Increasing life expectancy has been a key contributor to the surge of dementia cases globally, with low- and middle-income countries (LMICs) bearing a disproportionate burden. 1 In Iran, the number of adults aged 60 and above is exponentially increasing. In 2015, there were 6.5 million adults over 60; this number is projected to increase to 12.9 million in 2030 and to 30 million in 2050. 2 Assuming the most up-to-date national prevalence estimate of 7.9% remains stable, the number of people with dementia would rise from 513,000 in 2015, to 1.02 million in 2030, and 2.4 million in 2050. 3
Like many LMICs, Iran currently does not have a national strategy for tackling its rising dementia epidemic. Knowledge of the condition has not been well integrated into the country’s medical and health curriculums, and has not been addressed by continuous education programs. As a result, the number of health care professionals and facilities equip to recognise, diagnose, treat, and support patients through the illness remains low, and is unequally distributed across the country. These have in turn led to the low dementia diagnostic rate of 21% (range: 9.7% in Khuzestan to 40% in Alborz). 3
Memory Clinics in Iran, MCI Initiative
The Memory Clinics in Iran (MCI) Initiative was designed to address this gap in dementia knowledge amongst health and medical professionals in Iran. It aims to:
-
provide short-term training on cognitive impairments and dementia to interested medical and healthcare professionals to help improve dementia preparedness within Iran’s health workforce;
-
promote collaboration amongst medical and healthcare professionals across different fields and specialisations to work towards integrated care for people with cognitive impairments and dementia;
-
create a human resource platform for cognitive impairments and dementia in Iran made up of program graduates and other experts with dementia training;
-
raise dementia awareness and interests amongst medical and healthcare professionals;
-
inspire and encourage medical and healthcare professionals to work in the field of cognitive impairments and dementia;
-
create career opportunities for medical and healthcare professionals in the field of cognitive impairments and dementia;
-
support program graduates and other health and medical professionals to initiate or contribute to setting up further memory clinics across the country to improve Iran’s capacity for the early detection and management of dementia.
The initiative was led by Professor Maryam Noroozian and her team at the Cognitive Neurology and Neuropsychiatry Division of Department of Psychiatry at Tehran University of Medical Sciences. Professor Noroozian is a pioneer of dementia research and clinical practice in Iran and set up the country’s first memory clinic in 2003.
The MCI Initiative was piloted in September 2017. The pilot (Table 1) was jointly supported by the Tehran University of Medical Sciences (TUMS) and offices of Elderly Population and Rehabilitation, the Ministry of Health, and Institute for Cognitive Science Studies (ICSS) of Iran. The launch of the initiative was conducted in the presence of the special guests from the United Nations (UN) and United Nations Populations Fund (UNFPA) Iran representatives, Institute for Cognitive Science Studies (ICSS), Ministry of Health, professors of TUMS, and other universities with messages of endorsement from academics from New York University, University of Louisville, Northwestern University and the University of Edinburgh.
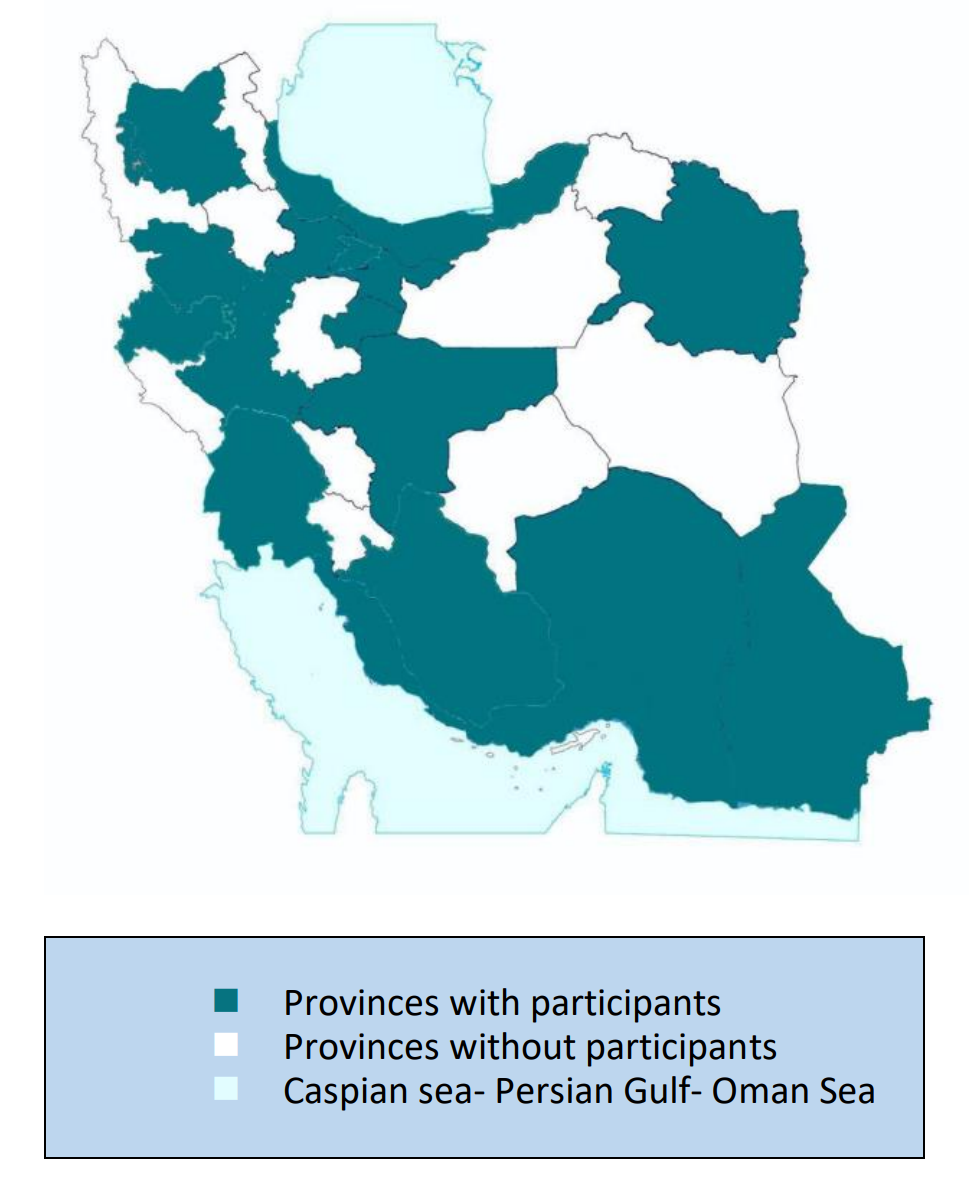
The pilot program was held in Tehran from September 2017 to April 2018. Virtual social networks, including Telegram, Instagram, and WhatsApp, were used to recruit participants. 152 health professionals from 19 provinces of Iran’s 32 provinces participated in the course (Figure 1). These participants came from diverse disciplines, including psychology (31.3%), psychiatry (20.6%), neurology (18.6%), general practice (8.6%), neuroscience (4.6%), geriatric, and other health sciences (13.3%). Participants were requested to submit proof of their educational status and assessed for programme eligibility prior to acceptance into the programme. Due to feasibility constraints in delivering the pilot, not all who were eligible were accepted. The applicants from unrelated specialties (24 applicants) were excluded, as well as the applicants who registered after the deadline.

The pilot was offered at a low cost thanks to partner support, including provision of a teaching hall by the Tehran University of Medical Sciences. Since the conclusion of the pilot, the MCI Initiative has received many requests from health professionals throughout Iran to provide further training for those who were unable to participate in the pilot. There were also request for more advanced modules from graduates of the pilot course.
Nonetheless, there were a number of limitations worth mentioning. While there was a diversity of specialties amongst participants in the pilot, this variation was due to self-selection by interested participants. Only a small percentage of participants were from general practice. Yet, there is evidence to show that when dementia care is dominated by specialists such as geriatricians, neurologists, and psychiatrists, providing sufficient coverage for the growing number of people affected by dementia becomes difficult and costly. Provision of continuing care and management of dementia by knowledgeable general practitioners is a practical and cost saving way to extend coverage of dementia diagnostics and treatment within the population as the epidemic progresses. 1 Thus, further programs should target training general practitioners to equip them with the necessary skills for this important task.
The MCI Initiative will continue, and further stages will explore more effective ways to target and attract primary care practitioners. The success of the pilot has prompted the authors to seek funding for the continuation of the program, as well as to have the MCI curriculum integrated into the academic curriculum run by the Research Centre for Dementia and Cognitive Disorders at Tehran University. In addition, the lead author is developing a Dementia Fellowship Programme for training medical specialists in dementia. The original cohort continues to meet to discuss and present cases, and will serve as support for future cohorts. As the programme scales-up, health care workers in under-represented provinces will also be targeted.
The MCI Initiative can serve as a useful model for other LMICs experiencing a heavy burden of dementia among their population. With rising non-communicable diseases (NCDs), which are a risk factor for dementia, and a growing portion of the population living longer across the world, including in LMICs, programmes such as the MCI Initiative are necessary to ensure that the vulnerable elderly have access to prompt diagnosis, and are provided with adequate health care.
Authorship contributions
All authors contributed to, read and approved the final manuscript prior to submission.
Competing interests
The authors completed the Unified Competing Interest form at www.icmje.org/coi_disclosure.pdf (available upon request from the corresponding author), and declare no conflicts of interest.
Correspondence to:
Maryam Noroozian, MD
Professor of Neurology
Director, Memory and Behavioural Neurology Division
Roozbeh Hospital, South Kargar Avenue, 1333795914, Tehran, Iran
[email protected]