adults was only 60.4%.2
Adherence is the extent to which a person’s behaviour corresponds with agreed recommendations from their healthcare professional.3 Persistently high antiretroviral (ART) adherence levels, both in terms of dose frequency and timing,4 are required for VLS and to prevent drug resistance.5 For new ART regimens at least 80% adherence is required; however, 95% or more is needed for older treatments.6 Achieving optimal adherence is one of the most significant challenges in the treatment of HIV in countries across Sub-Saharan Africa (SSA).7 There is little data available on ART adherence rates within Zimbabwe; however, a meta-analysis found that 23% of African patients demonstrate less than 80% adherence.8
Structural, personal and inter-personal factors have been shown to influence ART adherence across SSA.9–11 However, research from High Income Countries (HIC) has also emphasised pre-existing beliefs about illness and medication which influence adherence and health outcomes.12 Researchers have grouped patient beliefs about medication into two themes: 1) necessity of prescribed medication for present and future health and 2) concerns about adverse effects.13 Horne14 proposed a cost-benefit framework to explain how these beliefs influence adherence, in which necessity beliefs are balanced against concerns. If necessity beliefs outweigh concerns, adherence is more likely. This framework has been demonstrated within a variety of illnesses including HIV.15,16 Although the majority of research utilising this framework has been conducted in HIC12 it has been found to be generalisable to SSA.17
Beliefs about ART are one of the greatest predictors of ART adherence.18 To optimise health outcomes, clinics in SSA should design targeted interventions to address these.10 Culturally sensitive interventions can more effectively address beliefs and improve adherence.19 Within SSA, previously identified ART beliefs include concerns about side effects20 and that once you are healthy you can stop taking ART.21 Concerns may also explain why patients use traditional medicines.22 Beliefs about ART should be identified since they impact how medication is taken and/or the amount taken.23 These beliefs may trigger intentional non-adherence (e.g. to avoid side effects) or unintentional non-adherence (e.g. forgetting). Non-adherence may be an ‘informed choice’ and health professionals need to engage and understand the patients’ choices12 to promote effective shared decision making.
Barriers and facilitators to ART have been explored in both rural24 and urban Zimbabwe.25 However, no prior studies have explored specific beliefs of PLWH towards ART. A detailed assessment of factors influencing patients’ attitudes towards treatment in this setting is essential to develop appropriate adherence interventions. The aim of the study was to explore medication beliefs among PLWH in Zimbabwe.
METHODS
Study Setting
This study was carried out between June and July 2014 at Parirenyatwa Hospital Family Care Centre [PHFCC] in Harare, Zimbabwe. PHFCC is publicly funded, receiving resources from the Zimbabwean Ministry of Health and Child Care. All HIV medications are provided to patients without cost. Medical evaluations, including CD4 and viral load, are also provided free of charge. The clinic provides care for approximately 3000 adults and 1000 children.26
Study Design and Sample
Qualitative methodology was utilised whose goal, unlike quantitative research, is not to generalise the results to the target population, but instead, to showcase a rich, contextualised understanding of the human behaviour being studied.27 Twenty-one in-depth semi-structured interviews were carried out with adult PLWH (≥18 years old) who had been prescribed ART for at least one month. Two healthcare professionals at the clinic were also interviewed: a peer counsellor and a clinical psychologist.
Participants were recruited using maximum variation purposive sampling for gender, age, and treatment line. This method intentionally selects a wide variety of participants to get a balanced view of the construct being studied.28 The healthcare professionals selected were individuals who were familiar with the psychosocial, economic and cultural influences affecting patients at the clinic.
Ethical Considerations
Written informed consent was obtained from every participant. If any non-adherence was reported, the participants were referred for more detailed assessment within the PHFCC. Ethical approval was obtained from: Research Council of Zimbabwe, Medical Research Council of Zimbabwe (MRCZ/A/1736), the Joint Research and Ethics Committee of the University of Zimbabwe (18/13), and the Research Ethics Office of King’s College London (PNM/11/12-147).
Data Collection
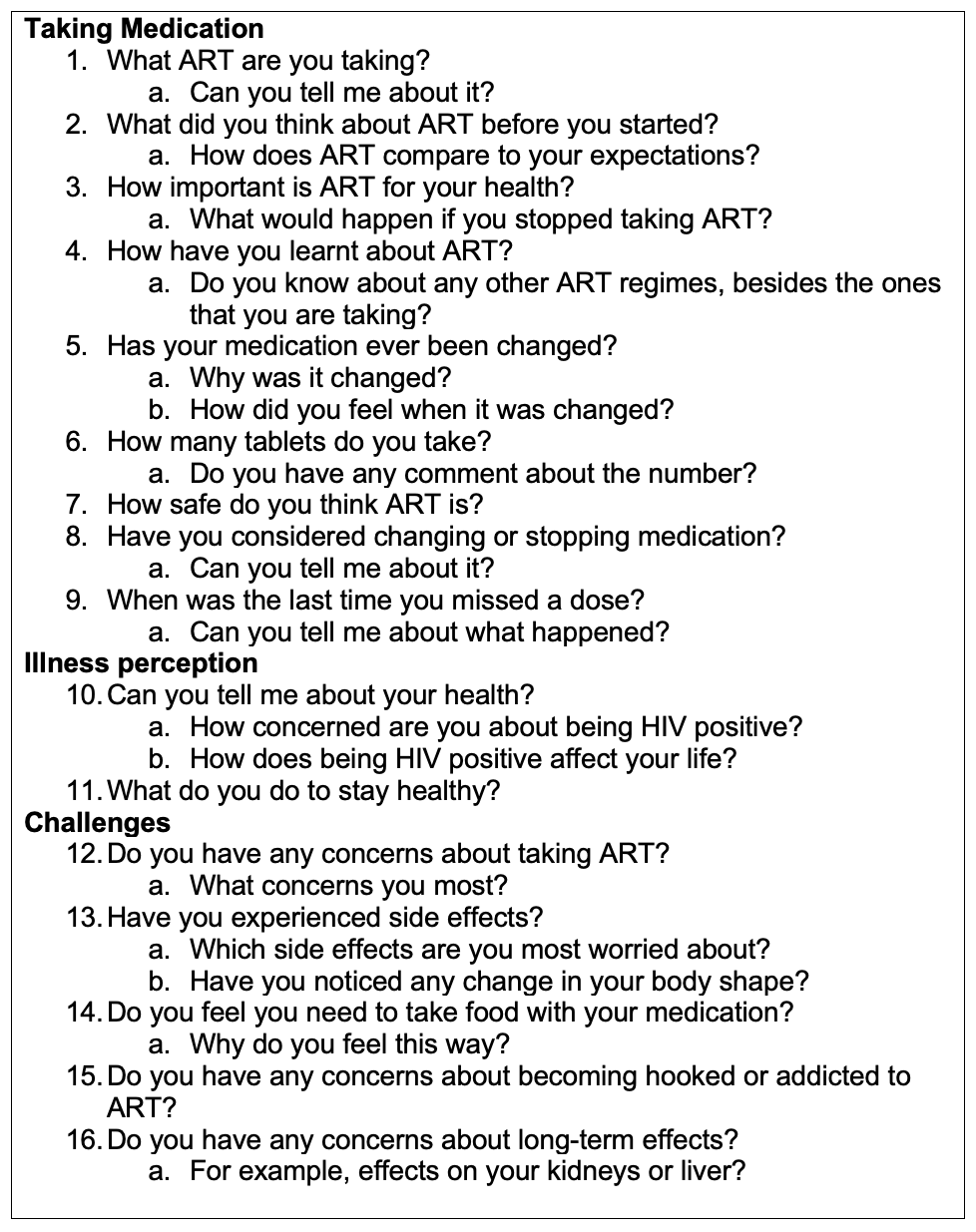
The English interview guide (see Figure 1) was translated into Shona and back-translated by a fluent speaker to confirm precision and clarity.

There were three female interviewers who all had previous training in qualitative methodology. Via an iterative process, the guide was edited to ensure conversations were fluid, questions remained open-ended, and concepts were culturally appropriate. The interviewers used the guide to speak to participants about their experiences of ART, including factors that facilitated and impeded adherence. The guide was adapted for the healthcare professionals to focus on cultural and contextual factors that impact ART adherence and their experiences of non-adherent patients.
Each interview was audio recorded, which was transcribed verbatim. Transcripts were compared with initial recordings for precision. The five Shona interviews were translated into English prior to analysis. Interviewers used elements of grounded theory for data gathering by examining emerging themes.29 Interviewers discussed major themes and appropriateness of the guide with the senior researcher. These meetings enabled iterative modifications to the guide throughout data collection and helped ascertain when theoretical saturation was achieved, after which no further interviews were conducted.30 Saturation is when no new information or new themes arise from the data.31 Within qualitative research within a relatively homogenous population, theoretical saturation can occur within samples of 12 participants.32 The duration of the interviews was 45 to 60 minutes (mean 50 minutes).
Data Analysis
Three researchers reviewed two transcripts each and reconciled codes, producing 28 initial codes. Subsequent line-by-line open coding was completed of each transcript using NVivo 10 (QRS International, Burlington MA, USA).
Axial coding was performed,29 sorting codes into categories and determining how these were interconnected. Selective coding allowed the researchers to assemble ideas from the data to form a descriptive model of beliefs about ART.29 The coding tree (see Table 1) illustrates the process of developing and refining codes. Major themes of the descriptive model are demonstrated using key quotations in the results.
RESULTS
Participants
Nine participants were female (42.9%). Ages ranged from 24 to 66 years (Mean = 43.5 [SD =11.4] (1 missing)). Eleven participants were on first line treatment (52.4%)(1 missing) (see Table 2).
Themes
Emerging themes pertaining to ART beliefs have been categorized into two groups: medication importance and medication concerns (see Table 3).
Theme 1: Medication importance
How important ART was perceived as being for the participants’ heath affected their medication-taking behaviour. Adherence was dependent on how necessary the participants believed ART was for their health. When participants perceived ART to be dispensable, alternative treatments were used, instead of or in combination with biomedical treatment. The majority of participants believed in the efficacy of ART so would take a dose late to avoid missing it.
Necessity of ART
The majority believed ART was necessary for their current and future health. ART enabled them to work and care for their families. Without medication they worried about their health worsening. ART became part of participants’ daily routine enabling them to lead a normal, healthy life:
“They are very important because I can lead a normal life without any worry that if I get, I mean if I feel ill, I don’t think that I maybe am getting onto the AIDS stage” (PID11, Male, 62 years).
Personal positive experiences of taking ART caused participants to believe in the necessity of the treatment; however, observing others’ experiences also reinforced this. By observing others not taking ART and its negative impact the participants strongly associated positive health with ART:
“They are very important because I have seen for myself…I knew a lot of people who got infected, some of them they didn’t bother to go for treatment, and most of them have passed away” (PID9, Male, 63 years).
Perceived Alternative Treatments to ART
Alternative treatment, particularly herbal remedies, were used when ART was not seen as necessary to treat HIV; however, few participants reported using these. Participants noted that using herbs was more common in rural areas. Alternative therapies were often not used in conjunction with, but instead of, ART. Observing others’ experiences with alternative treatments also reinforced how important ART was to their own lives:
“I’ve seen people saying they don’t want to go and take medication, they want to go herbal. Herbal is more or less saying you’re not taking your medication. After 1 year I’ve seen them worse than me. After 2, 3, 4 months they’re probably dead” (PID19, Male, 42 years).
Herbal remedies (e.g. the Moringa tree and Mubvamaropa plant) were promoted by traditional healers. Depending upon how important ART was perceived as being, the herbal remedies were used either in addition to ART or in place of biomedical medicine:
"My mother has a Moringa tree. It doesn’t cure AIDS, but maybe it reduces the viral load. People come to collect the beans and the leaves. There are some people in the village who have used it, they use it in addition [to ART]" (PID11, Male, 62 years).
Avoid Skipping a Dose
ART was seen as important for health so when participants were unable to take a dose on time the majority would take their pills as soon as possible:
"“But say I forget to take them at 10, I always compensate by maybe 12, 1 o’clock” (PID19, Male, 42 years).
Participants would rather take their medication late, even by hours, than miss a dose. Certain participants would even take their dose early to prevent missing one:
“I may be travelling on a bus, and I have planned to take my medication at 8 so I end up resolving to just take them at 7 so that I travel safely. That means I will have taken them earlier by one hour because it will be difficult to start unpacking my things looking for medication” (PID6, Female, 42 years).
Theme 2: Medication concerns
Regardless of how necessary ART was perceived as, participants had multiple concerns about their medication. Participants were apprehensive regarding the impact and safety of ART including: short and long term effects of the medication; number of doses; the fact there is no long lasting ART regimen; potential interactions with other medications; ART may not work or be as effective without food; and fear of stigma of taking ART in public. In some cases, these concerns negatively impacted self-reported ART adherence behaviour, thus decreasing the therapeutic impact of the medication. At other times, participants tried to adhere due to the perceived benefits of ART.
Side Effects
Almost all participants experienced ART side effects including: palpitations; hallucinations; dizziness; vomiting; drowsiness; insomnia; weight changes; headaches; forgetfulness; difficulty walking; pain; and numbness. The impact these had on participants’ lives varied depending on the severity of the symptoms; however, some participants found it difficult to cope:
"Because how am I going to live with these problems? That I can’t do anything and I’m always feeling painful" (PID3, Male, 66 years).
Some participants found it difficult to maintain good adherence when side effects were debilitating and they were unable to undertake normal daily tasks. Participants would avoid the side effects by delaying, skipping or stopping treatment:
"I wouldn’t be able to drive say after 30 minutes once the medication starts taking effect. So, I would delay taking the medication" (PID1, Female, 38 years).
For some participants, side effects did not impact them to the same extent over time:
"but with time I got used to it" (PID 12, Male, 40 years).
Other participants discussed side effects with healthcare professionals who changed their treatment regime, removing the debilitating side effects.
Worries about Long term effects of ART
Participants worried about the long-term impact of treatment, particularly on their liver or kidneys. Some participants felt their body would be unable to cope with the medication for years:
"… because it [your body] cannot handle five tablets every day for the next 10 years" (PID19, Male, 42 years).
However, this did not seem to negatively impact self-reported adherence.
Pill Burden
ART must be taken every day to be effective and participants discussed the number of pills that would be acceptable. There were differing opinions, but generally participants preferred a lower pill burden:
"They are too many. If they could be reduced it would be a huge relief" (PID2, Male, age unknown).
Participants became overwhelmed and stressed trying to ensure they take their pills every day:
"I was just so stressed every time I took the tablets, there were just too many for me. So, I was just reluctant to take them" (PID21, Female, 36 years).
This led to some participants skipping or delaying medication; however, the majority noted that they tried to adhere as required.
Desire for a Longer Lasting Treatment Regimen
Participants indicated the positive impact a long-lasting regimen would have on their lives, describing more time and money if they did not have to attend the clinic regularly for drug pick up or check-ups:
“ART should be improved in a way that you don’t have to take them regularly, but over a certain period of time. You take them maybe once in six months or maybe once in a year…then it would become much better. It would save me a lot of money to come up here to collect the tablets and have medical check-ups and all that” (PID11, Male, 62 years).
The strong desire for long lasting treatment was indicated by rumours regarding ‘cures’ which were widely discussed in the waiting room:
“I heard in United Kingdom, you take one tablet in three months. I don’t know where we get it, but it would help us to reduce time and adherence…if I take one in three months it’s easier than to take every day” (PID17, Female, 42 years).
This spread of erroneous information could potentially jeopardise continued ART adherence. PLWH may become frustrated they do not have access to a longer lasting treatment regimen which in turn may impact their medication-taking behaviour or they may misunderstand and believe their regimen does not need to be taken every day.
Concerns about Possible Drug interactions
Some participants raised concerns about the interaction of ART with other drugs. Participants worried about one treatment cancelling the effect of others:
"I worry. I just think maybe if the tablets mix, it might mean that one disaffects the other" (PID9, Male, 63 years).
Participants indicated ART was more important than other medications they were prescribed. They noted they would take the non-ART drug only when absolutely necessary or they would not take it at all:
"I take my asthma tablets only when my asthma is high, otherwise I leave them" (PID20, Male, 38 years).
Perceived need for food
The majority of participants believed they had to take ART with food. Participants were concerned that taking ART without food would worsen side effects, and the medication would not be as effective or not work at all. Some were advised by health providers to take ART after food whereas others decided to follow this guidance from their own experience, particularly due to the worsening side effects:
“If I didn’t take food later on … there would be heat and the hallucinations would intensify” (PID1, Female, 38 years).
Food was seen as imperative to ensure medication worked for some participants:
“Because you don’t eat, the drug will not be useful for my health. It don’t work [without food]” (PID14, Male, 43 years).
These beliefs may negatively impact adherence since if a participant does not have food available, they may not take their medication on time.
Desire to Avoid Perceived Stigma
Participants worried about stigma and discrimination which affected the settings in which they would take their medication. Some participants were embarrassed about taking ART in front of others:
“Because I don’t want people to know my status, because at times their comments are upsetting and you end up being stressed. It also affects your working environment as well as your social life” (PID2, Male, age unknown).
Participants avoided taking medication in public and preferred taking it at home:
"I only [take medication] out of home if like I am on a trip or anything (PID9, Male, 63 years).
Participants noted that funerals were particularly difficult settings in which to maintain good adherence:
"You find that in our culture, death and funerals are a big thing. You have to attend funerals, and when you do you are sitting in one room with everyone. So, a lot of people will not take their medication because they will not want people seeing them taking their ART. You spend like three nights before someone is buried. The women will just be in one room and the guys will be, maybe outside by the fire. So, there is nothing private about that. If you have to take your medication, you have to take it there. They will not take their medications when they go for funerals" (Clinical psychologist).
Some participants, however, found they became more comfortable taking medication in public over time:
“I don’t feel embarrassed. I used to, but not now. I just used to feel a kind of like, I was not settled. I used to hide when taking ART” (PID12, Male, 40 years).
DISCUSSION
This was the first study in Zimbabwe to describe beliefs about ART and HIV treatments and how context-relevant necessity beliefs and concerns affect self-reported ART adherence. The data was analysed using grounded-theory framework; however, nonetheless the codes and themes are reflective of the Necessity-Concerns Framework (NCF).14 The NCF has been shown to be a useful model for understanding patients’ evaluations of their prescribed medications across different conditions, medications and settings; however, it has been predominantly developed in the UK and studied in Western countries.12,33,34 The results provide support for this framework to be utilised within Zimbabwe and potentially within SSA. The majority of participants thought ART was necessary for their health and regardless of concerns they would try to adhere. Although, in certain situations, when concerns heavily impacted their life (e.g. severe side effects) they would skip, delay or stop treatment. The results also provide implications for healthcare settings. Healthcare professionals have to discuss these context-relevant beliefs about ART with their patients to promote ART adherence.
In Zimbabwe, knowledge of HIV has grown since the epidemic started and recent research suggests fewer people now use traditional medicines.35 However, the current study indicates this is still an issue particularly in rural areas. Participants indicated although some PLWH take traditional medicine in conjunction with ART there are still those who take it instead of biomedical treatment. Previous research has indicated it is important to understand why PLWH choose alternative treatments to ART.36 Building collaborative relationships between traditional practitioners and health systems is key to scaling up comprehensive HIV care throughout SSA.37 In Zimbabwe, there are 45,000 registered traditional healers compared to 1,400 doctors.38 Future research and policy need to focus on ensuring collaboration.
Many participants were worried about stigma so avoided taking their medication in public, affecting adherence. Funerals, in particular, were suggested to have an impact. In a study in rural Zimbabwe,39 nursing staff indicated attending funerals was a reason patients did not collect ART on time. Attending social engagements is also a barrier to ART adherence in other SSA countries.40 Healthcare professionals should specifically mention this context when discussing stigma. Healthcare professionals should also discuss problem solving around how to take the medication in that situation.
Most participants took medication late if necessary, but participants did not seem to have clear guidance. Patients have different opinions about when to take medication40 and patients and clinicians differ in their understanding of the term “missed dose.”41 Healthcare professionals need to ensure these guidelines are discussed and are clearly understood. Additionally, healthcare professionals need to provide clear guidance on whether PLWH are able to take ART alongside food and provide problem-solving around managing possible side-effects of the medication.
This study adds important new insights into how patients view ART adherence and how beliefs about ART impact this. In particular, the study identified a concern, not often highlighted in the literature. Patients were concerned about the possible drug interactions when mixing ART and medication for other illnesses. Patients seem to value ART over other medication; however, healthcare professionals need to be aware of these concerns to ensure patients clearly understand when they can take medications together.
These views alongside other interviews with non-adherent and depressed patients42 were utilised to help culturally adapt an adherence and depression intervention in Zimbabwe. The themes were used to help train adherence counsellors about the beliefs and personal experiences of patients, to ensure they understood what information is required to help support patients adhere to their medication.43 Additionally, the results of this study was utilised to develop a barriers measure to ART adherence for people living with HIV in Zimbabwe.44
This study had some limitations. Patients no longer remaining in care or with poor adherence to appointments should have been interviewed to explore all perspectives. The study was only conducted in a single HIV clinic, which did service patients from rural and urban areas, however, it would be beneficial to interview participants from other locations in Zimbabwe, particularly rural, to gain an insight into any potential differences. Previous research in Zimbabwe has indicated patients worry about negative treatment and want to appear as a “good patient” to professionals.45 This fear may have biased results since patients do not want to show signs of non-adherence. To minimize this bias, interviews were conducted in a private location and it was made clear that this study had no effect on participants’ care.
CONCLUSIONS
Every patient has a unique perspective when taking ART. Healthcare professionals need to understand and take these into account for each patient.46 The results indicate the necessity for healthcare professionals to discuss patients’ beliefs about ART to ensure these do not negatively impact adherence. In particular, concerns about medication should be identified and reviewed. By removing or reducing concerns, patients are more likely to adhere to ART.47 These beliefs also need to be utilised by researchers to develop culturally relevant adherence interventions. Health professionals must be aware of the beliefs patients hold regarding ART and ensure they provide a platform for patients to discuss these with them.
Acknowledgements
We would like to thank all the participants who took part in this study and the healthcare professionals at the clinic for their assistance.
Funding
NIH Research Grant 1R21MH094156-01 funded by the National Institute of Mental Health
Authors’ contributions
K.K, L.P, D.M, and P.M. performed the research. N.C, M.A and L.D.H designed the research study. T.B and D.C contributed essential insight. N.C, L.P and K.K analysed the data. N.C. and L.P wrote the paper. All authors have read and approved the manuscript.
Competing interests
The authors completed the Unified Competing Interest form at www.icmje.org/coi_disclosure.pdf (available upon request from the corresponding author), and declare no conflicts of interest.
Correspondence to:
Natasha Croome
Institute of Psychiatry, Psychology and Neuroscience
King’s College London
De Crespigny Park
London
SE5 8AF
+44 1372 815007
[email protected]