The disparity in maternal health outcomes between high- and low-income countries remains unacceptably high. Almost all of the estimated 295,000 maternal deaths in 2017 occurred in the developing world, with two thirds of this burden resting in sub-Saharan Africa.1 Most recent estimates place Ethiopia as the fourth largest contributor to global maternal deaths, behind India, Nigeria and the Democratic Republic of Congo.1 Reflecting the global situation, postpartum haemorrhage (PPH) is the largest cause of maternal deaths in Ethiopia, contributing to almost one third of the deaths in the country.2,3 Thus, strategies to better manage PPH will be critical in order to reduce maternal mortality in Ethiopia. The current gold standard therapy for the prevention of PPH recommended by the World Health Organisation (WHO) is active management of the third stage of labour (AMTSL), involving uterine massage, controlled cord traction and administration of a uterotonic.4 Administration of a uterotonic has be shown to be the most effective component of AMTSL and an oxytocin injection is the first line drug, reducing the risk of PPH by approximately 40-50%.5,6 However, access to a quality oxytocin product in low-resource settings is challenged by the requirement for a skilled birth attendant to administer the injection, and a consistent cold chain to maintain product quality.7,8 In Ethiopia, these elements are not always available in settings where women give birth. According to the most recent demographic and health survey, 72% of women give birth without a skilled provider.9 Further, cold supply and storage of oxytocin is challenging in many areas of Ethiopia due to a lack of available and reliable refrigeration facilities.2,10,11
To overcome the current barriers to the accessibility of a quality oxytocin product in low-resource settings, novel heat-stable formulations of the drug are currently under development, including a sublingual tablet12 and oxytocin inhalers.13–15 These products are designed to simplify the administration of oxytocin and remove the need for refrigerated storage or additional consumables for administration.
While innovations such as these may possess technical attributes and meet clinical efficacy criteria required to prevent PPH in low-resource settings, delivering impact is dependent on achieving and sustaining end user access. The concept of access in health care has been proposed to be dependent on five major characteristics: affordability, availability, accessibility, accommodation and acceptability of a service or product.16 Many studies have shown that end user acceptability is key for effective scale up of health innovations in LMIC,17–20 and that an assessment of acceptability should be conducted early in development, such that products can be designed and adapted as necessary to align with user needs and values.21
In line with these principles, this study aimed to assess the potential acceptability of an inhaled oxytocin product to key stakeholders in Ethiopia, namely community members, healthcare providers and policy-makers. This research highlights ways in which the needs of the end-users can be integrated into the design of this type of product and its implementation strategy, with an ultimate aim of improving acceptability.
Methods
Methods are reported according to the consolidated criteria for reporting qualitative research (COREQ) framework.22 This study was conducted as part of a wider research program aiming to understand the acceptability and feasibility of an inhaled oxytocin product in Myanmar, Ethiopia and India. Research methods have been previously described,23 however, an overview is provided here.
Research team and reflexivity
The data collection team was composed of researchers with experience in qualitative research methods and a thorough understanding of the local context. A four-day training workshop was undertaken by all researchers, covering the details of a heat-stable inhaled oxytocin product, the study aims and a refresher training on qualitative research principles and the ethical conduct of research involving human subjects.
Study design
A qualitative thematic content framework was applied to explore acceptability of an inhaled oxytocin product from the following three angles:
-
Contextual acceptability explored knowledge, attitudes and practices towards the medical condition (PPH) and comparable medicines, as these elements will form the context in which an inhaled oxytocin product will be positioned and thus will underlie acceptability.
-
Product acceptability was assessed directly by exploring perceptions toward an inhaled oxytocin product itself.
-
Usage setting acceptability sought to understand the most appropriate setting for product use.
Data were collected through focus group discussions (FGDs) and in-depth interviews (IDIs).
Participant sampling and recruitment
Participants of this study were community members, healthcare providers and key informants (Table 1). Community members were selected on the basis of their ability to share insights reflective of the target patient population and thus included mothers and their families (husbands, parents and in-laws). Individuals involved in community-based health education and promotion were also selected, including traditional birth attendants, health development army members and religious leaders. The health development army is a network of volunteers who serve as a link between the health system and their community by extending health education and promotion messages. Participants were identified through a key figure within the community, such as an elder or health extension worker, and invited (in person) to participate on the day of data collection. Healthcare providers were purposively sampled based on their ability to share insights reflective of the potential end-users of an inhaled oxytocin product, including midwives, nurses, doctors and pharmacists. These participants were invited to participate in person by a member of the research team on the day of data collection. Key informants were selected on the basis of their ability to share insights relating to the acceptability of this type of product to key policy-makers, and included government officials, members of professional associations or non-government organisations, and health facility administrators. A total of 244 individuals were engaged in relation to the findings reported here, comprising 143 community members, 73 health care providers and 28 key informants.
Setting
Data was collected from three regions of Ethiopia including a major region (Oromia) and two emerging regions (Gambella and Afar). Research was also conducted in Addis Ababa, where data collection focussed on key informant interviews with ministry of health officials, senior obstetricians and members of professional organisations. FGDs and IDIs with community members were conducted in a location which was convenient for participants in addition to offering required comfort and privacy. This included a community hall, or primary school. Interviews with healthcare providers and key informants were typically conducted at or near the workplace for the sake of convenience for the participant. In each case, a private space was located for the interview to achieve privacy and isolation from distractions. For all FGDs and IDIs only participants who were intentionally recruited and who had given their informed consent were present during data collection.
Data collection
Written informed consent was obtained from all participants on the day of their involvement in the study, before commencing each FGD or interview. Semi-structured guides were used to moderate discussions and interviews. Guides were pre-tested during a one-day pilot exercise and adapted as necessary before data collection commenced.
In order to explore attitudes and perceptions towards an inhaled product, a typical breath-activated inhalation device was shown to participants as an example of an inhaler that would be suitable for use with an inhaled oxytocin product. This inhaler was used in early phase clinical studies for an inhaled oxytocin product currently under development and is a useful illustrative example due to its low cost, passive inhalation mechanism and simplicity of use.
Where consent was provided by the participant(s), discussions and interviews were audio recorded using two digital recorders (one acted as a back-up). Field notes were taken for all FGDs and IDIs to record any non-verbal observations and serve as a back-up in case audio recordings failed or were inaudible. Audio recordings were transcribed verbatim in the source language, supplemented with field notes and translated into English. A selection of transcripts were then checked for accuracy against the audio recording by third party translation specialists.
Data analysis
A thematic content framework was applied to data analysis. Transcripts were coded using NVIVO software version 11(QSR International, Melbourne, Australia) by a team of three researchers. In order to encompass a range of relevant perspectives, the analysis team was composed of a member of the data collection team, a researcher from an inhaled oxytocin product development team and an independent experienced qualitative researcher. Each transcript was read by an analyst independently and open codes applied to units of meaning within words, phrases or paragraphs of text. Analysts met regularly to compare codes and agree upon a common coding framework, which was then applied to subsequent transcripts until all had been coded.
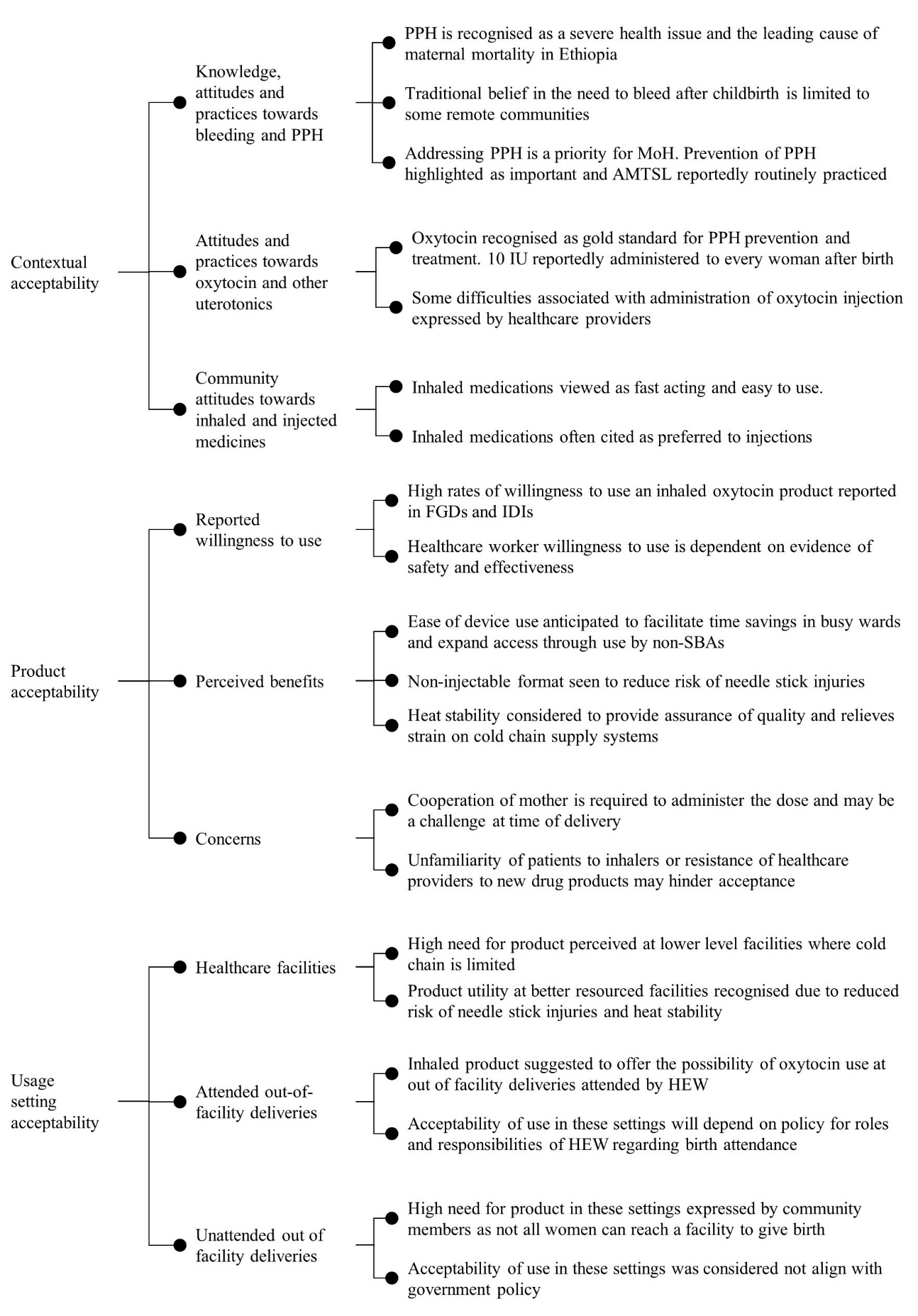
Through a group consensus approach, open codes describing similar ideas were grouped into themes. These themes were further grouped under thematic categories representing the three fields of acceptability as shown in Table 2 and Figure 1. This thematic framework was discussed and agreed upon by all researchers at a final analysis workshop at the conclusion of the study. Key findings were disseminated back to study participants and stakeholders in each study site between July – August 2017.
Ethical approvals
Ethical approval to conduct the study was provided by the Alfred Hospital Ethics Committee in Australia (Project 153/15), the Scientific and Ethical Review Committee of Ethiopian Public Health Institute (EPHI 6.13/269) and was ratified by the Monash University Human Research Ethics Committee (CF15/1701 – 2015000854).
Results
See Figure 1 for a schematic overview of the major findings in each theme. Findings are described in more detail below with illustrative quotes from FDGs or IDIs.

Contextual acceptability
Knowledge, attitudes and practices towards bleeding and PPH
Many healthcare providers expressed their concerns for PPH and recognised the complication to be one of the leading contributors to maternal deaths not only globally, but also in Ethiopia. Some providers explained how quickly bleeding can result in death of the mother and therefore stressed the importance of prophylaxis to ensure treatment is not the only measure relied upon to save the life. Healthcare providers from all regions reported that AMTSL is practiced for the prevention of PPH at every childbirth taking place in a health facility.
Knowledge of and concern for bleeding after birth was also common amongst community members, and was commonly identified as a possible complications that can occur during childbirth. Several community members remarked on the serious nature of PPH, with many suggesting that it can put the labouring woman at risk of death.
“The excessive bleeding may be life threatening to labouring mothers…Blood is what a human soul is in. The human soul is in the blood according to the bible. If there is no blood there is no life.” – Priest of an Orthodox Christian Church, urban area, Oromia.
There were some community members in Afar who expressed a belief that postpartum blood loss is beneficial or necessary. However, most of these participants also expressed their opinion that too much blood loss is dangerous and should be prevented.
Several key informants from within the Ministry of Health and the health service sector explained the focus of government efforts to overcome the burden of PPH in Ethiopia. Promotion of AMTSL was described as a major component of the government’s strategy to reduce PPH. Additionally, efforts are directed towards securing consistent availability of key health commodities, including oxytocin.
“So haemorrhage is a major problem. That’s why we want to make sure all human resource we have, that is, with maternity care have the proper skills associated with it. And we also make sure that we have all the required commodities and supplies for prevention and management of haemorrhage.” – Policy-maker, Ministry of Health.
Attitudes and practices towards oxytocin and other uterotonics
Healthcare providers described oxytocin as the gold standard drug for PPH and an essential medicine. Some elaborated to suggest that there are heightened measures to ensure constant availability of the drug.
“Other drugs we frequently face those kind of stock outs…but there are some drugs which are considered to be very essential and the things they (the government) give priority and oxytocin is one of them. It’s very rare to run out of oxytocin.” – Obstetrician, tertiary hospital, Addis Ababa.
In health facilities, oxytocin was reportedly used for all women as part of AMTSL, delivered at a dose of 10 IU either intramuscularly or intravenously. Despite these reports, some healthcare providers described the barriers to delivering an injection of oxytocin during the third stage of labour. The necessity to have a suitably trained assistant during delivery to administer the injection of oxytocin was cited as a barrier to timely administration of the drug. Additionally, an obstetrician elaborated to describe the risk of needle stick injuries when trying to administer oxytocin under these circumstances.
“Sometimes we may face difficulties associated with the injection. While mothers are in labor….it may be hard to get persons to assist you, in this case you can inject yourself or other persons unnecessarily (by accident). For this, some students and staffs have started the antiretroviral therapy.” – Obstetricians, tertiary hospital, urban area, Oromia.
Community attitudes towards inhaled and injected medicines
Comments from community members about their knowledge of inhaled medications were relatively evenly weighted between those with an awareness and those who were unfamiliar with this drug delivery route. Most respondents who were familiar with inhaled drugs cited asthma medications as known inhalers and many expressed positive opinions towards these medicines based on the ease of use compared to injections. Others held positive view towards inhaled drugs based on their perceptions of the efficacy and speed of onset of inhaled asthma medications.
“One day someone got sick in our village and she was provided the injection but there was no change in her health. Later, we bought this [asthma] medication from the pharmacy and gave her. She became normal.” – Health extension worker, Gambella.
Conversely a common attitude expressed by community members was a fear of injections. In most cases, this fear related to the pain associated with the injection. A few community members also suggested that patients’ fear of injection compromised health-seeking behaviour.
“Since the injection causes pain, many people fear syringe even when they get sick they don’t want to go health institution due to fear of syringe.” – Health development army member, Oromia.
Product acceptability
Reported willingness to use
Responses to an inhaled oxytocin product were predominantly positive, and expressions of praise or willingness to accept this type of product were voiced in almost all FGDs and IDIs conducted across all regions and amongst all participant groups in this study.
Participant 6: “If the health professionals provide me [this inhaler], I will use it. To be saved from excessive bleeding, I will use it properly.” Participant 2: “I will use it too.” – FGD with mothers, Oromia.
While most participants expressed an unconditional willingness to accept this type of product, some healthcare providers described the need for published evidence to show an inhaled product exerts a similar physiological response and has a comparable pharmacokinetic profile to the injectable product.
Perceived benefits
The predominant benefit described by healthcare providers, community members and policy makers was that an inhaled product would be easy to use. Often, this was considered a benefit because it allows oxytocin to be administered by any individual with appropriate training (not necessarily a skilled birth attendant), thereby widening access to mothers who cannot access a skilled attendant for birth.
“Because it is easy to use and can be stored anywhere, it can be applied by anyone who is trained, not only professionals.” – Traditional birth attendant, Afar.
Some healthcare providers suggested that the ease of product use would facilitate considerable time-savings for birth attendants if the dose could be prepared with fewer steps compared to an injection. This was said to raise the possibility of task-shifting oxytocin administration to the mother, while the healthcare staff attend to other aspects of delivery management.
Most healthcare providers and policy makers described the heat stability as a the most significant benefit of an oxytocin inhaler. Providers from Afar and Gambella were particularly vocal on this point and expressed the need for a product which can withstand the high temperatures of these regions (>40 °C). Some providers elaborated to acknowledge that a heat stable oxytocin product may exhibit improved efficacy compared to the injection because its quality will not be impaired by inconsistent cold storage. Representatives from within the supply chain suggested that a heat stable oxytocin would be of benefit for its ability to release space in constrained cold chain systems.
“If it is thermo-stable in that way, that’s the best advantage you can get. As I mentioned, all those cold rooms that we are building can be used for other things like insulin and the like.” – Supply chain informant, Ministry of Health.
Concerns
The most significant concern for healthcare providers related to the fact that patient cooperation is required for administration of an inhaler. The anticipated issues associated with engaging the mother for oxytocin administration via inhalation were raised by approximately half of the healthcare providers participating in the study. In many cases, providers expressed their concerns for trying to administer an inhaler if the mother is unconscious after delivery.
“But as a weakness this medication needs a cooperation from the clients to administer it, for instance if the patient is unconscious she couldn’t cooperate…so we couldn’t administer this medication….” – Doctor, urban clinic, Oromia.
Additionally, there were some providers and key informants who explained that, after a long history of use, healthcare personnel trust the oxytocin injection and may be hesitant to believe that a novel oxytocin delivery route has equivalent efficacy.
“You know, health professionals have this inner shell of keeping things that they used to do. They’re used to giving injections, makes them feel oxytocin injection is the best. When you give the inhalation, even though they know this is like asthma, such an inhalation, there could be resistance, especially mid-level professionals who might think that this could be less effective.” – Policy-maker, Ministry of Health.
In a similar manner, some community members speculated that patient resistance may arise in response to a new or unfamiliar product. A grandmother suggested that formulating oxytocin as a tablet (which is more familiar) would therefore be advisable. However, several other community members suggested that providing education would be sufficient to overcome resistance of a new drug delivery route.
Use setting acceptability
Healthcare facilities
Many healthcare providers expressed their opinion that the most significant benefit of a heat-stable inhaled oxytocin product would be realised at lower level facilities such as health centres and health posts, as these facilities lack reliable access to cold storage for the oxytocin ampoule. Availability of the product in these settings was described as important to assure widespread access, particularly those in rural areas.
“If it is available only in hospitals and pharmacies, those from rural and remote areas cannot get it easily… so it is better if available in health posts and health centers.” – Religious leader, Oromia.
Several stakeholders also acknowledged the benefits that this type of product could offer at better-resourced facilities such as hospitals. In most cases, the benefits of an inhaler in these settings were described in terms of the capacity to avoid the risks associated with injections. Some providers also suggested that a heat-stable product would also be of benefit for higher level facilities, which also face cold storage constraints.
Attended out-of-facility deliveries
Healthcare providers and community members suggested that an inhaled oxytocin product should be used by health extension workers at out of facility deliveries as a means to expand access to oxytocin, particularly to women in rural areas, who are often unable to reach a facility for delivery. However, some healthcare providers and key informants felt it important to highlight the context in which this type of product should be given to these health workers. In line with government efforts to promote institutional deliveries, it was suggested that uterotonics should be used by health extension workers in emergency situations only, rather than to enable them to routinely attend out-of-facility deliveries. This attitude was particularly prominent for a representative from within the Ministry of Health, who citied government policy that prohibits these health workers from attending births.
“But our health extension workers are not allowed to attend deliveries. Fully. They used to attend deliveries – ‘clean and safe deliveries’. Kind of a backup. [But] we don’t encourage any program that provides an opportunity for health extension workers to attend delivery.” – Policy-maker, Ministry of Health.
However, other key informants from the Ministry explained that there are plans to upskill health extension workers to the level of skilled birth attendant and give authorisation to attend births outside of facility settings.
Unattended out of facility deliveries
Some community members described the importance of making an inhaled oxytocin product available for births that occur outside of healthcare facilities, even those that are not attended by a health extension worker. In most cases, this was described as necessary for emergency situations where a woman is unable to reach a healthcare facility or access a healthcare provider in time for delivery.
“If we decide to keep this inhaled oxytocin only in health centers, we are denying access to most of the rural community who have a transportation problem to reach to the health facilities.” – Community leader, urban area, Gambella.
This attitude was expressed similarly across participants from urban and rural areas, however, it seemed to be a particularly salient point for community members from Gambella and Afar when compared to Oromia.
Many healthcare providers explained that use of an inhaled oxytocin product at out of facility deliveries does not align with government policies or their own opinion that institutional deliveries should be promoted. Even if provided for emergency situations (where a woman is unable to reach a healthcare facility), healthcare providers feared that the mere accessibility of this type of product to community members would encourage out of facility deliveries.
“If you are at home you cannot have access to an IV line, blood, antibiotics and so on. So people should deliver in hospital. Period. Or in a health centre… If someone asks my opinion about giving this [inhaled oxytocin] to home deliveries I would say no.” – Obstetrician, Addis Ababa.
Discussion
Subject to complete clinical testing, a heat stable, simple to use inhaled oxytocin has the potential to expand access to a quality uterotonic for the prevention of PPH in low-resource settings and thereby improve maternal health outcomes in countries where the highest burden currently rests.24 The current study explored the potential acceptability of an inhaled oxytocin product for the prevention of PPH in Ethiopia.
Recognising that the acceptability of a new product will be grounded in the existing attitudes and belief structures of end-users, we explored knowledge, attitudes and practices surrounding the context within which an inhaled oxytocin product would be positioned. This included knowledge, attitudes and practices towards comparable products (other uterotonics and inhaled medications) and the condition for which this type of product is designed (PPH and postpartum bleeding). In this study community members, healthcare providers and policy-makers expressed a concern for postpartum bleeding and PPH was recognised to be the leading cause of maternal mortality in the country. This finding is supported by previous research in Ethiopia showing that bleeding during childbirth is one of the most commonly known danger signs amongst community members.25–27 The existing concern for the gravity of PPH will likely improve acceptability of an innovation for PPH prevention, as previous reviews have shown that adoption of a novel product or program is facilitated if it addresses an issue that is experienced or prioritised by adopting stakeholders.28,29 Further, amongst healthcare providers, there was a recognition that oxytocin is the gold standard drug for PPH prevention, thus an inhaled oxytocin product may be acceptable to these stakeholders when compared to a completely novel drug molecule. However, the existing trust in the oxytocin injection currently available may equally serve as a barrier to adoption of an inhaled product, particularly amongst healthcare providers, who may be reluctant to accept a new oxytocin administration format. Taken together, these findings will guide the design of appropriate advocacy strategies based on existing attitudes and knowledge gaps. For example, limited emphasis may need to be placed on raising awareness about PPH, since the condition is well recognised. However, it will be important to make available sufficient evidence to demonstrate that an inhaled product has the equivalent safety and efficacy to the injection in order to assure acceptance of a novel administration format from healthcare providers.
Acceptance and adoption of an innovation will be facilitated if it has a significant and observable advantage over current alternatives.28,30 An inhaled product may be viewed by healthcare providers as advantageous due to the difficulties associated with administration of the oxytocin injection that were described by some participants of this study (shortages of birth attendant time or availability of trained assistants). Similar difficulties with timely administration of oxytocin injection have been previously reported in several low-resource settings.31–35 Thus, the acceptability of inhaled oxytocin amongst healthcare providers will be enabled, if the product is viewed as easy to use and suitable for task shifting to lower-tier delivery assistants. These findings will support product development activities with regard to device selection, which will need to give significant consideration to user handling factors in addition to technical performance and cost.
Amongst community members, an inhaler may be accepted as more advantageous than the current injection, as inhaled medications were generally viewed as fast-acting and easy to use. In contrast, injections were often described as less favoured due to pain and infection-related side effects. While these findings are in contrast to several previous studies highlighting a strong patient preference for injections in the developing world,36–38 studies conducted in Ethiopia have found injections to be the preferred administration format in only 15-42% of studied populations.39–41
Ease of product use and heat-stability were the most significant anticipated advantages of an oxytocin inhaler cited by all stakeholders, who largely expressed a willingness to accept and use this type of product as long it had equivalent efficacy to the injection. However, concerns or perceived pitfalls are equally important to understand. The most significant concern from healthcare providers was that patient cooperation would be required for administration of oxytocin from an inhaler, and that cooperation may be difficult to attain from women during the third stage of labour. Similar concerns were expressed by community members and by some healthcare providers participating in this research program in Myanmar.42 Thus ensuring that the inhaler can be feasibly administered immediately after childbirth will be an important for product acceptability. In this respect, selection of an inhaler device which has low airflow resistance and an intuitive operation mechanism will be critical to ensure that women in the third stage of labour face minimal challenges to using the inhaler. In addition, product introduction plans should include training for pregnant women in the lead up to childbirth to ensure the mother has a familiarity with how to use the inhaler.
The findings of this study highlight the importance of identifying an acceptable setting for use of an inhaled oxytocin product. Community members in particular welcomed the possibility of making the product available outside of health facility settings, thereby expanding access to life-saving care for women who are unable to reach a facility to give birth. However, product use in this setting is unlikely to be acceptable to policy-makers and other health system stakeholders, who suggested that this distribution strategy would not align with government policy to promote facility-based deliveries. Similar issues have hampered the scale-up of community distribution programs for an orally administered uterotonic, misoprostol, in Nigeria, Mozambique and Ethiopia.43–45 An opportunity for an inhaled oxytocin product to expand access to oxytocin at out of facility deliveries may be presented by the health extension workers. This cadre of health worker was established in 2003 to provide community-based primary health care, including health education, screening as well as basic preventative and curative services.46 However, at the time of this study political support for these health workers to attend deliveries was uncertain. While the Health Sector Development Program (HSDP)-IV (2010-2015) set a target to have 38% of births attended by health extension workers,47 a federal policy-maker engaged for this research downplayed support for this program in preference for promotion of institutional deliveries. It is likely that acceptability of an inhaled oxytocin product for use by health extension workers will hinge on current programs to upskill these health workers to the level of a skilled birth attendant.48
Strengths and limitations
A notable strength of this study is the investigation of user attitudes and perceptions of the context within which an inhaled oxytocin product will be positioned. For example, researchers explored existing attitudes towards oxytocin or inhaled medicines before providing a detailed description of an inhaled oxytocin product, such that these existing attitudes could be used to triangulate the opinions that participants expressed towards the product. This served to limit the impact of response bias that may arise from participant desire to please researchers by expressing acceptance of the product in question. Further, care was taken to mitigate investigator bias by moderating the involvement of members of the inhaled oxytocin product team in the study. Data collection and analysis was largely carried out by independent researchers, who provided an impartial and objective perspective.
The timing of this study is considered by authors to be a strength, in that understanding the potential acceptability of a product highlights opportunities that can be leveraged and barriers that should be mitigated when designing an introduction strategy. However, a limitation associated with this approach is that acceptability can only be hypothesised and it is likely that unforeseen barriers or enablers may arise when the product is used in practice. Implementation research conducted alongside product introduction will be important to further explore the acceptability of an inhaled oxytocin product in low-resource settings.
Conclusions
This study explored the potential acceptability of an inhaled oxytocin product for the prevention of PPH in Ethiopia. Findings highlight that this type of product is likely to be largely acceptable to policy-makers, end-users and beneficiaries due to existing concern for the disease condition, positive attitudes towards inhaled medications, and the perceived benefits of an inhaled oxytocin product (heat stability and ease of use). Risks to acceptability could be posed by practical issues associated with the use of an inhaler at the time of childbirth. Settings for product use should align with the health policy context in order to assure acceptability. Beyond providing an understanding of the possible user receptivity to an inhaled oxytocin product, the findings of this research can be used to support the design of appropriate implementation strategies that are well tailored to the distinct social and political context of Ethiopia.
Acknowledgements: The contribution of Yibeltal Kiflie to the interpretation of data from this study is gratefully acknowledged.
Funding: This study was made possible by the generous support of the Saving Lives at Birth partners: the United States Agency for International Development (USAID), the Government of Norway, the Bill and Melinda Gates Foundation, Grand Challenges Canada, and the UK Government https://savinglivesatbirth.net/; grant number: AIDOAA-F-14-00046). Additional funding was provided by Grand Challenges Canada and the Government of Canada (http://www.grandchallenges.ca/; grant number: TTS 0609-05). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Authorship contributions: The study was conceived by VLO, PL and MPM. The protocol was developed by VLO with input from PL, AMT and MT. Data collection was carried out by VLO, PL AMT and MT. Data analysis was conducted by VLO, MT and AM. All authors contributed to interpretation of findings. The manuscript was written by VLO with input from all authors.
Competing interests: The authors have completed the Unified Competing Interest form at www.icmje.org/coi_disclosure.pdf (available upon request from the corresponding author) and declare no conflicts of interest.
Corresponding author:
Michelle McIntosh
381 Royal Parade
Parkville, VIC, 3052
Australia
[email protected]