Malnutrition remains a significant problem worldwide, but the types of nutritional problems have changed significantly over the past two decades. While under-nutrition was and is still a major threat to health and well-being in middle-and low-income countries, obesity has equally become an additional problem in such countries with increasing prevalence. Micronutrient disorders are a global problem affecting about 2 billion people in both developing and developed countries. They are quiet epidemics of vitamin and mineral deficiencies that affect people of all genders and ages, as well as certain risk groups. In addition to causing definite disease conditions, they also worsen infectious and chronic diseases, significantly impacting morbidity, mortality, and quality of life.1 The nutrition transition in sub-Saharan African countries is complex because over-nutrition associated with overweight, obesity and other non-communicable diseases (NCDS) emerged before the problems of under-nutrition and micronutrient deficiencies have been solved, creating a double burden of nutrition-related ill-health.2–4
Obesity has more than doubled since 1980 globally. In 2008, more than 1.4 billion adults 20 years and above were overweight. Out of these, an estimated 205 million men and 297 million women, that is more than half a billion adults were obese.5 In 2008, the global prevalence of obesity was 10% and 14% among men and women respectively compared with 5% and 8% in 1980. In 2014, 39% of the world’s adult population were overweight while 13% were obese.6 According to the report by the World Health Organization (WHO),7 over 26.8% and 6.5% of adults are overweight and obese respectively in Nigeria. The prevalence of overweight was 26% and 37% in men and women respectively, while the prevalence of obesity was 3% and 8.1% in men and women respectively.7 Among individuals aged 30 years and above, the prevalence of overweight and obesity together increased by 23% in men and 18% in women, while that of obesity alone increased by 47% in men and 39% in women, between 2002 and 2010, in Nigeria.8 In South West Nigeria, 29% of the University undergraduate students were overweight, 6% were obese while 13% were underweight.2
The WHO considers that more than 2 billion people worldwide suffer from micronutrient deficiencies, primarily iodine, iron, vitamin A and zinc, with important health consequences.9 Though all ages and both sexes are affected, children less than 5 years of age, adolescents, women of childbearing age, particularly the pregnant and lactating, refugees and victims of famine are mostly at risk.10 Among university undergraduates in Lagos, Nigeria, only 31% eat up to three times daily, only 23% eat breakfast while only 2% consumed the recommended daily allowance of fruits and vegetables.11
Overweight and obesity are associated with many diseases. These include hypertension, diabetes mellitus, atherosclerosis, certain types of cancers, chronic kidney disease and increased overall cardiovascular risk.12–16 Others include asthma, osteoarthritis, and low back pain. Each 5 kg/m2 increase in BMI is associated with a 30% higher overall mortality risk and higher mortality from stroke, kidney disease, and diabetes mellitus in addition to reduced life expectancy by as much as ten years in those with BMI over 40 kg/m2.12 The public health implications of micronutrient disorders are also potentially huge. They do not only cause obvious clinical manifestations, but are also responsible for a wide range of non-specific physiological impairments, leading to reduced resistance to infections, metabolic disorders, and delayed or impaired physical and psychomotor development.17 In adults, they are also associated with the risk of several chronic diseases including cardiovascular diseases (CVD), osteoporosis and cancer.18
Obesity in young people in middle income countries, has serious implications in later life8 due to its consequences. The transition to higher education involves a significant life change (in environment and resources) for many students as they often start living away from their parental home for the first time, get more freedom and make new friends.19,20 This period is accompanied with un-favorable changes in health behaviors and has been implicated as a risk period for weight gain.21 The rates of obesity have increased rapidly among University students globally and locally and a recent study among undergraduates in Nsukka Campus Nigeria revealed a prevalence as high as 21%.22,23
Some studies have explored the prevalence of obesity among undergraduates8,11,24,25 but there is limited information on nutrient intake, the pattern of obesity using different methods of assessment and relationships between micronutrient disorders and obesity among university undergraduate students in Lagos. This study, therefore, determined the nutrient intake, the pattern of obesity using different methods of assessment and relationships between micronutrient disorders and obesity among university undergraduate students in Lagos State. The result will be useful for policymakers in detecting areas where intervention is needed in the prevention of obesity and micronutrient deficiency.
METHODS
A descriptive cross-sectional design was used to obtain data from full time undergraduate students in the three Universities in Lagos: University of Lagos (UNILAG), Lagos State University (LASU) and Caleb University.
A multistage sampling technique was employed to select the students from the universities. All the three Universities were included. Simple random sampling was used to select four faculties from the twelve in UNILAG and LASU and one college from Caleb. Using simple random sampling technique (balloting), at least one quarter of the number of departments was selected from each faculty making eleven (11) from UNILAG, five (5) from LASU and one from Caleb University.
Using sampling proportional to size, students were selected across faculties, departments and levels depending on the total population of students in each faculty, department and level. Systematic random sampling technique was employed in each class to select respondents. The number required from each class was used to divide the class list to determine the sampling interval. The total number of students interviewed was five hundred and six.
Data collection
Pre-tested, semi-structured interviewer administered questionnaire was used to obtain data on socio demographic and economic characteristics. Mean nutrient intakes were estimated from 24-hour dietary recalls which were conducted on two days of the week (one week day and one week end day). General and abdominal obesity were assessed using anthropometric measurements while percentage body fat was determined using Bio-electrical Impedance Analysis, following standard procedures.
Data analysis
IBM SPSS Statistics (version 20) was used for data analysis. Associations between variables were tested using Chi-square and Fischer’s exact tests. Twenty-four (24) hour-diet recall was analyzed using Total Diet Assessment soft-ware. Anthropometric indices were compared with WHO standards and classified.
RESULTS
Socio-demographic status
Their ages ranged from 15 to 41 years but the modal age group was 19-24 years while the mean age of the respondents was 20.3 + 3.45 years. More than half of the respondents (54.7%) were females and majorities were Christians’ (82.9%). Majority (47.6%) of the students had no consistent source of income or received less than N10,000 (USD 31.7) pocket money.
Mean energy and nutrient intake of respondents
Mean nutrient intake of respondents were compared with FAO/WHO 2001 standards for daily recommended intakes of nutrients according to sex and age group. Most micro-nutrients were deficient except thiamine, and zinc. Micronutrients such as iron, calcium, potassium, folate, vitamin C, B2, B6 and B12 were inadequate while intake of sodium was higher than the recommended values for some age groups. There was no statistically significant difference between male and female mean nutrient intake for all the nutrients. (Tables 1 and 2)
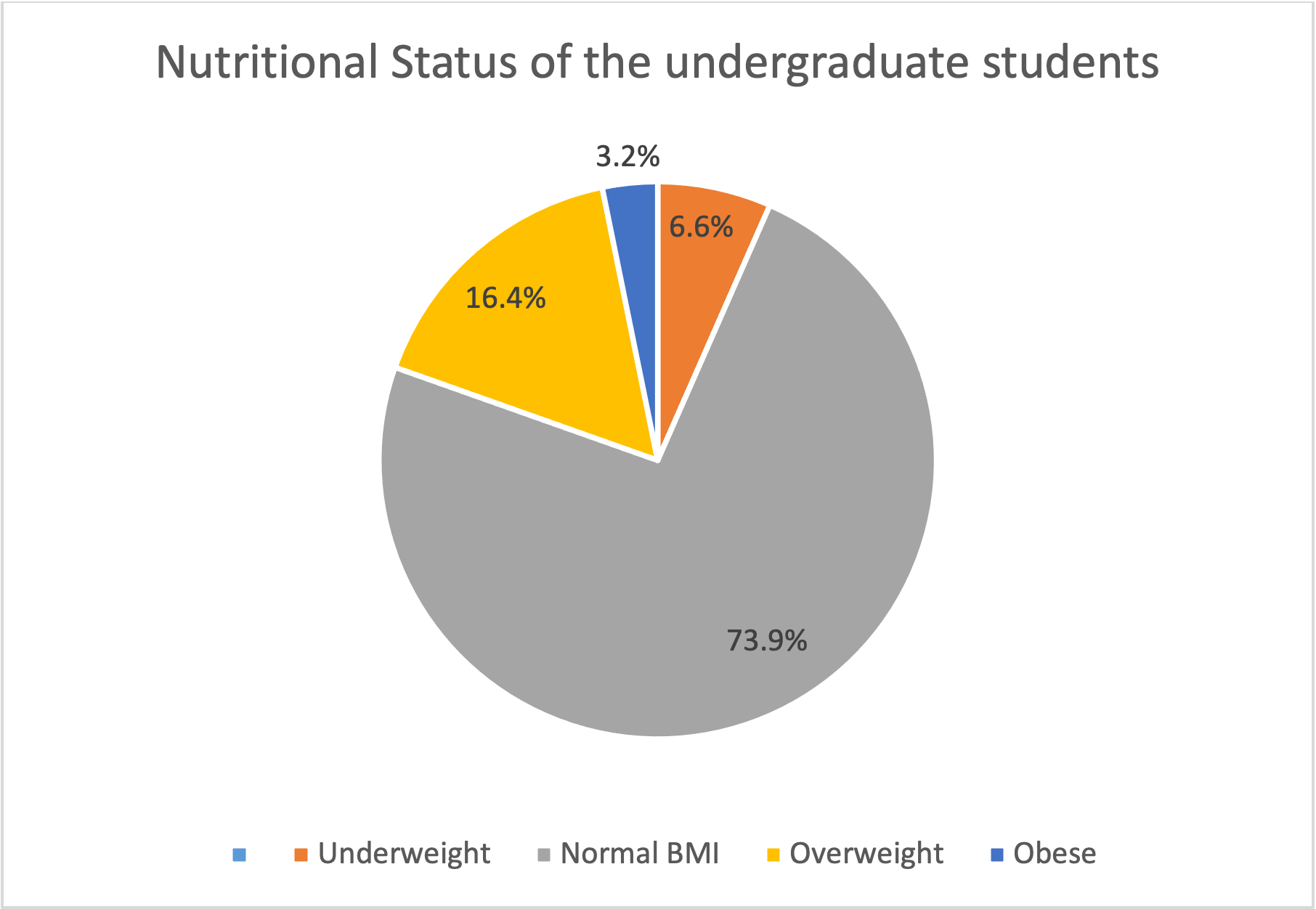
Overall BMI classification of all the respondents
According to Body Mass Index (BMI) classification, most of the students (73.9%) were in the normal range of BMI. Only few of them were underweight (6.6 %), overweight (16.4%) and obese (3.2%) (Figure 1).
_classification_of_all_the_respondents.png)
Pattern of obesity using different assessment methods by gender
Body mass index showed that 3% of males and 3.3% of females were obese. Based on waist circumference (WC), 1.3% of males and 8.4% of females were obese, whereas 12.3% of males and 26.5% of females were obese using Waist to Hip ratio (WHR). Prevalence of abdominal (central) obesity was significantly higher among females than males (P=0.000 for both WC and WHR). Obesity assessed using the percentage body fat had the highest yield of 54.4% in males and 37.1% in females. The difference between males and females were not statistically significant (P=0.69) (Table 3).
Prevalence of micronutrient deficient diet among undergraduates in Lagos
Almost all the under-graduates had vitamin B12 (86.8% M, 86.2% F), pyridoxine (92.5% M, 90.2% F) calcium (98.7% M, 99.6% F) and potassium (100% M, 99.6% F) deficient diet while almost half of them consumed excess sodium. Most of the females (58.9%) had iron deficient diet while more than half (56.1%) of the males consumed zinc deficient diet (Table 4).
Predictors of obesity
Males were 0.597 times more likely to develop obesity than females and students who had inconsistent amount of income were 2.23 times more likely to develop obesity than those who had no source of income. Moreover, for every one unit increase in folate, the likelihood of developing obesity was 1.0.
DISCUSSION
The average age was 20.31±3.454 with 54.7% being females and 45.3% being males. Most of the students had educated mothers and enlightened parents who lived in detached houses/duplex (23%) or bungalows (28%) or self-contained apartments within story buildings (41.6%) but many (37.6%) of the students received less than N10, 000 (USD 30) monthly pocket money or had no consistent source of income.
Most of the nutrients and energy were deficient except carbohydrates. This study contradicts the study by Hirshberg where intakes of total energy surpassed guidelines26 but agrees with another study in Ghana where female respondents met 97 percent of energy requirement while the males met only 66 percent.27 The energy might have been deficient because many undergraduate students in Nigeria eat only two times daily and buy most of their meals from fast food restaurants.11 Since many undergraduates perceive inadequate funds as a reason for not eating healthy, they might have purchased small portion sizes of meals that were affordable rather than purchasing enough portion size to meet their needs.11 The low energy and high carbohydrate intake infer that the students’ diet consisted of majorly simple carbohydrates with little energy from other sources such as protein and fat rich foods. Energy is very critical in metabolism because the transport, synthesis, and breakdown of nutrients and molecules in a cell require the use of energy.28 Adequate energy intake is also important to reserve protein for more important functions like hormone and enzyme production and building of tissues rather than energy generation. Protein intake was better than energy especially among the females probably because many of them ate meat which contains a high amount of qualitative protein daily; however, some of it could have been converted to energy rather than fulfilling the special functions of protein.
The fiber intake was not adequate. This agrees with the result of another study by Irazusta which shows only 43% of females and 51% of males met the recommendations for fiber intake.29 Adequate fiber is very important in bowel movement, weight control and prevention of NCDs generally.30
Iron intake was not adequate for all the age groups especially among females. Majority (92%) of the females had iron deficiency. They met only 40% of their requirement while the males met 78% of their Recommended Dietary Allowance (RDA). Females require more iron than males in order to replace menstrual iron losses which make them vulnerable to anemia and other iron deficiency disorders. Iron deficiency anaemia should be avoided among females of reproductive age because children born to such people are likely to suffer poor growth and cognition. This result is similar to the one obtained in the Ghana study above where intake of iron was low among the females.31
Zinc intake was adequate among females but not adequate for males who require more zinc. Almost half (49%) of the males had zinc deficiency. Its adequacy is critical to the males’ reproductive ability. Zinc enables the male body to produce testosterone apart from other general functions such as production of enzymes and promoting immune function.32 Calcium intake was low compared to RDA (less than 50%). This is probably because the undergraduate population did not consume enough milk or milk products daily despite its importance as a major source of dietary calcium.33 The proportion of students who took milk and its products in other studies in similar population was low.8,34
Sodium intake was in excess for both males and females while potassium deficiency was almost universal. Almost all the under-graduates (99%) had potassium deficiency while less than half had hypernatremia This is probably a result of frequent consumption of processed foods and fast food restaurants while consuming inadequate fruits and vegetables. Diets based on processed foods are high in sodium and low in potassium.25 This finding agrees with the study by Burke et al among undergraduates in University of New Hampshire in United States which discovered that more than 90% of college students exceeded sodium recommendations.35 High level of sodium and low level of potassium intake are risk factors for hypertension in many people and it is recommended that sodium intake should be limited while potassium should be increased.36 Research has shown that the problem with hypertension is not just high level of sodium but the balance between sodium and potassium. Higher potassium intake has been found to result in blood pressure lowering in the overall population with more pronounced effects in patients with hypertension or consuming a high sodium diet.31 Unfortunately, less than one third of Nigerians consume adequate amount of fruits and vegetables which are rich in Potassium.
This result is similar to another one in Ghana, where about two-thirds had normal BMIs and a third were either overweight, obese or underweight.31 The prevalence of general overweight & obesity in this study was lower than obtained among undergraduates in South Western Nigeria generally (29%, 6%) and in a Central University in the West Bank (25%, 7.2%).8,37 The prevalence of abdominal obesity was significantly higher among females compared to males using waist circumference and waist to hip ratio (p=0.000). The percentage body fat assessed using bio-electrical impedance analysis yielded the highest rate of obesity which was higher among males though the difference was not statistically significant.
Limitations
Ideally, it would have been better to obtain and use blood samples to demonstrate objectively the measure of deficiency or excess of micronutrients; however, 24-hour diet recall was used as a proximate. There could have been a challenge with accuracy of recall and extrapolating micronutrient deficiency from two days nutrient intake could have yielded some degree of inaccuracy.
CONCLUSIONS
Mean nutrient intake was lower than RDA for most micronutrients except thiamine and sodium ,which were too high. Micronutrient-related malnutrition and central obesity were higher than reported in previous studies. Male gender, inconsistent income and increased amount of folate were significant predictors of obesity. Nutrition and lifestyle education programs targeting behavioral change should be instituted in universities through the school curriculum. Whole foods such as legumes, milk, fruits and vegetables which can also supply iron, calcium, potassium, folate and other micronutrients and control weight gain are recommended for the undergraduates.
Acknowledgements
The authors wish to acknowledge the Deans of Students affairs of the three universities for granting permission to collect data.
Ethics approval and consent to participate
The study was conducted according to the guidelines laid down in the Declaration of Helsinki. Ethical approval was obtained from the Health Research and Ethics Committee of the Lagos University Teaching Hospital (Ref No: ADM/DCST/HREC/APP/179 and Lagos State University Teaching Hospital (Ref No: LREC/10/06/630). Informed written consent was obtained from all students as well as parental consent from those who were younger than eighteen (18) years of age before conducting the study, and confidentiality was maintained.
Availability of data and material
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Funding
None
Authorship contributions:
FO, SA, EA, OO conceptualized and designed the study. F.O acquired and interpreted the data. FO, SA, EA and KN drafted the manuscript and critically revised it for important intellectual content. KN was a major contributor in writing the manuscript. All authors read and approved the final manuscript.
Competing interests
The authors completed the Unified Competing Interest form at www.icmje.org/coi_disclosure.pdf (available upon request from the corresponding author), and declare no conflicts of interest.
Correspondence to:
Dr. Foluke A. Olatona
Department of Community Health and Primary Care
College of Medicine, University of Lagos, Nigeria