

The world presently experiences a critical shortage of health workers, with a projection of an undersupply of over 10 million by 2035.1 Community health workers (CHW) are increasingly seen as important members of, or adjuncts to, the global health workforce, assuming responsibilities for basic or even more advanced provision of primary health care. CHWs are generally considered to be cadres of workers “who receive standardized training outside the formal nursing or medical curricula to deliver a range of basic health, promotion, educational, and outreach services, who has a defined role within the community system and the large health system” 2; they are well established in many low- and middle-income countries (LMICs). Some countries with national CHW programs are Brazil, India, Nepal, Ethiopia, Pakistan, Bangladesh, Iran, and Afghanistan.3–7 These large-scale CHW programs aim to address a chronic shortage of health workers, yet evaluations of their performance are typically carried out using data from individual CHWs such as qualitative interviews and/or randomized surveys at a specific point in time rather than continuous administrative and programmatic database.8,9 In most of these countries, the CHW program started as a pilot project and scaled up over time. In these expansion processes, it is often forgotten to integrate the program into the national health information systems, yet monitoring and evaluation of health programs depend on regular information gathering and analysis. Potential quantitative research on national CHW programs using health-related administrative datasets is limited to few countries with national community health systems. However, most available data of CHWs are not disaggregated based on geography, population size, and gender. This could be due to the health information component of CHW programs being underdeveloped, of poor quality, or unavailable. It might also reflect that CHW programs have yet to be viewed as an integral part of national health systems.
In this paper, we use a case study of Afghanistan, where national health datasets on CHWs and their activities are available and the program is regarded as part of its national health system. The Afghan government in 2003 with support from international donors initiated a national program called the Basic Package of Health Services (BPHS), which included training volunteer CHWs in rural areas to expand access to basic health services. CHWs provide basic health services to the rural communities, facilitating community members access to the formal health system to which they had earlier little or none. At the same time, a health management information system (HMIS) was developed to track the implementation of the BPHS across the country, including administrative data on CHW activities.
The size and distribution of Afghan national CHW program is comparable with a number of other national programs, depending on the size of the population they cover (Table 1). Afghanistan’s approximately 23,500 CHWs serving a rural population of around 19 million is comparable with Iran’s 31,000 Behvarz (An Iranian title for CHWs), who serve an estimated 23 million rural residents.7 In most countries, a CHW has the responsibility of around 750 to 1000 individuals, except in Ethiopia where a Health Extension Worker covers around 2,500 individuals. But Ethiopia’s Health Extension Workers lead a group of ten volunteer community health workers.9
The goal of this paper is to describe the overall performance of the Afghan national CHW program using data from the HMIS. In this paper, we describe the number of CHWs, their distribution and activities, and maternal and child health outcomes, addressing three important health systems questions:
-
How many CHWs are working across the country, and how are they distributed based on geography and population size?
-
What are the frequencies of activities CHWs undertake and the ratios of their activities by population size and geographic distribution?
-
What is the ratio of maternal and neonatal mortality rates by population size and CHW density?
Although antenatal and postnatal care and referrals of complicated deliveries to health institutions contribute to better maternal and health outcomes 10, the causal relationship between the activities of CHWs and maternal and child health outcomes in Afghanistan is not an objective of this study. Improved maternal and child health outcomes in Afghanistan have many social determinants beyond the health services.11 Findings from this study have implications for more system-wide evaluations of CHW programs in other similarly resource-constrained countries.
METHODS
This study is a descriptive quantitative analysis using a large administrative database linked to population census data from Afghanistan. The country’s HMIS has a Microsoft Access database where information is stored regarding the implementation of primary health care, including the national CHW program across the country. Developed in 2003, the HMIS was revised twice to include comprehensive information on health services.
Dataset extraction and data cleaning
After consultation with HMIS officers in Kabul, we chose to analyze data from 2009 onward as HMIS officials indicated that data quality and comprehensiveness had improved significantly by 2009. The Afghan Central Statistics Office (CSO) gathers census data and makes the data public without any personally identifying variables. Using the health and census databases, the following variables are included in this study (Table 2), and described more fully below.
To describe the activties of CHWs and maternal and child health outcomes, district was chosen as the unit of analysis as the smallest geographical unit for which data were available in both datasets. Within each district we had access to total population numbers by sex and for each of the years 2009 – 2012. The data on districts of Afghanistan were retrieved from the national census dataset of the Afghan Central Statistics Office. As the CHW program was intended only for rural populations, we included only those districts with a rural population in the national census dataset, excluding areas identified as urban by the Afghan Central Statistics Office.
The variable to enumerate the existence of CHWs in a village is the number of health posts. A Health Post is a house in a village where two CHWs are based. CHWs have many tasks, but only four of those tasks are recorded in the databases:
-
Normal delivery referral is the number of normal deliveries referred by the two CHWs in a Health Post to a health facility;
-
Obstetric complication referral is the number of pregnant women with obstetric complications referred by the two CHWs in a health post to a health facility;
-
Antenatal visits are the number of visits the two CHWs in a health post make to pregnant women in their coverage area, and
-
Postnatal visits are the number of visits the two CHWs in a health post make to women who recently delivered babies in their coverage area.
These variables are indicators of the existence of and activities by CHWs in a district.
Data are reported annually from 2009 to 2012 (the equivalent of Afghan/Persian years of 1388 to 1391) in this analysis. Since the number of health posts was reported every month, to find the number of active Health Posts in a year, the median number of Health Posts reported over 12 months was chosen because an outlier in a month would dramatically change the mean. In addition, tests of normality on all health-related variables indicated a significant deviation from normal distribution (Kolmogorov-Smirnov Sig<0.001 and Shapiro-Wilk Sig<0.001) (Appendix S1 in the Online Supplementary Document). Other health services and activity variables were summed for each year. For example, the number of normal delivery referrals by CHWs monthly was summed over 12 months to give the annual cumulative number. The initial two years of data did not have antenatal and postnatal visits by CHWs because those activities were only included in the terms of reference for CHWs starting in 2011.
Data analysis
We performed a number of descriptive analyses to address our study objectives. Results are presented by year. The number of CHWs, the frequencies of their activities, and the number of maternal and neonatal deaths are reported as ratios relative to population size (per 10,000 individuals) to help understand the distribution of workers, their activities, and health outcomes across the country over time. We also report the activities and health outcomes as ratios relative to the number of Health Posts in districts to shed light on the relationship between service burdens and health outcomes.
Geographical mapping
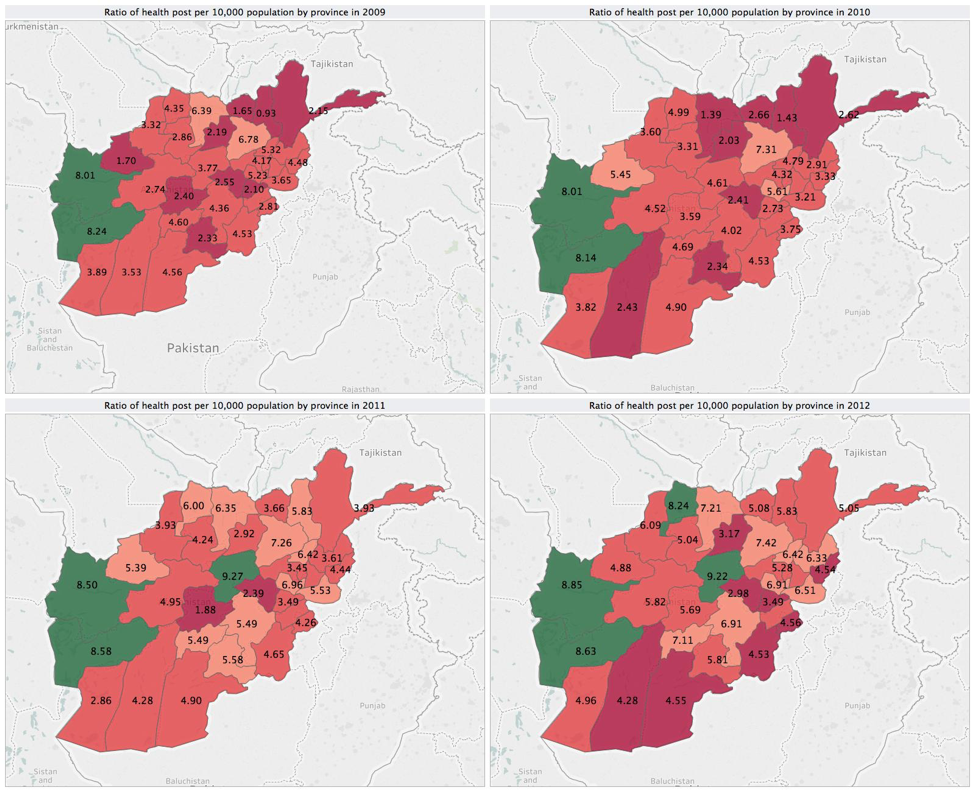
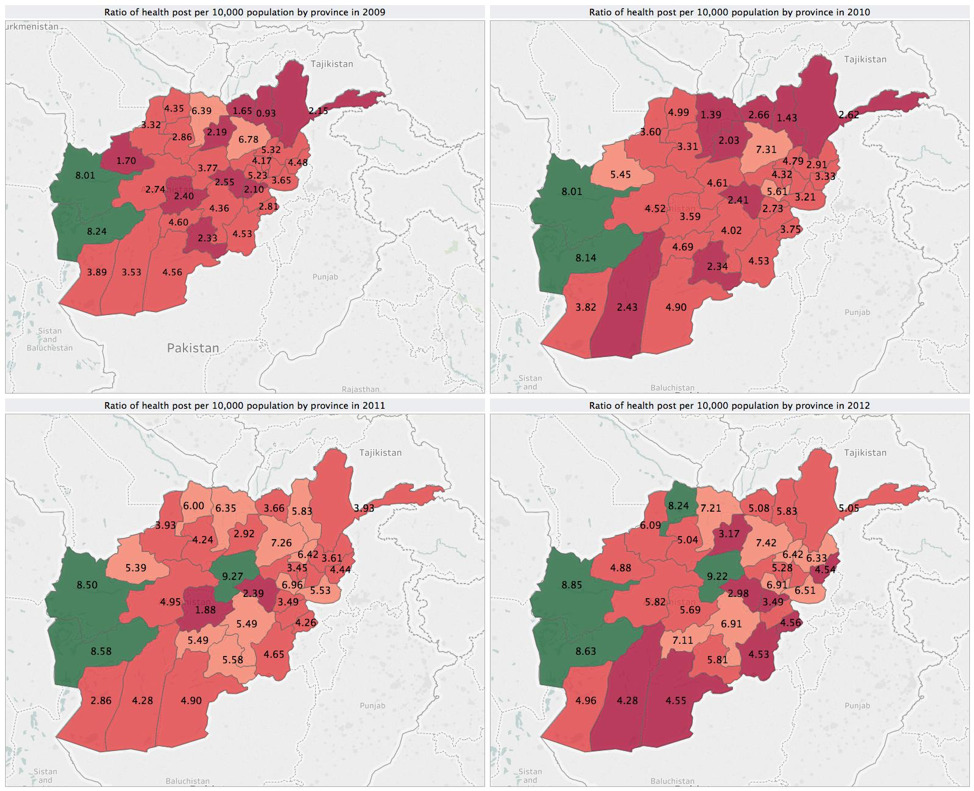
Tableu Software (Tableu Software, Seattle, WA, USA) was used to map the data geographically. According to the BPHS policy, a Health Post has a catchment area of 1,000 to 1,500 people (average 1,250). We mapped the number of health posts per 10,000 individuals. To present the data by province, the median numbers of Health Posts per population in districts were added to create the median number of Health Posts per province. Eight or more Health Posts per 10,000 population (or one Health Post per at least 1250 people) was considered adequate to cover the population by the BHPS/CHW program policy (Figure 1). Provinces that did not meet the policy standard of 8 health posts per 10,000 individuals in the population were further categorized into tertiles based on their health post ratios, as having a somewhat low (Colored Peach - below 8 but above 5.34 health posts per 10,000), low (Colored Blush Red - below 5.34 but above 2.67 health posts per 10,000) or extremely low (Colored Dark Red - below 2.67 health posts per 10,000) number of health posts relative to population size (Figure 2).
Data quality
Evaluating the quality of data from developing countries can be challenging. One way to assess quality is to examine the step by step process of data collection. The data of the HMIS were collected by CHWs. CHWs were provided with a pictorial tally sheet (Appendix S2 in the Online Supplementary Document) to record their activities and some major health indicators such as maternal and neonatal death on a monthly basis. The tally sheet has a box for each indicator including antenatal and postnatal visits at home, normal delivery referrals, obstetric complication referrals, maternal death, and neonatal death. At the end of the month, CHW supervisors record CHWs’ pictorial tally sheets in another form called the Monthly Activity Report (MAR) (Mar (or Maar) in Persian means snake. The data collection form MAR is known as the small snake, and MAAR as the large snake. It signifies two things: first, a large form that collects data on activities of the CHWs from the communities; and second, a chain through which information is carried to the highest level at the Ministry of Public Health). The supervisors combine the monthly activity report from all their CHWs into another form called the Monthly Aggregated Activity Report (MAAR). These forms are then entered into a provincial HMIS database and sent to the national Ministry of Public Health in Kabul. The provincial HMIS is manually updated into the national HMIS every quarter of a year. At the end of the year, the national HMIS office receives a paper copy of the Monthly Aggregated Activity Report to crosscheck with the provincial HMIS.
To examine the validity of the national HMIS data, the 2012 Monthly Activity Report and Monthly Aggregated Activity Report forms from 16 Health Posts and nine health facilities in eight districts of four provinces were collected during fieldwork in 2013. Data from the Health Posts were cross-checked with data at the health facilities, and from health facilities with the HMIS database. The aggregated data from one level matched the higher level of data, supporting the quality of the HMIS database at least in terms of its accurate representation of the monthly reporting forms.
RESULTS
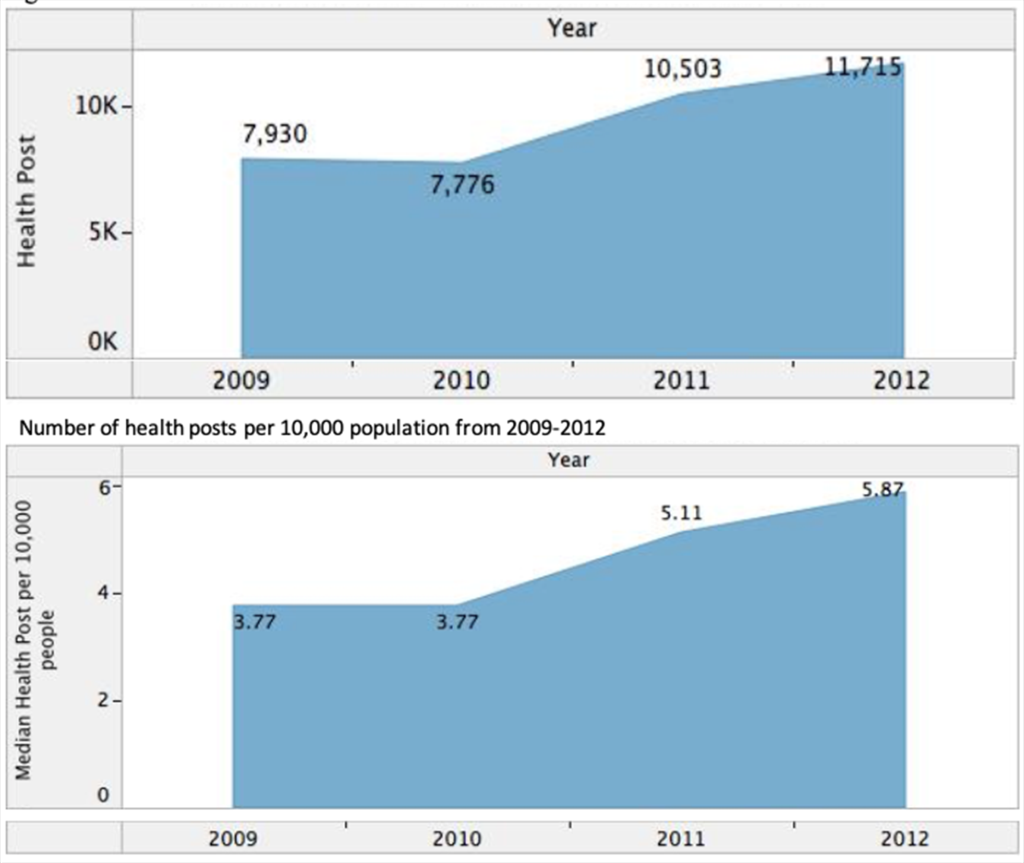
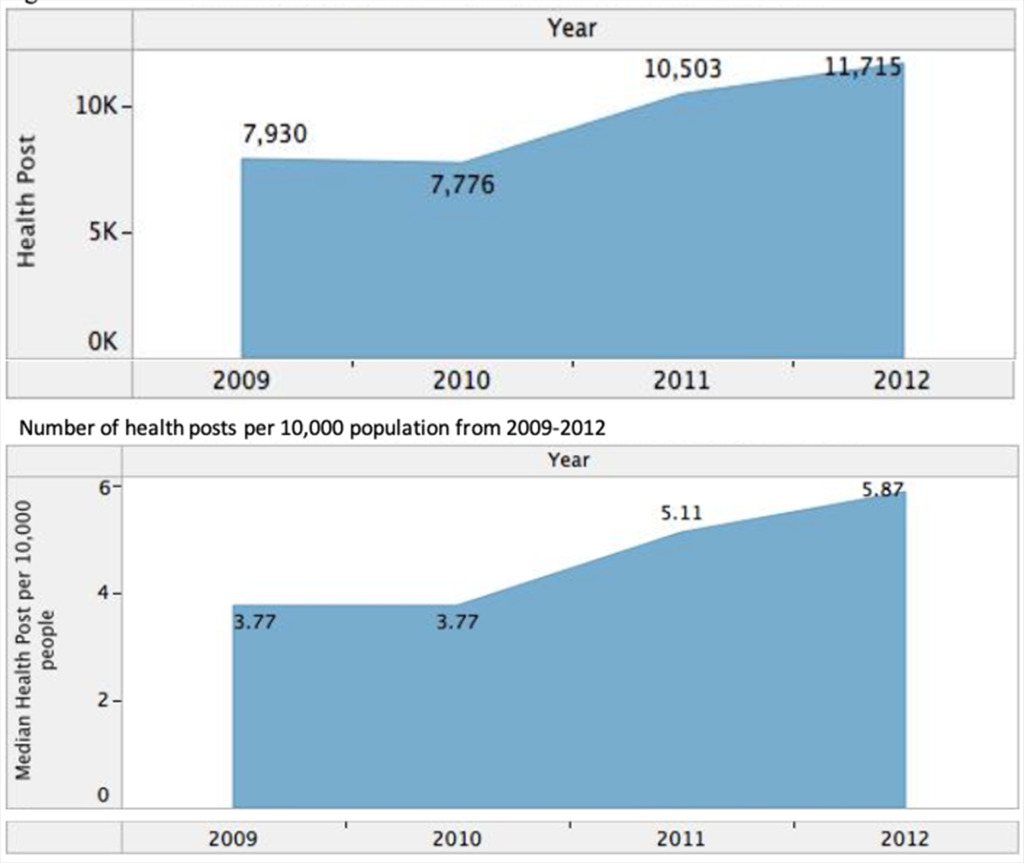
Figure 1 illustrates that the number of Health Posts and their ratio to population size increased over the four year period from 7,930 (3.77 per 10,000 individuals) in 2009 to 11,715 (5.87 per 10,000 individuals) in 2012, following a slight downward slope in 2010.
Geographical Distribution
Figure 2 shows the distribution of Health Posts per population in all provinces from 2009 to 2012. In 2009, two western provinces had reached the ratio of 1 Health Post per 1250 people, increasing to 4 provinces in 2012 with inclusion of a northern and a central province in the list. The ratio has shown some improvement in the north eastern provinces, but decreased in southern provinces.
Service Delivery
Figure 3 shows the numbers of referrals and home visits made by CHWs in a given year. Absolute numbers of all service delivery activities increased over time. In 2012, over 133,000 normal deliveries and over 28,000 obstetric complications were referred to health facilities by CHWs. In that same year, CHWs made approximately 400,000 antenatal visits and 261,000 post natal home visits.
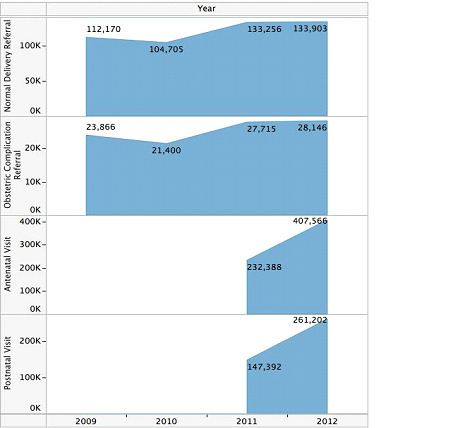
Ratios of referrals and home visits by population size and health posts for each year are shown in Table 3. While the number of normal delivery referrals per 10,000 people in the population increased from 2009 (approximately 65 referrals per 10,000) to 2012 (approximately 72 referals per 10,000 population), the number of normal delivery referrals per health post decreased slightly during the same time period, from approximately 14 (2009) to approximately 11 (2012) referrals for each health post per year. Referrals for obstetric complications referrals by population size showed a slight decrease between 2009 and 2010 from 14 to 13, but increase in 2011 and 2012 to 16 referrals per 10,000 people. In the mean time, the number of obstetric complication referrals by health posts decreased over time from approximately 3.3 referrals per health posts in 2009 to approximately 2.6 referrals per health post in 2012. The number of antenatal and post-natal home visits increased significantly in relations to both population size and numbers of health posts from 2011 to 2012 (Table 3).
Health outcomes
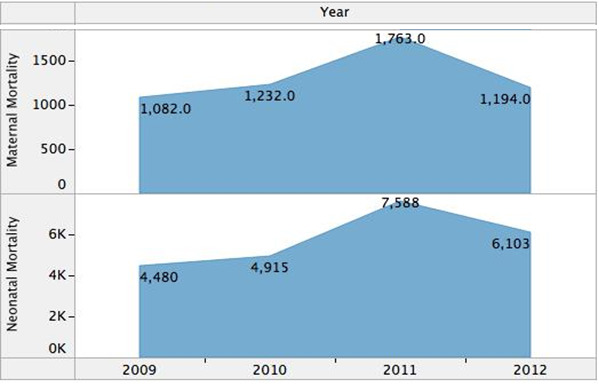
From a starting point of 1,082 maternal deaths in 2009, the number of maternal deaths increased in 2010 (1,232) and 2011 (1,763), and then dropped in 2012 (1,194) (Figure 4). The number of neonatal deaths started at 4,480 in 2009, increased in 2010 (4,915), notably increased in 2011 (7,588), and then decreased in 2012 (6,103). Ratios of maternal and neonatal deaths to total population shows some increase from 2009 to 2011 and a decrease from 2011 to 2012 (Table 3). The ratio of maternal and neonatal deaths per health posts, however, shows a steady decrease between 2009 and 2012 (Table 3).
DISCUSSION
Our findings demonstrate an increase in the number of health posts and an increase in service delivery by CHWs in rural Afghanistan from 2009 to 2012. With some fluctuations, we identified overall increases in absolute numbers of maternal and neonatal deaths over time from 2009 to 2011 and decreases from 2011 to 2012. When presented in relation to fluctuations in population size, these trends were less clear.
The large volume of activities that Afghan CHWs undertake is valuable mainly due to a lack of professional providers in those settings. Moreover, CHWs provide more services than the four activities related to maternal health that are analyzed in this study. They dispense drugs for prevalent health conditions such as headache, fever, pneumonia and diarrhea, refer non-pregnancy related patients to clinics, provide health education, promote family planning, and personal sanitation. Those activities are not recorded in the HMIS. More importantly, Afghan women in rural areas have a tradition of giving birth at home and avoid seeking professional health services even in severe cases of complications, leading to high morality among women and newborns.12 CHWs’ impact on those practices could be lasting.
The distribution of Health Posts remains unequal across provinces. Although more provinces met the policy standard of 1 health post per 1,250 individuals in the population by 2012, most provinces were still below this ratio. The unequal distribution of Health Posts by population size across provinces may lead to unequal maternal and neonatal health outcomes. The findings imply that there were large pockets of populations who were not covered by Health Posts. As resources in the CHW program are allocated to all Health Posts equally, without any considerations to the number of people they covered, the findings suggest a significant mal-distribution of health resources, particularly medications in areas covered by Health Posts, where some populations under coverage of Health Posts were unlikely to receive the services and drugs they needed.
The findings on maldistribution of resources in this study is in line with other Afghan and non-Afghan health research. Previous studies on maternal and child health outcome found unequal distribution across the country, where mountainous and hard-to-reach areas had many times higher mortalities than rural areas close to towns and cities.10,13,14 We have not found empirical research on geographical and population distribution of CHWs in other countries. However, in most countries with national CHW programs, a CHW has the responsibility of around 750 to 1000 individuals based on their policies.9 A systematic review has found that heavier workload for CHWs influences the ability of CHWs to follow up their patients and leads to lower motivation and lower performance.15 These and our study findings suggest the need not only for more CHWs but also for more equitable distribution of CHWs and reasonable workload. Future studies can aim to identify those large and small pockets of populations who are not truly served by the Afghan program.
The decrease in maternal and neonatal deaths near the end of the observation period, i.e., from 2011-2012 is encouraging, although the absolute numbers remain higher than in 2009. Limitations in our data preclude us from drawing conclusions about the impact of CHW activities on mortality rates. For example, the increase in health posts per 10,000 total population, particularly in 2011 (Figure 1), could potentially have led to better outcome reporting, which could help explain the increase that year in reported neonatal and maternal mortality. Alternatively, it is possible that the general increase in service delivery that we observed over time may have an impact, either in these trends or in the future, on mortality rates. It is too soon to evaluate the impact of the inclusion of antenatal and postnatal visits to the task of CHWs in 2011 but there is the possibility that these health services have or will help to decrease deaths.
Large administrative datasets have advantages and limitations with respect to their value for health services research. Administrative datasets have large numbers of observations from a wide range of areas and frequently cover entire populations, giving researchers the ability to generalize their findings. The Afghan data from more than 300 districts covering 19 million people (2/3rd of the population) has the potential to allow a national level understanding of the breadth and reach of the CHW program, with researchers being able to identify structural or procedural weaknesses in the database, functioning as a third-party evaluator. Accessing administrative datasets has a low or non-existent cost. An implicit assumption in using administrative datasets is that a country recognizes CHWs as human resources for health, hence maintaining a dataset on their deployment.
One of the limitations of the Afghan administrative database was a lack of socio-demographic variables that could be used to analyze disparities in healthcare. The smallest unit in the database was a Health Post, not an individual, thus missing information on gender, age, education, income or ethnicity of users. We also did not have data specific to the number of pregnant women or total births in the population, which may have influenced some of our findings with respect to neonatal and maternal mortality and health service delivery. A general limitation of administrative datasets are a lack of data from areas not under the coverage of the program. In the case of Afghanistan, some districts were not under the control of the state, making this study not representative of the whole population, but the population under coverage of the program. Administrative databases also involve complex organizational procedures and human biases and reporting errors that may affect the quality of the data.
This study can be a baseline for future studies of CHWs in Afghansitan. Studies on health facilites in rural Afghanistan can link the referrals by CHWs to the tasks undertaken by professional providers. There is also a possibility to compare antental and postnatal visits undertaken by CHWs at home with the same services provided in health facilities. More importantly, this study can be used for future cross-country analysis of CHWs and indicates a need for standardization of quantitative data on CHWs to be leveraged for future multi-national studies.
CONCLUSION
Large administrative datasets are important data sources for research with a potential to offer valuable lessons for policymakers and health managers. To our knowledge, this is the first study to have described a country-wide CHW program using a large national administrative database. The findings indicate that a large volume of services are provided by CHWs to populations in need, that coverage of services in most of the country is still inadequate, and that the distribution of CHWs and their resources are inequitable within the country. Despite methodological and quality challenges, this study can be used as a baseline for future replications, a point of comparison for research on health facilities, and as a comparison for other countries. Importantly, the design we used for this case-study (drawing from a large administrative database) is one that we think could be usefully copied in many other countries increasing, improving, or revising their own CHW programs, especially in light of the international commitments to Universal Health Coverage (UHC) under the Sustainable Development Goals, and the efforts led by the World Health Organization and UNICEF to ensure that the principles of primary health care drive the UHC agenda.16
Acknowledgements
We thank the Afghan Ministry of Public Health, in particular Dr. Nawid Shams Bahristani, Dr. Ahmad Jan Naeem, and Dr. Daud Azimi for their support for this research. Ethics approval was received from the University of Ottawa and the Afghan Ministry of Public Health. Health Management Information System (HMIS) database is available through the Afghan Ministry of Public Health, and Afghan Census Data is available through the Afghan Central Statistics Office.
Funding
This work was carried out with the aid of a grant from International Development Research Centre, Ottawa, Canada. Information on IDRC is available on the web at http://www.idrc.ca.
Competing interests
The authors completed the Unified Competing Interest form at http://www.icmje.org/coi_disclosure.pdf, and declare no conflicts of interest.
Correspondence to:
Maisam Najafizada, PhD
Assistant Professor, Faculty of Medicine
Memorial University of Newfoundland
300 Prince Philip Drive
Health Sciences Centre, Room 2852
St. John’s, NL, A1B 3V6
Canada
[email protected]