



Diagnostic medical sonography is a noninvasive diagnostic imaging modality used in diagnosing disease of almost all the body organs and progressively plays an indispensable role in major clinical decisions about patient management. The use of ultrasound imaging forms an integral part of health care in developed countries and is increasingly available in developing countries because of its good visualization characteristics and relatively easy availability, accessibility, and affordability.1–3
Ultrasound technology was adopted for clinical use in the 1950s, and since then, it has become the fastest-growing diagnostic imaging modality. It is now the second most commonly requested imaging procedure.3,4 The application of ultrasound imaging modality in clinical practice was initially the preserve of Medical Practitioners.5–7 However, with the advancement of clinical need, other health professionals of varying backgrounds perform the scans, and it became known as ‘sonography’ taken after the ‘radiographer,’ which describes the x-ray technician.7
The evolution of sonography practice in Ghana has taken a similar trajectory, and there has been a rapidly increasing application of ultrasound in medicine in the last two decades.8 Despite this, there remains a lack of rigorous regulation that governs the practicing of sonography. Many healthcare practitioners have undergone training to obtain the skills to become safe and competent sonographers in Ghana, albeit they are few. However, the current lack of regulation of this area of healthcare practice, coupled with the high numbers of sonographic examinations requests and the limited numbers of qualified sonographers, have led to a situation where unlicensed sonographers have virtually taken over the profession.
Unauthorized health practitioners have long been a problem of the health care system around the world. The predominant victims of quacks cannot afford the expensive clinics patronized by the elite, coupled with the state’s inability to regulate these unbridled activities of these unlicensed professionals who run a parallel health care system in the country. The Ghana Association of Medical Laboratory Scientists reported that unauthorized medical laboratory practitioners caused many Ghanaians’ death attributable to the wrong diagnosis from these illegal laboratory scientists leading to wrong prescriptions.9 Many Ghanaian communities have experience with ultrasound technology due to its high application in especially antenatal care10, increasing liver and prostate conditions among middle-aged men, and a too high number of unindicated requests for ultrasound examinations from health professionals.11,12
The application of diagnostic sonography in current healthcare delivery in Ghana is not immune to unlicensed sonographers who take advantage of helpless patients. Moreover, many referring clinicians have no option but refer their clients to access ultrasound imaging and reports from these unlicensed sonographers, which possibly undermines the quality of care and rational utilization of the ultrasound technology. It is also worth noting that some government and privately owned hospitals and diagnostic centers eengage the services of these quack sonographers. However, limited knowledge exists about the quality of training of these unlicensed Sonographers, their educational background, their sonographic competence, and whether the existing regulatory system captures how their activities impact healthcare delivery in Ghana.
Ultrasound education in the United States is a direct entry program. There is a one-year certificate program for applicants with qualifications in a related allied health profession and a two-year program for high school diploma courses in basic science, general physics, and algebra.13
Medical ultrasound in the United Kingdom (UK) is at the postgraduate level, with most sonographers entering the field with a health background. The precise pathway for sonographers is an undergraduate degree in nursing, midwifery, or radiography followed by practical experience as a qualified staff member before the individual joins a postgraduate program to undertake their ultrasound training.14,15
Besides, being a graduate of a sonography school in the United States does not automatically have the certification or registration. Registered Diagnostic Medical Sonographer (RDMS) credential is a requirement in addition to graduating from ultrasound school. The demonstration and maintenance of competency through certification by a nationally recognized sonography credentialing organization is standard practice.13
The route to professional ultrasound certification and registration in Ghana is long and limited. The first Ghanaian tertiary institution was accredited in the year 2009 to commence the training of professional diagnostic medical sonographers, and they have been graduating an average of 35 Medical Sonographers since 2013. The second University to start accredited medical sonographers’ training is the University of Cape Coast, Ghana, and the first cohort of 40 trained sonographers shall graduate in the year 2020. These four-year sonography programmes’ entry requirements are similar and include a senior high school certificate with at least credits in any three core courses and any three elective courses, including Physics, Chemistry, Biology, and Elective Mathematics. The University of Ghana, Legon, also offers a postgraduate programme in diagnostic sonography, and the entry requirement is similar to that of the UK. They usually graduate an average of 10 students yearly. All these diagnostic medical sonography programs have accreditation by the National Accreditation Board (NAB), Ghana.16
By law in Ghana, all allied health professionals adequately trained in an accredited institution must register with the regulatory body and practice in only accredited health facilities.
The Allied Health Professions Council (AHPC) is the body established by the Health Professions Regulatory Bodies Act, 2013, Act 857, to regulate the training and practice of Allied Health Professions in Ghana. As part of its mandate, the Council is responsible for granting Professional Accreditation for all Allied Health Academic Programmes. The Council’s main objective is to ensure the highest standard among allied health professionals in Ghana.17 The Health Facilities Regulatory Agency (HeFRA) was established in 2011 by an Act of Parliament, Act 829. Their mandate is to license and monitor physical facilities for public and private health care services.18 The Agency’s mission is to transform healthcare facilities’ regulation through quality standard-setting, enforcement, and client-focused partnerships.
However, there is a lot more room for these regulatory authorities to improve to achieve the goals for which they were set up by law. Ghana has several sonographers trained through unaccredited means including health facilities and diagnostic centers operating without the required facility licensure.
Quack sonographers mostly operate in the periphery and at diagnostic centers, clinics, and hospitals in urban and rural areas taking advantage of the lacunae in the healthcare regulatory system. It is worthy of note that most private and government health facilities in Ghana engage the services of unlicensed medical sonographers due to an overflow of referrals for ultrasound examinations, shortage of registered Sonographers, and the noninvasive nature of some of the ultrasound scanning procedures.
Therefore, why the government of Ghana, with all its resources and with all the promulgated regulatory laws, can not ensure proper health care and health information for its citizens? Why is it that the government can not take a stern look at the unwarranted deaths and health hazards resulting from illegal health professionals and start proffering solutions?
To the best of our knowledge, there has not been any comprehensive study done in Ghana on the scale of unlicensed Medical Sonographers and their unbridled ultrasound scanning activities along the country’s length and breadth. It is also imperative to elicit as a country, the attendant health hazards, and the socio-economic ramifications of this precarious situation.
Therefore, we decided to carry out a qualitative study across the country and at multiple health facilities to evaluate the ubiquity of unlicensed sonographers’ practice of ultrasound and provide an in-depth description of the health menace and clinical implications to the health of the ordinary people in Ghana.
METHODS
Study area
This study was a qualitative study using well-structured pretested questionnaires administered to unlicensed sonographers who had registered in a tertiary institution as a cohort of matured students admitted for a Bachelor of Science degree programme in medical sonography. We relied on these unlicensed sonographers who had registered in the tertiary institution for further studies in ultrasonography to contact many of their unlicensed colleagues who practice across the whole country.
Study population
Survey methodology was employed to recruit 207 potential participants. The participants were all unlicensed medical Sonographers practicing sonography across all the 16 regions of Ghana. None of the participants have been licensed by the Allied Health Professions Council (AHPC) to practice sonography in the country. As many of the cohort of unlicensed sonographers, we contacted and were inclined to participate in the study formed our sample size.
Study design
The study was a qualitative study with the use of well-structured pretested questionnaires administered to participants. We also collated Sonographic Reports emanating from multiple unlicensed sonographers. These are reports given to referred patients to the tertiaryA hospital for further management. These reports were carefully analyzed by Specialists, including but not limited to, Radiologists, Obstetricians, Gynaecologists, and Surgeons.
The pretested questionnaires were self-administered to investigate the scale and scope of practice of the unlicensed medical sonographers. The following specific objectives were conceived to determine the:
-
Demographic characteristics of unlicensed sonography practitioners.
-
Distribution of unlicensed sonographers across the country.
-
Source, method, form, and duration of sonography training of the unlicensed sonographers.
-
Types of sonographic investigations and the competence of the unlicensed sonographers.
-
Degree of use of social media and other external technological support in their practice.
-
Perception of participants on the regulation of the sonography profession.
-
Competence of sonographers determined from the quality of collated sonographic reports analyzed over a period.
Inclusion criteria
The study was confined to unlicensed sonographers in the health care delivery system in Ghana. All medical sonography practitioners not licensed with the AHPC were eligible to be included in the study.
Exclusion criteria
All practicing medical sonographers who are properly licensed and registered with the AHPC.
Data collection and analysis
Data was collected by way of multiple techniques. A structured questionnaire was used to collect information on demographic characteristics, type of sonography training received, and general information on the practice of sonography. The non-participant observation used to assess the reports emanating from unlicensed sonographers of referred patients brought to clinicians at a tertiary hospital were collated.
The data obtained were entered and analyzed using the IBM Statistical Package for Social Science (SPSS v.23.0 software). Proportions presented for categorical variables using frequencies, percentages, and Chi-square where appropriate. A P-value of <0.05 was considered statistically significant. The results are presented in appropriate tables and charts.
Ethical clearance
Ethical clearance and permission to undertake the study was obtained from the Cape Coast Teaching Hospital Ethical Review Committee (Reference number: CCTHERC/EC/2018/030).
Written informed consent was obtained from each participant before the administration of the questionnaire. Participants were assured of confidentiality and informed that participation in the study was voluntary.
RESULTS
A total of 207 unlicensed sonographers were recruited for the study. The results showed 90% (186) response rates out of which 128 (69%) were males and 58 (31%) were females.
Demographic characteristics of respondents
The participants’ age distribution results, the type and level of education, and any prior vocational training are depicted in Table 1.
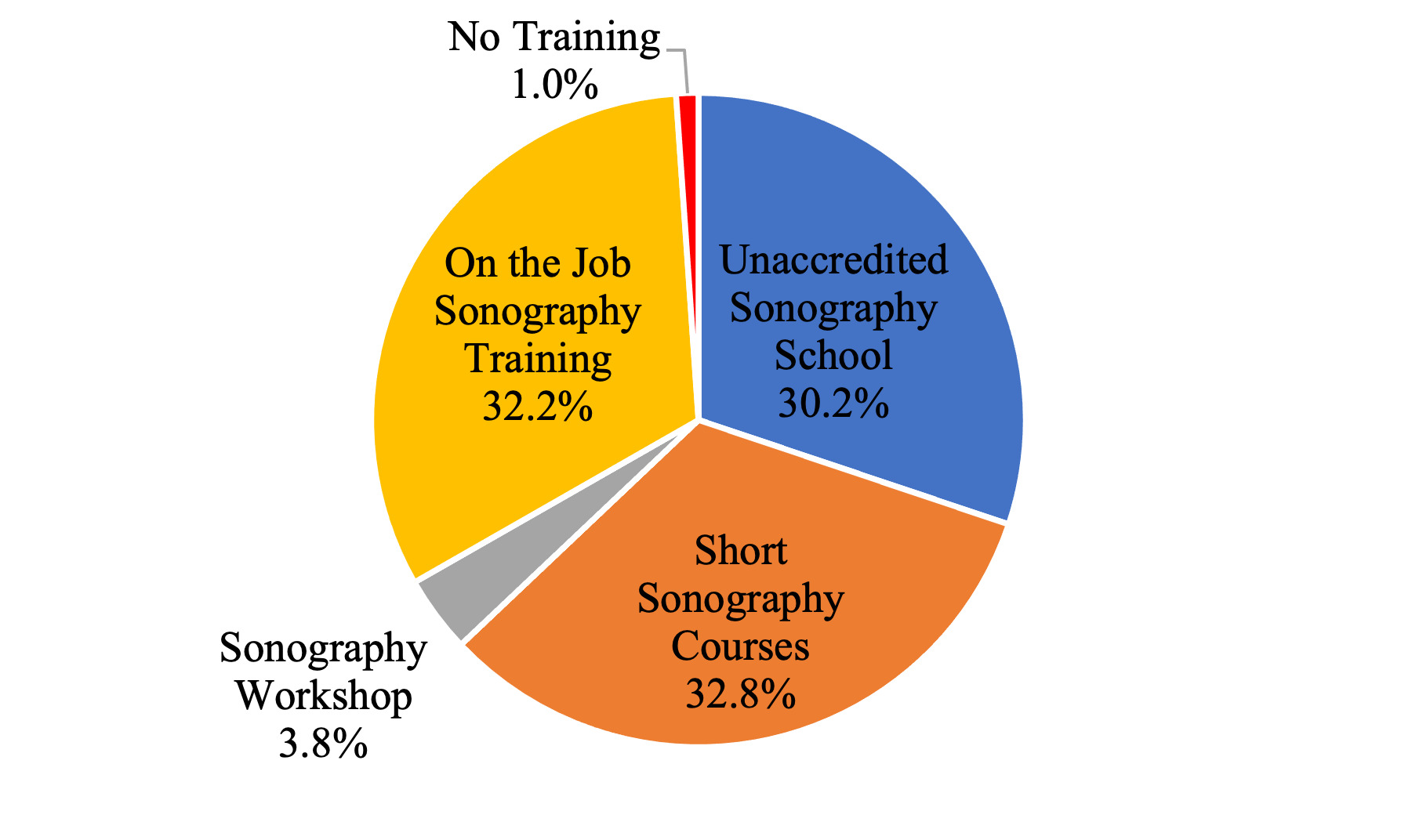
Mode of acquisition of sonography training
The mode by which these unlicensed sonographers were introduced to the sonography profession and received training is illustrated in Figure 1.
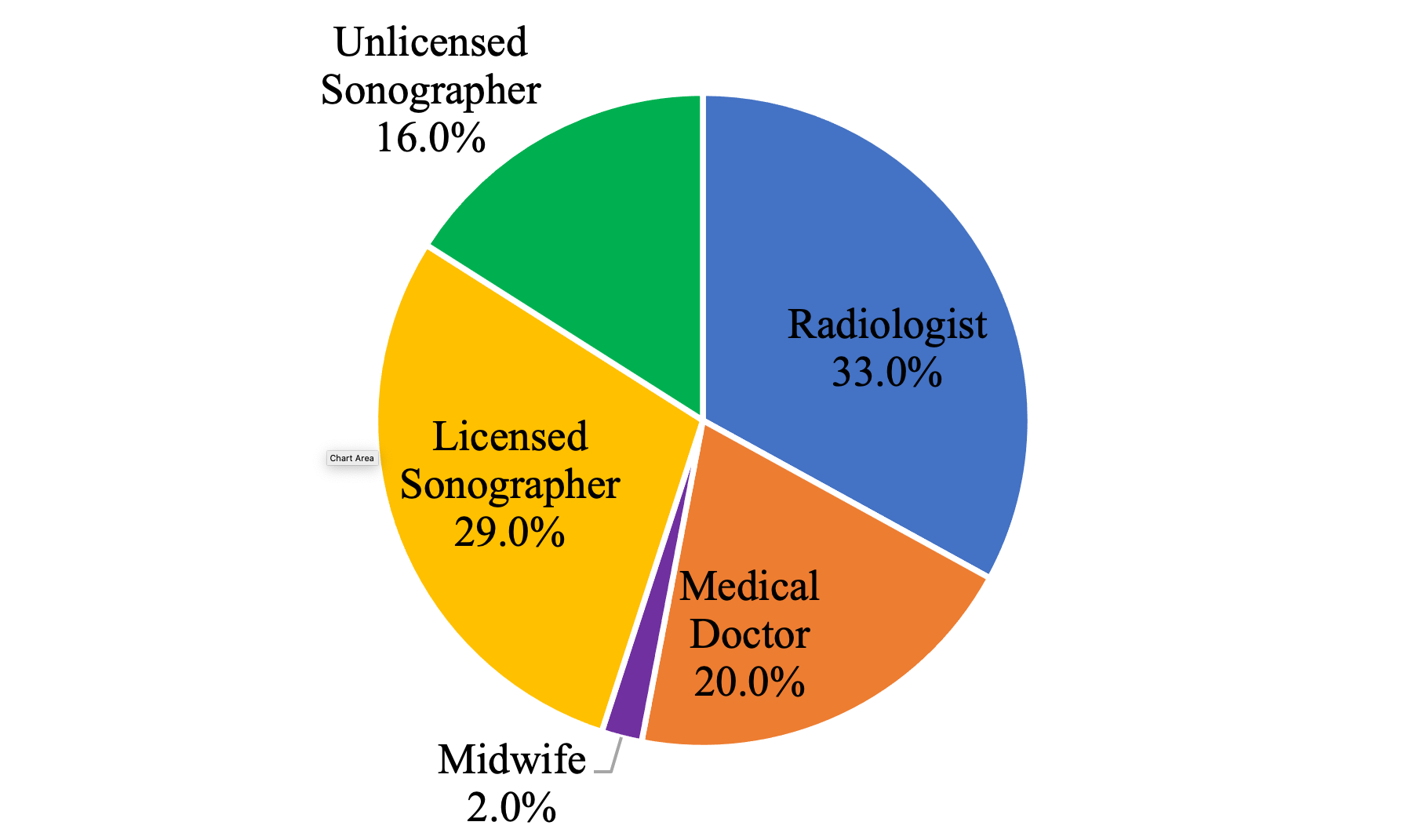
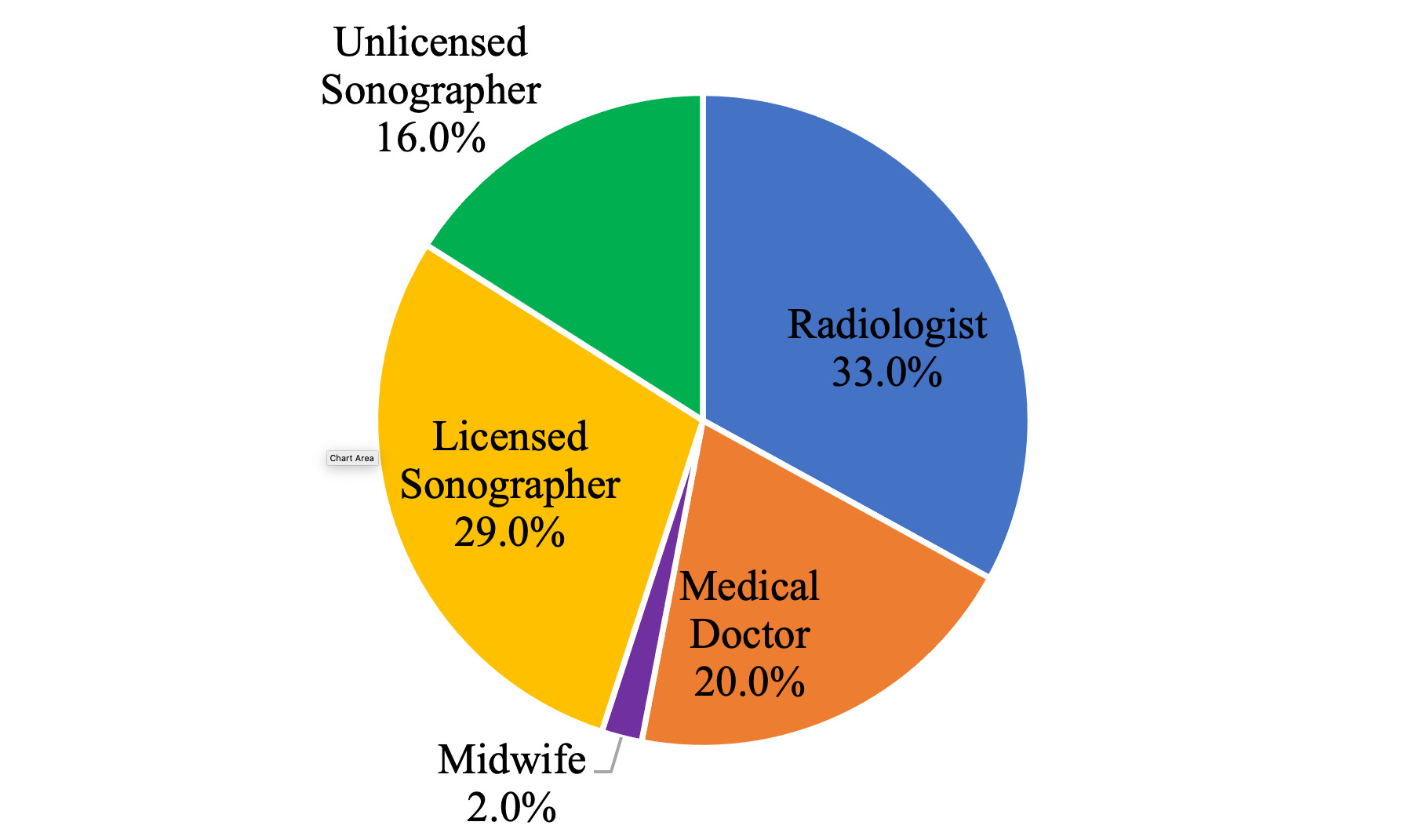
Person responsible for sonography training
The individual responsible for these unlicensed sonographers’ training and introduced them to the sonography profession is illustrated in Figure 2.
Duration of training and how soon sonography practice started after training
We tried to elicit the duration respondents received sonography training and how soon they started practicing after the training. The results are shown in Figure 3.

How long has respondent been practicing sonography?
We further analyzed the period that respondents have been practicing sonography, and the result is illustrated in Figure 4.

Distribution of educational level and mode of acquisition of sonography training
Furthermore, we evaluated the distribution of respondents’ educational level and mode of acquisition of sonography training. Three main educational backgrounds were identified: senior high school (SHS), Tertiary, and Technical. The results are presented in Table 2.
Distribution of workplace and ownership of facility
Analysis of their current workplace and ownership structure (inset) of ultrasound diagnostic facilities across the country is illustrated in Figure 5.
_of_facility.png)
Respondents perception on practice and regulation of sonography
Table three summarizes respondents’ perceptions on the subject of regulation and control of sonography practice in Ghana.
Result of analysis of collated sonographic reports
Specialist Radiologists, Obstetrics and Gynaecologists, and Surgeons carefully analyzed collated sonographic reports emanating from several unlicensed sonographers from several sources. The results showed a severe lack of expected level of competence. The reports were analyzed for form, content, and clinical diagnosis compared to the referred patient’s clinical findings upon examination. Out of 1,643 reports collated and analyzed, 36.4% were competently written, and the pathology was accurately appreciated. The breakdown of the collated and analyzed reports are shown in Table 4.
DISCUSSION
This study, to our knowledge, documents for the first time and evaluates the degree and ubiquity of quacks practice of sonography in Ghana. The role of sonography in the diagnosis of diseases is well established in clinical practice. However, there are no strict regulations and enforcement to moderate medical ultrasonography in Ghana, a developing and resource-challenged country.
In this study, we assessed the penchant of unlicensed individuals to practice medical sonography. Furthermore, our study also allowed us to analyze data from across the country. The availability and accessibility of Ghanaians to ultrasound diagnosis and the probability of being exposed to an unlicensed sonographer performing the scan is high. Therefore, we decided to evaluate the universality, socio-economic burden, and the associated health hazards of the continuous ultrasound application by these unlicensed practitioners to diagnose disease.
As a developing country, Ghana has very few health professionals, which is the general trend in Africa.19 The Ghana Society of Radiographers (GSR) is the umbrella association for all registered radiographers and medical sonographers in Ghana. The GSR has only 334 registered members for over 30 million people. This regrettable situation is partly due to the woefully inadequate medical sonography training institutions in the country. Therefore, there is a considerable lacuna that invigorates unlicensed sonographers to thrive.20–22
A total of 186 unlicensed sonographers responded with 69% males and 31% females, and they practice at 11 out of the 16 regions of Ghana. It is worthy of note that 70.6% are practicing in the country’s two most populous regions: the Greater Accra (38.4%) and Ashanti regions (32.2%) of Ghana.
As can be inferred from (Table 1), all respondents belong to the working-class age23, but most (54.0%) had no profession before engaging in sonography practice. It is quite apparent that working-class age individuals who lack any professional training will engage in any income generation activity where there is apathy on enforcement agencies. It is also significant to note that respondents with other professional educational backgrounds opted for medical sonography practice because it was deemed a more rewarding endeavor.
The majority (88.2%) of respondents have Senior High School (SHS) or tertiary education before being introduced to the sonography profession. The minimum requirement of entry into an accredited medical sonography program is the SHS level of education.16 It shows that if students had been informed on the medical sonography profession earlier and more accredited sonography training schools were available, they could have opted for professional training and got adequately licensed. The awareness of SHS graduates about the radiography and sonography professions is low, as found in a study.24 Therefore, there is a need for more enlightenment of SHS students about the medical imaging profession.
The study identified four significant pathways (Figure 1) for the proliferation of unlicensed sonographic workforce in Ghana. The majority (95.2%) were trained by attending sonography short courses (32.8%), Peer-to-peer hands-on training (32.2%), and unaccredited training schools (30.2%) played a vital role in the creation of unlicensed sonographers. As can be elicited from (Figure 2), the three leading individuals responsible for their training are radiologists (33%), licensed sonographers (29%), and medical doctors (20%). Therefore, there is a need for advocacy and recognition for radiologists, licensed sonographers, and medical doctors to not seek their interest. Instead, our collective responsibility is to safeguard the sonography profession jealously to protect lives. Training by unlicensed sonographers is 16%, but this can be impeded, and indeed all forms of training can be limited with enhancing enforcement and for regulators to declare the practice without a license persona non grata. Sonography training by midwives is two percent (2%), and this cohort of unlicensed sonographers are mainly females trained to primarily perform obstetrics sonography because of the high demand for sonographers at antenatal clinics. It is worth knowing that most so-called unlicensed obstetrics sonographers eventually venture into gynaecological and other body parts. It explains why 31% of our study respondents were females, a significant number (P=0.035). This can also be attributed to pregnant women’s enormous preference for females to perform obstetrics and gynaecological scans on them, especially at antenatal clinics. These findings are consistent with studies that showed the majority of females’ preference for female sonographers for obstetrics and gynaecological ultrasound.25,26 Therefore, our study finds these trends of sonography training an inferior form of knowledge transfer in ultrasound training.
The length of sonography training received by these unlicensed sonographers is illustrated in (Figure 3). The majority (41.9 %) of respondents received less than four months of training; quite a substantial number received between two to four weeks of training. Due to the high demand for medical sonographers, our study showed (Figure 3) that most of them (71 %) were engaged and started practicing almost immediately without any clinical supervision or internship, which is crucial in sonographic quality practice. Most respondents have been practicing for a year or more up to five years, as can be elicited from (Figure 4). About five percent have been practicing medical sonography for over 15 years without a license.
As can be inferred from (Table 2), the majority of respondents were SHS graduates, and most of them acquired their sonography training through on the job mode of sonography training (18.8%), ultrasound short course (18.3%), some 8.1% attended an unaccredited school, and 1.6% attended ultrasound workshop. It is unconscionable for these cohorts of unlicensed sonography practitioners with only SHS education (not a professional of any related health profession) to go through such a short period of training by all standards and be unleashed on the Ghanaian populace to diagnose diseases including life threatening conditions.
Our study also established the ownership structure of respondents’ workplaces, as shown in Figure 5. Most respondents (67.2%) worked in hospitals or clinics, and 29.6% worked in diagnostic centers. The ownership analysis revealed that 66.7% of the facilities were privately owned, 15.8% government-owned, 14.2% owned by the Christian Health Association of Ghana (CHAG), which are faith-based health facilities, and 3.3% of respondents had set up and operated their personal ultrasound scan center. The primary explanation for this trend, consistent with other studies27,28, is the high demand coupled with the limited number of licensed medical sonographers in Ghana. Therefore, both government and privately operated health facilities illegally patronize these unlicensed sonographers. The facility owners must sponsor these unlicensed sonographers to upgrade and be licensed. The Health Facility and Regulatory Authority (HeFRA) of Ghana is the body mandated by law to regulate institutions’ activities, providing any form of healthcare. Owners of private health facilities mainly utilize these unlicensed sonographers to exploit and pay them lower salaries than licensed sonographers. The lack of rigorous scrutiny of academic certificates of health professionals working at health facilities and the enforcement of regulations by the HeFRA makes unlicensed professionals’ practice without making serious efforts to upgrade. It is imperative to acknowledge these unlicensed sonography practitioners’ contributions in bridging the massive gap in the availability of licensed sonographers. However, urgent measures must be taken to mitigate the inadequate supply of professionally trained medical sonographers; otherwise, this challenge may persist for some time. Ghana, a developing country, is quite challenged with health facilities; therefore, the government strives to provide more health facilities. The expansion and provision of health facilities progress, coupled with insufficient availability of licensed medical sonographers, may worsen the already appalling status quo. This situation is similar to other developed countries, as according to the Bureau of Labor Statistics (BLS), the demand for diagnostic medical sonographers is expected to increase by 19% through to 2028.29,30
As can be inferred from (Table 3), the respondents’ perception of the practice and regulation of sonography practice in Ghana was optimistic. The majority (82.2%) of respondents believed the prerequisite for practicing medical sonography is to be licensed by the AHPC and for the profession to be rigorously regulated. The overwhelming majority (95.5%) of respondents wanted practicing unlicensed sonographers to be allowed to upgrade at accredited sonography schools leading up to their appropriate licensing with the AHPC.
The study found inadequate knowledge of the various forms of ultrasound scanning activities commonly performed by respondents irrespective of the kind of training received. A meticulous collation and scrutiny of some ultrasound reports brought by referred patients to our tertiary hospital characterize the menace and inexcusable harm some of these quack sonographers unleash on innocent patients. Out of 1,643 reports collated, 36.4% were competently written, and the pathology was accurately appreciated. Consequently, there is potential to harm patients through a lack of clinical insight, missed diagnosis, misdiagnosis, or over-diagnosis.31 Several preventable deaths, especially maternal deaths from our estimation, could have been averted had a certified medical sonographer performed the ultrasound scan. There were instances where ectopic gestations were misdiagnosed as ovarian cystic (mass) lesion after which the patient subsequently ruptured some few days later and died from haemorrhagic shock when brought to the hospital.
Ultrasonography is operator dependent; thus, the quality of examinations performed can vary based upon the operator. Numerous studies exist to corroborate the assertion that the key to patient safety is sonographer credentialization and facility accreditation.32–36 Clinical knowledge and appropriate ultrasound training are much-needed tools to scan and write good ultrasound report accurately. Waring et al.37 argue that ultrasound examinations performed by sonographers not adequately trained in ultrasound scanning and interpretation may be misleading or dangerous to patients, and we concur. We are mindful that this study’s findings and recommendations shall add impetus to the fight towards eradicating quack health professionals in general who runs a parallel health service in Ghana.
Limitations of the study
It would have been good to contrast the quality of reporting by unlicensed sonographers with those emanating from licensed professionals for unequivocal inferences on professionalism and quality.
CONCLUSIONS
Considerable evidence now proffered that supports the assertion that there is a high proliferation of unlicensed sonographers in Ghana. This situation is a significant public health issue, not exclusive for its immediate impact on patients and the attendant high healthcare delivery cost, but especially in emergencies, and long-term socio-economic implications. The unbridled practice of sonography by unlicensed practitioners is a recipe for higher misdiagnosis rates, clinical complications, and higher mortality in patients. With anticipation, regulators, policymakers, and stakeholders will now devise collaborative action to eliminate this unacceptable and unwarranted status quo and health menace. We recommend the following:
-
All practicing Diagnostic Medical Sonographers shall be required to register with the professional association and the Ghana Society of Radiographers (GSR) to safeguard the profession and strive to eliminate quacks in the country.
-
GSR’s umbrella association must support the licensed sonography practitioners, and the regulatory body AHPC shall be encouraged to organize training and educational programs on acceptable medical sonographic practices.
-
The Ghana fraternity of Medical Sonographers shall keep accurate records of all the members.
-
Diagnostic Medical Sonographers must be encouraged to use modern facilities and equipment to diagnose and manage patients.
-
Diagnostic Medical Sonographers shall be provided with badges and personalized stamps by the AHPC to certify their ultrasound reports and offer patients/clients options of differentiating between certified Medical Sonographer and quacks.
-
Appropriate standards of practice must be proffered and enforced at health facilities or diagnostic centers through HeFRA, and facilities must be encouraged to implement these standards.
-
All unlicensed practitioners must be encouraged to undertake further training in accredited sonography institutions to upgrade and enable them to register with the AHPC and be appropriately certified.
-
The AHPC and the government must drive to provide more accredited sonography training institutions to train more medical sonographers to ameliorate the massive disparity in these health professionals’ supply.
DECLARATIONS
Acknowledgements
The authors are incredibly grateful to the faculty members, staff, and management of the department of Imaging Technology and Sonography, University of Cape Coast and Klintaps University College, Accra for their support and collaboration in making this study possible.
Funding
None.
Data availability
Anonymized data relied on for this study may be released upon application to the Head, Department of Imaging Technology & Sonography, School of Allied health Sciences, University of Cape Coast, Ghana.
Authorship contributions
PNG, JS: Conceived and designed the study; designed the questionnaire, Analyzed, and interpreted the data; Wrote the manuscript. INO, CO: Literature search, analyzed and interpreted data, wrote the manuscript. EKME, KDT, ADP: Literature search, analyzed and interpreted the data, proofreading. DA, EAAG: Performed experiment; Collated data and analysis; analysis tools. All authors read and approved the final manuscript.
Competing interests
The authors completed the Unified Competing Interest form at www.icmje.org/coi_disclosure.pdf (available upon request from the corresponding author), and declare no conflicts of interest.
Correspondence to:
Philip Narteh Gorleku MD. Ph.D.
Department of Medical Imaging,
School of Medical Sciences
P.M.B. University of Cape Coast
Cape Coast, Ghana.
[email protected]