
As in most countries south of the Sahara, persistent infections with hepatitis viruses represent in Gabon a significant burden of disease. 1 Recent data indicate that 7.3% of first-time blood donors are carriers of the hepatitis B virus (HBV) surface antigen (HBsAg).2 Molecular analyses have also demonstrated that a significant subset (8-16%) of HBsAg(-) patients present circulating HBV DNA sequences in their blood suggestive of an occult B infection (OBI).3 In addition, it appeared recently that a substantial proportion of HBsAg carriers (25%) are co-infected with the hepatitis delta virus (HDV).3,4 The prevalence of infection with the hepatitis C virus is geographically heterogeneous with a report indicating a seroprevalence of anti-HCV ranging from 2.0-21.0% depending on the location of sampling campaigns.5
Other risk factors of chronic liver diseases are also significantly prevalent in Gabon. It is the case of alcohol consumption considered as very high in the country (10.9L of pure ethanol per capita), ranking in the second position on the continent, on the par with South Africa (11.0L).6 Noticeably, abuse of alcoholic beverages is considered to have increased dramatically in the country during the last decades.7,8 Moreover, it seems risky to properly estimate the local consumption of the numerous versions of very popular unrecorded alcoholic beverages produced from cane, maize, cassava, or palm.7 In Europe, investigators have already drawn the attention of the medical communities about the danger of such beverages with a poorly defined chemical composition.9 Unfortunately, very few qualitative studies have been hitherto conducted in Sub Saharan Africa (SSA).10 Furthermore, the role played by aflatoxin B1, another major toxic risk factor of PLC, is totally undocumented in the country.11,12
Overall, and even without further detailed consideration about more recently appeared risk factors of liver tumors such as type 2 diabetes, metabolic syndrome and obesity, the potential consequences for liver health of the current Gabonese epidemiological situation do not look better than in any surrounding countries13 and could even be considered as worse when alcohol consumption is examined specifically.
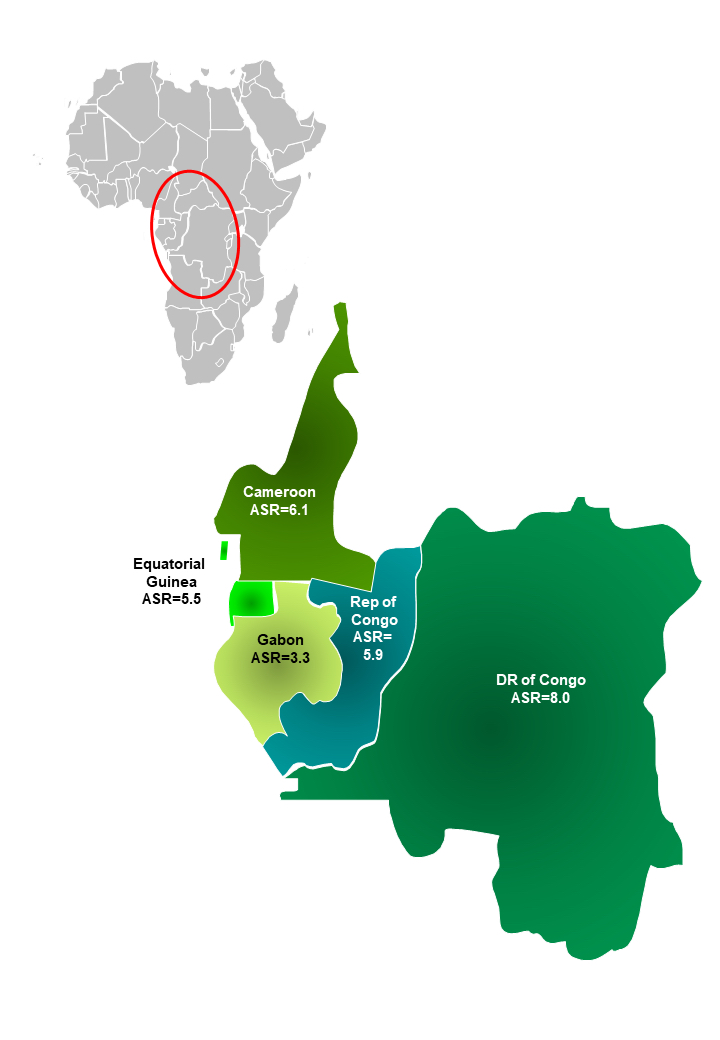
Intriguingly, and in contrast with all neighboring countries, the epidemiology of primary liver cancer (PLC) in Gabon is currently not considered as a worrying Public Health problem. Looking at the most recent Globocan data, the crude incidence of PLC is 2.7/10E+05 habitants (ASR=3.3) when both sexes are included. It ranks in 44th position out of 52 countries in Africa. The situation is rather similar when sexes are considered separately (ASR=3.9 in men, 45th, and ASR=2.6 in women, 42nd). These figures position the populations of Gabon at the level of Danish women (ASR=2.6) and slightly above that of Latvian men (ASR=3.8) for PLC incidence.14 Furthermore, when we compare the proportion of recorded Gabonese PLC cases published in the last version of Globocan with those observed in neighboring countries (Republic of Congo, Equatorial Guinea, Cameroun or the Democratic Republic of Congo that does not share any border but is distant from only 150km at its closest), we found that PLC incidence is significantly lower in Gabon than in any of its neighbors (see Table1 and Figure 1). Few HCC cases have been reported in the literature from Gabon albeit always in papers focusing on another medical issue.15,16 Such fragmented elements of a larger landscape suggest nevertheless that the disease is present in the country as it is in its Northern or Southern neighbors where it is generally more strongly acknowledged.17–20

Given the landscape of PLC, risk factors described ut supra, there is clearly a discordance between the pressure applied by well-recognized causal agents for PLC and the apparent consequence of their presence in Gabon in terms of tumor numbers. However, a recent global survey of potentially missed incident cases suggested that Gabon is the second country in the world (after Cameroun) for PLC underestimation.21 Finding an explanation for this discordance is not straightforward. A parsimonious explanation would be that there is a massive under-reporting of PLC cases in Gabon.
Partly due to the small population size (2.2 million, world rank=143/203), the country has very limited health infrastructures. In the oncology field, Gabon has a cancer institute in the capital (Institut de Cancérologie de Libreville, ICL) where all patients with tumor diseases should be referred to in theory. The capacity of ICL is rather small as it can accommodate only 600 patients per year while the incident cancer burden in Gabon is estimated to 1700 cases by Globocan in 2018.14 This underpowered institution, incapable to manage each patient affected by intrinsically severe diseases, generated in the population, feelings of frustration and, defiance whose expression is regularly conveyed by the national press.22 More globally, the whole health system is considered as dysfunctional, inefficient, inequitable, and dilapidated in Gabon. As a consequence, the population nurtures a notoriously difficult relationship with the main University Hospital of the country (CHUL). This situation is all the more paradoxical that Gabon is considered as a rich country in Africa (4th position, 18100 USD/hab/year) with substantial resources earmarked for public health.23,24
The National Cancer Registry has been established recently (2017) and the referral of new cases to this structure is plausibly still not well anchored in the habits of the local medical practitioners.25 It seems clear, however, that a significant improvement of the visibility of this structure is expected in the future. In any case, it would be unfair to blame so early a novel structure installed in Gabon as several recent reports came to recall that PLC is notoriously under-reported in many countries including high-income ones.21,26,27
More speculative hypotheses can be made to explain the low rate of PLC in Gabon. Habitants could be either protected by their genetics or by healthier lifestyle habits. Both explanations are similarly eccentric. Local populations are a priori similar to those of neighboring countries (ie Bantus and Pygmies).28 Furthermore, as already mentioned, concerning a putative healthier way of life of Gabonese, the issues of obesity or alcohol consumption in the country indicate that populations are not more cautious that neighbors and it is even rather the opposite concerning alcohol consumption.29,30
Finally, we propose that the propensity of the Gabonese population to privilege the use of traditional medicine might explain putatively missing PLC cases in Gabon. The magnitude of the use of traditional medicine by the general population in SSA is currently a matter of fierce debate. It appears, nevertheless, that without reaching the poorly documented percentage of users (80-90%) commonly cited in the literature, it is still very high in most African countries.31,32 Until recently, criticisms against traditional healers with regard to their handling of neoplastic diseases were rather mild or even toned down. For some investigators, often living in the Southern part of SSA, traditional healers are considered to play a positive role in the education of populations and the prevention against cancer.33 Elsewhere in Africa, and notably, in West Africa, the appraisal of the role of the healers in cancer care is far less favorable and it is often considered that they contribute to the late diagnosis and care process implementation or to the absconsion of patients.34–37 Recent medical literature from Africa drew the attention of the medical community on this problem and it is possible that Africa will enter soon in a period of medical history already observed in Europe where modern medical power installation conducted to the elimination of “illegal” healers.38 Given the importance of liver diseases in SSA (often >10% of the general population is concerned in most countries), the common practice of traditional healers is, of course, often dedicated to patients affected with chronic hepatitis ie at risk to develop terminal complications such as liver cirrhosis or PLC. The potential consequences of the frequentation of healers rather than the medical doctors are well known and manifold in the case of liver diseases. First, some herbal remedies used in SSA are hepatotoxic and lead occasionally to veno-occlusive diseases or severe fibrosis due to their high content in pyrrolizidine alkaloids (eg retrorsine) sometimes even considered as potential liver carcinogens.39 In fact, some plant-based traditional medicine often used to treat all types of common pains and diseases have shown their deleterious activity on liver cells.40,41 Second, traditional healers are sometimes conducted to practice subcutaneous cuts on which they rub herbal remedies. Incidentally, these cuts are mostly done with razor blades or other instruments often reused and, in any case, never sterilized according to the principles of modern antisepsis. When applying such practices in a country where a large pool of individuals is infected with hepatitis viruses, it contributes probably to the spread of the diseases they are supposed to fight.42 Third, by delaying the access to adequate treatment, consultation of traditional healers obviously lowered the patient’s chance of survival.35,37 Actually, herbal remedies targeting liver diseases are widely sold in the markets of Gabonese cities. It is, for example the case of the barks from Nauclea diderrichii (Brimstone tree, a vulnerable species, Rubiaceae) and from Annickia affinis (African yellow wood, Annonaceae) (Figure 2). The large place occupied by the traditional medicine in Gabon has historical explanations. First, traditional medicine was the only available health system before colonization, it is as such well accepted by the populations. Second, a significant number of herbal medications employed in Africa were shown to be efficient to treat certain pathologies.43 Third, currently, and particularly in Gabon, traditional medications are often cheaper and more easily available than modern drugs.44 The two latter characteristics led governments including that of Gabon as well as international organizations to promote to some extent the use of traditional medicine. As an outcome, traditional healthcare facilities occupy a very large space in Gabon and in Libreville, the national capital in particular.45
__nauclea_diderrichii__or_(b)__annickia_affinis__commonly_employed_to_treat_li.jpg)
Along with the use of traditional phytotherapy common to the whole sub-Saharan Africa, another important layer of tradition is playing a crucial role in Gabon. According to René Bureau, a french ethnologist specialist of this subregion of the continent, “Gabon is to Africa what Tibet is to Asia, the spiritual center of religious initiations.”46 Indeed, in Gabon, prevails the Bwiti, a lively and prestigious tradition of initiation by cult associations, that exerts its attraction both on laypeople and on persons with higher education. The fact that the first president of independent Gabon (1962), Léon M’ba, was initiated to Bwiti in 1933 is a good illustration of the importance of this tradition in Gabon.47 Bwiti is the religion of Eboga, based on the consumption of a psychoactive drug, ibogaïne, an indolic alkaloid present in the root bark of Tabernanthe iboga, a shrub from the rainforest.48,49 A therapeutic branch of Bwiti, Bwiti Misoko, produces the traditional healers or Ngangas.50,51 Remarkably, recent observations indicate that modern and traditional medicines are in competition in Gabon. Somewhat counterintuitively, it appears that in Gabon for a given disease, the most severe presentations are generally attributed to supernatural aetiologies (witchcraft, spirits), and brought to Ngangas rather than to modern medical facilities.52 In the context of medical syncretism, the failure of initial medical treatment is another motivation to shift for a Nganga implying thereby that the traditional healer is considered as the last resort for patients in Gabon. It seems plausible that, from the onset, for some patients with severe disease, modern medical treatment is never considered. Overall, these observations, originally made on cases of malaria, fit rather well with the refractory character of PLC towards therapeutics. Furthermore, this behavioral typology was obtained from the observation of young mothers who benefited from recent medical education campaigns. It is thus highly improbable that the propensity to rely preferentially on modern medicine will apply to some extent to middle-aged patients affected with severe liver disease. It is, on the contrary, highly probable that the Bwiti or any of its less advertised affiliate branches attract a significant part of Gabonese patients with PLC preventing any form of proper medical diagnosis. A survey of HIV-infected patients in Gabon led to similar conclusions.53
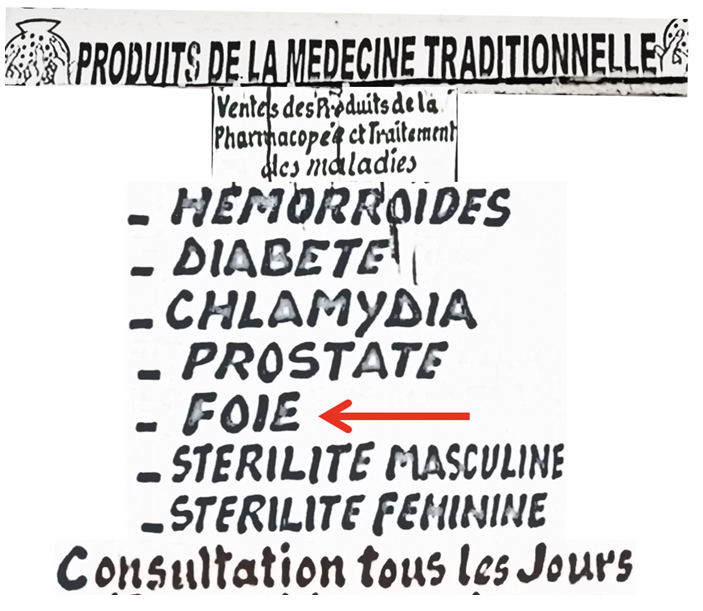
We hypothesize that in some countries of sub-Saharan Africa, and particularly in the case of PLC, notoriously associated with short survival, traditional medicine diverts accurate reporting of incident cases and artificially reduces PLC incidence. This situation has obviously damaging effects on health policy planning, on prevention measures, and on their subsequent evaluation. In the long term, it probably prevents or at least slows down significant improvements of public health in the nations concerned by an important usage of traditional medicine. In this regard, in Gabon, billboards and flyers proclaiming the merits and success of traditional healers, conspicuous in Libreville the national capital, (Figure 3) are probably participating in the perpetuation of the dominance of traditional practices in the treatment of severe liver disease.

In such circumstances, it is not easy to propose a “win-win” agreement between traditional and modern medical practitioners. Of course, public health stakeholders should instead implement long-term policies combating infections with hepatitis viruses, and uncontrolled use of alcohol. Such policies begin with the universal immunization of newborns and the subsequent evaluation of vaccination campaigns by serological surveys.54 It continues by the routine practice of hepatitis virus screening with sensitive methods including molecular ones. Infection by HDV is rarely tested in routine in Gabon, its implementation could, thus, represent rapid progress. Better and cheaper access to antiviral drugs is also mandatory in a country that occupies the second rank in continental Africa for Gross Domestic Product per capita. The systematic equipment of hospitals with transient elastography measurement devices (eg Fibroscan) to assess liver stiffness will result in improved surveillance either of patients with chronic liver infections or alcohol abusers at risk to progress toward cirrhosis or PLC.55 Besides, widespread distribution of cheap and portable ultrasound devices (http://www.echopen.org/) by specialists and non-specialists of liver diseases might help in the early diagnosis of liver nodules even in remote regions of the country.56,57 Beside diagnostic improvements, the installation of hospital facilities enabling liver tumor ablation by local therapies (radiofrequency, thermal, microwave, etc…) could be another major sustainable achievement for modern medical practice and a source of new hope and relief for the patients in Gabon.58
Finally, we can imagine in somewhat utopic speculation that the establishment of traditional medical structures manned by Ngangas-healers close or connected to hospitals will both respect Gabonese traditional culture and promote a medical syncretism that will, on the long term, facilitate the transition from tradition to modernity. Purely material aspects of traditional medicine are to some extent accessible to partial modernization. This will necessitate the establishment of general guidelines defining the frame of practice. It might imply the creation of a National Order of Healers, the professionalization by training, the standardization and quality insurance of substances (Pharmacopeia) and practices resulting from National Order guidances, information exchange and database construction, national networking and collaboration, technology transfer, commercialization of best products, and finally integration of traditional medicine as a branch of the national health system. Such partnerships, once implemented by Gabonese public health stakeholders might improve the position of modern scientific medicine for the larger benefit of local populations. The mutual defiance nurtured by traditional and modern medical systems associated with spiritual dimensions of the traditional medicine inherently reluctant to modernity might, however, delayed such beneficial evolution.45
Conclusions
According to the most recent estimates, and despite a high prevalence of all major risk factors of PLC in the population, Gabon is characterized by a significantly lower incidence of this deadly disease than in any neighboring country. We consider that the very popular local religious tradition of Bwiti, based on Tabernanthe iboga consumption supposedly enabling intercession with supernatural forces in case of severe disease, diverts a substantial proportion of patients from the modern medical systems and is responsible for the underreporting of PLC in the country. Thus, we recommend a closer association of traditional medicine with mainstream healthcare and the implementation of a national policy for traditional medical practice. To be perfectly fair, though, it appears that improvements of the system should apply, as well, and with a similar magnitude to the functioning of modern biomedicine in Gabon.
Funding: PMB was supported by a fellowship the Union for International Cancer Control (UICC) who granted PMB with an African Cancer fellowship for a training in Institut Pasteur.
Authorship contributions: PP conceived and put forward the hypothesis. PP and PMB wrote the draft of manuscript. BM, PEIB, AM, AMO, and JBMK critically read the manuscript. PP and PMB prepared figures.
Competing interests: The authors completed the Unified Competing Interest form at www.icmje.org/coi_disclosure.pdf (available upon request from the corresponding author), and declare no conflicts of interest.
Correspondence to:
Dr. Pamela Moussavou-Boundzanga
Laboratoire de Biologie Moléculaire et Cellulaire (LABMC)
Université des Sciences et Techniques de Masuku
BP 943, Franceville, Gabon
[email protected],
(+241) 066556468/077290083
Pascal Pineau Unité « Organisation nucléaire et oncogenèse », INSERM U993, Institut Pasteur, France, [email protected]