Nodding syndrome (NS) is a neurological condition of unknown aetiology confined to parts of the United Republic of Tanzania (URT), South Sudan and Uganda. The characteristic head nodding that gives the syndrome its name was first recorded as a symptom of epilepsy in the URT in 1965 and retrospective analysis has found evidence for possible cases as early as 1934.1,2 However, it was not until epidemics of NS were later recorded in South Sudan and Uganda in the 1990s and 2000s that NS attracted attention.
NS primarily affects children aged 5 to 15.3 Patients experience progressive neurological, and in some cases endocrinological, dysfunction; case definition criteria are shown in table 1.4 The extent of mortality directly associated with NS remains unclear. Anecdotal evidence has suggested that the greatest risk to NS patients may come from incidental deaths occurring during seizures.4 Seizures are initially atonic although other forms, including myoclonic, absence and generalised tonic-clonic seizures can manifest at later stages of the disease.5
A range of possible aetiologies have been suggested for NS, including associations with diet and nutrition, Onchocera volvulus (OV), Mansonella pestans, measles virus and autoantibodies as well as psychogenic causes.4,6–8 The most recent hypothesis is that NS may represent an autoimmune consequence of molecular mimicry between the autoantigen leiomodin-1 (LM-1) and OV tropomyosin.8 Despite the lack of a definitive aetiology, the term ‘onchocerciasis-associated epilepsy’ (OAE) has emerged in the literature.9 OAE refers to NS alongside other forms of epilepsy with postulated links to OV infection. These include Nakalanga syndrome, documented in Uganda, Burundi and Ethiopia, and other forms of epilepsy, some of which have been documented with head nodding but not confirmed as cases of NS.10,11 There is increasing evidence for OAE, with a recent prospective study demonstrating an association between skin microfilarial density and later risk of seizures or epilepsy.12 With the exception of a syndrome described in Mexico in 1938,13 OAE has thus far only been identified in Africa. No NS cases have been reported beyond the URT, South Sudan or Uganda and no new epidemic cases have been recorded since 2013.14
Without a defined aetiology, therapeutic approaches to NS have been forced to take a symptomatic approach, with guidelines published in 2013.5 A comprehensive programme of pharmacological, physical, speech, language, nutritional and mental health therapy has been shown to improve the condition of NS patients.15
Given recent developments regarding the potential aetiology of NS,8 and a shift towards the phrase OAE in the literature, a systematic review and critique of the proposed aetiologies and therapies of NS and a meta-analysis of the prevalence of OV among NS cases compared with controls is warranted. To maximise the evidence retrieved for non-judgemental appraisal the systematic searches in this review were conducted without restriction on intervention, comparison or study design.
METHODS
Systematic searches were conducted on 21 June 2018 using five electronic databases: EMBASE (1980-2018), Ovid MEDLINE In-Process & Other Non-Indexed Citations and Ovid MEDLINE® (1946-2018), Global Health (1973-2018), Web of Science and BIOSIS Citation Index (1926-2018). The Web of Science Core Collection Citation Indexes searched were: Science Citation Index Expanded (1900-2018), Conference Proceedings Citation Index- Science (1990-2018), Book Citation Index— Science (2005-2018) and the Emerging Sources Citation Index (2015-2018). Each database was searched using the terms ‘nodding syndrome’ OR ‘nodding disease’ OR ‘luc?luc’, without restriction on language, study date or design. For databases that used the Ovid platform (MEDLINE, EMBASE and Global Health) each of these terms were followed by the suffix ‘.ti,ab.’, instigating a search of the title and abstract. The term ‘nodding syndrome’ was also searched as a medical subject heading. For databases accessed through the Web of Science platform, each of the three terms above were searched as topics. Additional manuscripts were identified using manual searching.16–20
Selection of studies
Deduplication was performed using Endnote (version X8.0.1) and Zotero (version 5.0.47). All studies underwent title and abstract screening. Studies were deemed eligible if they were available in English and explicitly addressed NS. Studies which addressed the broader field of OAE and did not explicitly examine NS were excluded. Studies deemed eligible by title and abstract screen were accessed in full-text. Presentation abstracts were deemed to exist as full-text. Thereafter articles not containing primary data regarding the aetiology or treatment of NS were excluded. Studies which could not be accessed in full-text and did not state sufficient information in the abstract were excluded. Studies reporting primary data reported elsewhere were excluded. Both title and abstract and full-text screening were performed independently by two authors (JDJ, HJS), with discrepancies resolved by agreement. To minimise bias, studies eligible for the meta-analysis contained data from which the prevalence of OV in ≥10 NS patients or, if available, ≥10 controls could be calculated. This review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines,21 and a PRISMA checklist completed (Appendix S1 in the Online Supplementary Document). A study protocol was not published prior to this study.
Data extraction and risk of bias
The following information was extracted from each eligible study: author(s), publication date and title, journal name, study location, date, design and case/control population sizes, key findings and prevalence data for meta-analysis if available. The risk of bias was assessed using the appropriate critical appraisal tool from the suite offered by the Joanna Briggs Institute.22 Pre-study randomised controlled trial (RCT) protocols were not subject to critical appraisal.
Statistical analysis
A random-effects meta-analysis was performed to calculate the pooled prevalence (with 95% confidence intervals (Cis)) of OV microfilariae in skin snips taken from NS patients compared to controls. Study heterogeneity was assessed by the I2 statistic, reported with 95% CIs, and interpreted as low (≤25%), moderate (25-75%) and high (≥75%).23 All meta-analyses were conducted using the ‘meta-analysis of proportions’ function on MedCalc version 18.0 (MedCalc Software, Ostend, Belgium) which uses an arcsine square root transformation to calculate the weighted summary proportion.24 The significance of proportions was compared using the MedCalc N-1 χ2 calculator.
RESULTS
Study selection and characteristics
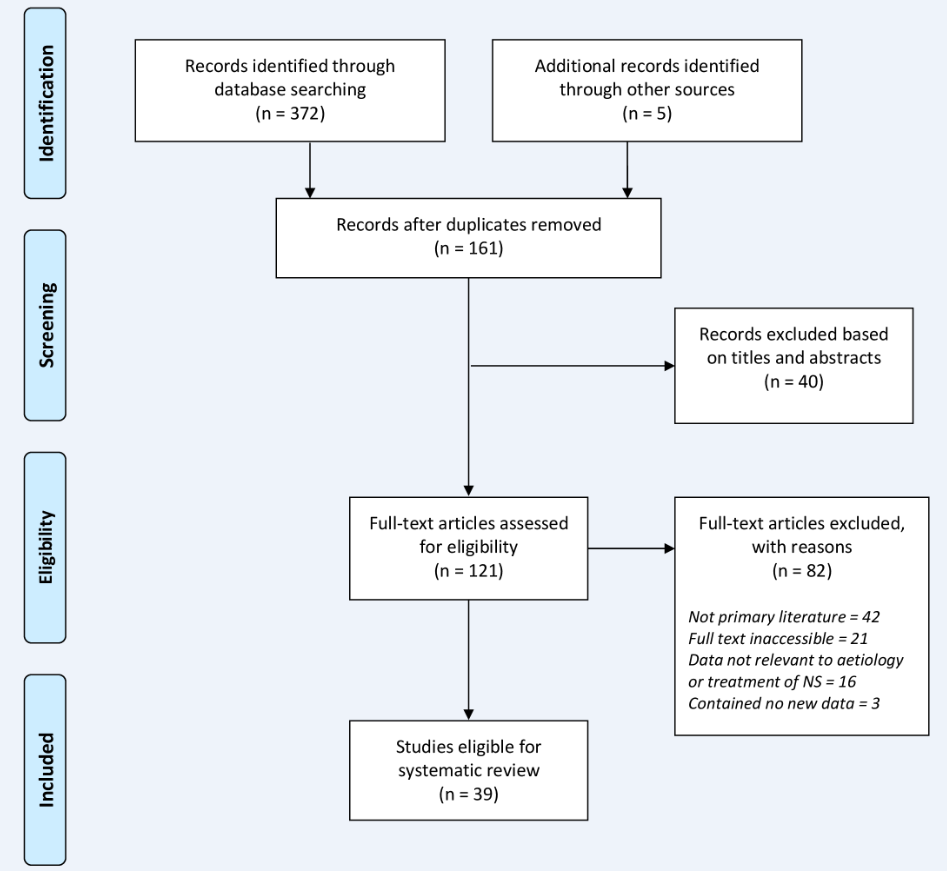
Figure 1 illustrates the study selection process. The systematic search yielded 377 articles; five additional articles were identified from review articles and manual searches.16–20 The titles and abstracts of the 161 articles that remained following deduplication were screened, and a further 40 articles excluded. Of the remaining 121 articles accessed in full-text, 82 were excluded because: they were not primary literature (n=42), the full-text was inaccessible (n=21) or they did not contain relevant (n=16) or new (n=3) data. The final 39 studies included 26 that explored potential aetiologies of NS and 13 that explored treatment of NS. Nine studies contained data suitable for meta-analysis of the prevalence of OV among NS cases and controls. These studies formed the core of the review and were supplemented by wider primary and secondary literature.

The selected articles ranged in date from 2008 to 2018 and included studies from South Sudan (n=4), Uganda (n=22), the URT (n=5), the Democratic Republic of Congo (n=1) and the United States of America (n=1). Study details and key findings are shown in Table 2 and Table 3 for aetiological and therapeutic perspectives respectively. The outcome of critical appraisal of the included studies and the list of studies that were excluded are included in Appendices S2 and S3 in the Online Supplementary Document respectively. Critical appraisal revealed a range of shortcomings in reporting across the eligible studies which, while important to highlight, were not considered to indicate bias sufficient to warrant exclusion.
The aetiology of NS
Appraisal of the data extracted from the 26 articles which investigated theoretical aetiologies of NS7,8,16,17,25–44 revealed four broad aetiological themes which form the basis of this review: metabolic, infectious, autoimmune and psychiatric associations.
Metabolic
Many of the populations where a high incidence of NS was recorded had experienced recent conflict and food shortages and often became reliant on relief food. Aid deliveries were regularly disrupted, sometimes resulting in the delivery of mouldy food, often consumed nonetheless. A correlation was identified between the peaks in NS cases and upsurges in conflict and food shortages, with a temporal disparity of 5-7 years.35 Moreover, it has been reported that there were no cases of NS in Ugandan conflict zones in which people had not been moved into internally displaced persons (IDP) camps, but instead cases appeared after the establishment of the IDP camps, supplied by relief food. This led to the hypothesis that the rise in NS cases may have been linked to the consumption of specific foodstuffs regularly supplied in the IDP camps.16,17,40
Four case-control studies have provided mixed conclusions regarding the association between consumption of (spoiled) relief foods and NS.6,7,36,41 Tumwine and colleagues were the first to suggest an association with food, specifically serena, a type of red/brown sorghum.7 However, further analysis of these data confirmed no association with cassava consumption.40 Later, Spencer and colleagues found positive associations with the consumption of maize, mouldy maize or relief food.41 Obol and colleagues also subsequently identified an association with the consumption of relief food.36 However, it has been suggested that recall bias over approximately eight years, and the attribution of blame by those affected to the Ugandan government and international organisations, may have influenced the results obtained by Spencer and colleagues.45 In contrast, Foltz and colleagues identified an association with the consumption of crushed cassava roots, but did not identify strong associations with the consumption of red sorghum or spoiled relief food.6 Notably, the consumption of certain cyanogenic plants, including sorghum and cassava, on the background of a protein-deficient diet has been linked to outbreaks of neurotoxic disease, albeit apparently not reminiscent of NS.40
It has also been postulated that mycotoxin-driven immunosuppression might have contributed to the NS outbreak, but mycotoxin levels have been shown to be similar between cases and controls28,39 and the distribution and clustering of cases does not appear to reflect an association with meals.46
Aside from the consumption of specific foodstuffs, the disruption of food security, food shortages and associated starvation have also been linked to the aetiology of NS. Several studies have investigated the presence of biomarkers for chronic malnutrition in NS patients. Vitamin B6 deficiency is known to cause abnormal tryptophan metabolism, leading to excessive production of 3-hydroxykynurenine which is known to be neurotoxic.47 Obol and colleagues studied 66 Ugandan cases and found that significantly lower vitamin B6 levels and high levels of 3-hydroxykynurenine were strongly associated with the presence of NS.36 In contrast, Foltz and colleague’s earlier study of 42 Ugandan cases did not identify any significant association between NS and vitamin B6 deficiency.6 Moreover, a Tanzanian case-control study, which compared 22 NS patients to seven controls and one patient with generalised epilepsy, also failed to find an association between NS or epilepsy and vitamin B6 deficiency.27 A large anion gap, indicative of metabolic acidosis, has been observed in 112 NS patients across a case report, case series and case-control study.32–34 However, this likely reflects the patient’s nutritional state, which could explain associations with a history of residence in IDP camps.34 It has also been suggested that this metabolic acidosis may reflect underlying mitochondrial dysfunction32–34; however, analysis of three cases did not detect any aberrations in mitochondrial DNA.48 The serum biotinidase and acetyl carnitine levels of 47 Ugandan NS cases were found to be abnormally low,25 generating speculation that NS may represent the influence of metabolic disruption upon the central nervous system (CNS),16 as has been hypothesised for autism-spectrum disorders.49–51 Vitamin D deficiency has also been noted among NS patients, and could reflect more time spent indoors due to stigmatisation, the use of anticonvulsants or an aspect of the condition itself.37
Psychiatric
Many children had horrific experiences during the conflicts that ravaged parts of Uganda and South Sudan in the 1990s and 2000s, while the URT remained comparatively stable. Psychiatric aetiologies for NS have therefore been considered and a sub-classification of ‘NS psychiatric’ (negative EEG and EMG findings), ‘NS neurological’ (positive electroencephalogram [EEG] and electromyograph [EMG] findings), ‘NS mixed’ and ‘NS atypical’ was proposed.52 However, detailed EEG analysis of two patients has demonstrated that head nodding episodes represent atonic, not ‘pseudo’, seizures.38 Musisi and colleagues found that many NS patients had complex psychiatric morbidities, some with a form of post-traumatic stress disorder known as developmental trauma disorder, and visual hallucinations were also reported.52 A 2013 case series of 22 patients by Idro and colleagues found that 12/22 had psychiatric morbidities including hallucinations (n=6), aggression (n=5) and other behavioural problems (n=4).29 An association between NS and visual hallucinations was also reported in a 2009 case-control study by Foltz and colleagues, but no association was found with the abduction of a family member or auditory hallucinations.6 In contrast, a recent case series involving 48 NS patients found no association between NS and visual hallucinations.25 Unpublished results from a 2016 cross-sectional study of 225 NS patients found that ‘the majority’ began head nodding in the IDP camps and also found that associated psychiatric comorbidities included depression, generalised anxiety disorder, post-traumatic stress disorder and pervasive developmental disorder.42 In a 2018 case series of 32 NS patients that had been resident in IDP camps, parents reported depression (50% of cases), aggression (48.1%), loss of appetite (39%) and anxiety (14.3%); 23.1% of these NS patients reported suicidal thoughts.19
It has been reported that for some patients episodes of head nodding may be spontaneous or triggered by cool temperatures, the offer of food, hyperventilation or sleep.29,38,53 Remarkably, head nodding has been reported to be triggered by the consumption of local, but not imported, foodstuffs.7 The psychological and neurological triggering of head nodding episodes requires greater investigation, and may contribute to the pathophysiological understanding.
Infectious associations
There has been a consistent epidemiological association in the literature between NS and the filarial nematode OV.6,10,30,43,54 An association with another filarial nematode, Mansonella pestans (MP), has also been reported.7 There are two predominant theories regarding the role of filarial infection.
The first is that OV infection indirectly leads to NS via an autoimmune aetiology (see below). Cases of NS have thus far only been identified in areas endemic for OV.55 Temporal, familial and geographical clustering have been observed,56,57 for example limited mapping of NS cases has revealed clustering around watercourses, compared with other forms of epilepsy.30 Regional conflict has also caused disruption of OV elimination programmes, and may have resulted in increased prevalence.56 Moreover, regions in which community-directed treatment with ivermectin and larviciding of major watercourses have been reinstated have experienced a substantial drop in NS cases.58,59
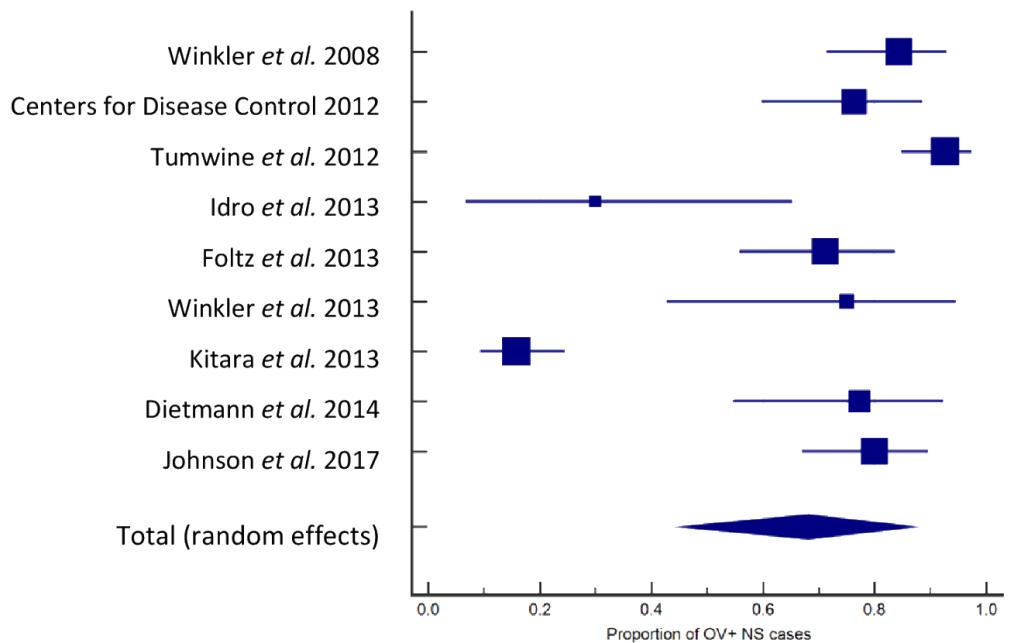
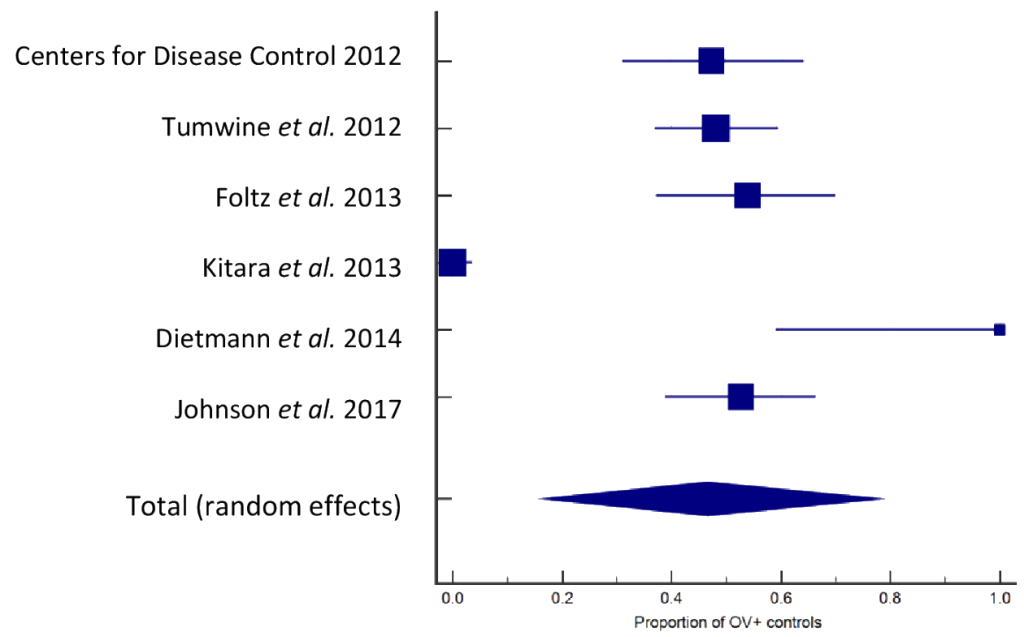
Nine and six studies contained skin snip and/or polymerase chain reaction (PCR) data about the prevalence of OV among NS patients and non-epileptic controls respectively (Table 4). Among these studies there was limited, but conflicting, evidence about the association of ivermectin treatment with the prevalence of NS specifically.7,33 We found that four of the six studies that contained OV prevalence data about both NS patients and controls identified a statistically significant difference between both populations, however many of these studies used small sample sizes. To mitigate against this we performed random-effects meta-analyses to examine the prevalence of OV among NS cases and controls. Among a pooled population of 416 NS patients we found that 68.0% (95% CI=45.2-87.0) were OV+ (Figure 2). Among a pooled population of 321 control subjects 46.6% (95% CI=16.4-78.1) were OV+ (Figure 3). Both results were significant but there was a high level of heterogeneity among both cases (I2=95.5%, 95% CI=93.3-97.0) and controls (I2=97.1%, 95% CI=95 95.5-98.2). The difference of 21.4% in OV prevalence between the pooled populations was significant (P<0.0001).
.png)
.png)
Despite the strong association with the presence of microfilariae in the skin, and magnetic resonance imaging (MRI) evidence of gross neurological lesions in some NS patients, to date evidence of microfilariae in the cerebrospinal fluid (CSF) of NS patients has not been forthcoming.4,6,7,38,40,43 A 2010 survey of CSF from 197 Tanzanians representing healthy, OV+ epileptic, OV+ only or epilepsy only patients did not yield evidence of OV in CSF, nor was skin snip density found to differ between groups.60 However, there is one report from 1976 of microfilariae in the CSF of 5/8 heavily infected onchocerciasis patients without recorded NS or epilepsy.61
The second theory is that OV, and potentially MP, represent opportunistic infections in patients with immunosuppressive neurotropic viral infections, such as MV.41 Conflict-related disruption of immunisation programmes contributed to a large MV epidemic in northern Uganda between 1997 and 2003, with approximately 40 – 50,000 cases per year. There were also simultaneous increases, albeit of lower magnitude, in cases in South Sudan and the URT. It has been observed that the peak in this outbreak preceded the peak in NS cases by 5-6 years.41 This led to the hypothesis that NS may represent a post-infectious sequelae of MV, much like subacute sclerosing panencephalitis (SSPE), reported to occur in 4–27.4 cases per 100,000.62 Clinical similarities between NS and SSPE have been reported, and the two conditions have been compared elsewhere.41 However, NS has not been reported from other countries with past or present outbreaks of MV.
Three case-control studies have investigated the association between MV and NS; two studies from northern Uganda and one from South Sudan.6,7,41 Together these three studies examined 112 cases and 118 controls for the association of a caregiver’s report of previous MV infection and NS. Spencer and colleagues reported a seemingly strong association between previous MV infection and NS, although the 95% CIs were wide (odds ratio (OR)=6.00, 95% CI=1.03-11322). In contrast, Foltz and colleagues found a positive, albeit weaker, association (OR=4.0, 95% CI=1.1-14.2; adjusted odds ratio (AOR)=3.3, 95% CI=0.8-13.66). In a smaller study from South Sudan, Tumwine and colleagues examined 13 cases and 19 controls and found no evidence of an association (OR=0.13, 95% CI=0.02-0.767). A medical history of MV infection is however open to recall bias, Foltz and colleagues used PCR to investigate the presence of MV in the CSF of 16 NS cases, all of which were negative.6
Immunosuppression, linked to mycotoxin exposure and malnutrition, has been suggested to have contributed to the rise in MV cases, and to partly explain the higher prevalence of NS among the Moru compared with the Dinka peoples in South Sudan7,41,63; this disparity has since been disputed.46 Alternatively, it has been hypothesised that different farming practices, the Moru being more reliant on crops and the Dinka on livestock, may have allowed the Dinka to acquire cross-immunity between MV and rinderpest, a related morbillivirus of ruminants.41 Rinderpest has been absent from Africa since 2001, and it has been suggested that loss of cross-immunity could explain the occurrence of NS among the Dinka after that date.41,42
While the neuropathology of NS remains to be fully elucidated, crystalline inclusions have been observed in histological sections from 6/9 patients.30 Given the absence of MRI evidence for crystalline material, it has been suggested that these may represent post-mortem artefacts.64 Characterisation of these postulated inclusion bodies is required, given its reported similarity to NS it is intriguing that the histopathology of SSPE is characterised by the presence of distinct inclusion bodies.65
Autoimmunity
Autoantibodies have been strongly associated with some forms of epilepsy and other neurological disorders.66 Like an infectious aetiology, autoimmunity offers a potential explanation for a range of spatially distributed CNS lesions. Although gross CNS pathology has been observed using imaging studies in some NS patients, evidence of neuroinflammation associated with an autoimmune response has to the best of our knowledge not yet been published.4,29,38,44 Nevertheless, there have been investigations into the presence of autoantibodies in NS patients. Idro and colleagues identified autoantibodies against the voltage-gated potassium channel (VGKC) in 15/31 NS patients compared to 1/11 controls, but there was no evidence of antibodies against the intracellular glutamic acid decarboxylase, associated with complex epilepsy.30 These data contrasted with that of Dietmann and colleagues who failed to identify VGKC or N-methy-D-aspartate receptor autoantibodies27; although the sample storage and assays used in this study have been questioned.30 Meanwhile, Soldatos and colleagues examined the CSF of two of three NS patients and found evidence of partially identical oligoclonal immunoglobulin bands.48
In 2014 it was suggested that autoantibodies against the autoantigen Ieiomodin-1 (anti-LM-1 immunoglobulin [Ig]) may be associated with NS, with anti-LM-1 Ig present in 11/19 Ugandan cases compared to 5/19 local matched controls.31 LM-1 has been reported to be expressed intra- and extra- cellularly in neurons, and is known to be an important component of the actin-myosin complex in myocytes.67,68 The expression of LM-1 in the murine CNS closely matches regions observed to be affected in NS and anti-LM-1 Ig has been shown to be neurotoxic to murine CNS tissue.8 Moreover, anti-LM-1 Ig exhibits cross-reactivity with OV tropomyosin, with which LM-1 shares 25.5% primary sequence identity (37% similarity) and has localised regions of higher sequence homology, e.g. LKEAExRAE is 66.7% identical to amino acids 362 and 372 of LM-1.8 Such cross-reactivity is suggestive of autoimmunity driven by molecular mimicry.
This initial report was followed by a study that investigated the presence of anti-LM-1 Ig in the serum of a further 36 patients from South Sudan. The infection status of the patients was determined by serology (cohort one) or skin snip (cohort two).8,31 Together, anti-LM-1 Ig was present in the serum of 29/55 (52.7%) of the pooled population of NS patients compared with 17/55 unaffected pooled controls (30.8%; P=0.024; matched OR=2.7 (1.1-6.5)). Notably, 24/44 (54.5%) OV+ NS patients were also positive for anti-LM-1 Ig, while 12/29 (41.3%) OV+ controls were also positive for anti-LM-1 lg. The difference in the presence of serum anti-LM-1 Ig between the NS and control cohorts (including OV positive (+) and OV negative (-) patients) was reported as significant (P=0.024). However, we compared the presence of anti-LM-1 Ig between OV+ patients or OV+ controls and found a 13.2% difference that was not significant (P=0.273; 95% CI=-9.81-34.2). CSF samples taken from 16 NS patients were also examined and 50% contained anti-LM-1 Ig, compared to 0/8 North American epilepsy patients.8
Therapeutic approaches to NS
NS shows an almost invariably progressive course, although treatment can improve life expectancy.15 The condition carries a high burden of social stigma for both patients and their families,69,70 including negative stereotypes from healthcare workers.71 Some NS patients have been isolated by communities afraid of contagion.53 Given the typical age and impaired abilities of NS patients, caregivers are vital in facilitating treatment; they seek help from a variety of sources including health facilities (78%), traditional healers (13%) and self-medication (9%). Half of those who attended health facilities did so a month after the onset of symptoms, indicating that more work is needed to ensure prompt help is sought.72 Aside from the work on social stigma there has been little work on the impact of NS on caregivers, although one qualitative study identified a high burden of emotional agony, alongside issues surrounding burnout, safety concerns, stigmatisation and rejection and homicidal ideation.73 Psychological interventions have been shown to mitigate depression in caregivers.74
The 2013 guidelines for the management of NS suggest that, depending on severity, care may include anti-epileptics or anti-convulsants, appropriate management of comorbidities, psychiatric support, nutritional assistance and physical, occupational, speech and language therapy.5 A cross-sectional cohort study of NS and other convulsive epilepsy (OCE) patients treated according to these guidelines showed improvement in both groups of patients, with 25% of NS and 51% of OCE patients being seizure free after 12 months.15
The 2013 guidelines detail the usage, advantages and disadvantages of anti-epileptics for NS.5 However, despite successful reports of the use of anti-epileptics, no clinical trial has been performed. Successful use of sodium valproate has been reported,75 and a case-control study showed a 57% reduction in total seizure burden among 22 NS patients treated with sodium valproate for 2-3 weeks.5 A 1994 case report demonstrated some initial efficacy for phenobarbitone, but long-term control was not achieved.11 A 2013 case series in which four patients were treated with anti-epileptics provided mixed or no evidence for the efficacy of carbamazepine and phenobarbitone respectively.52 In 2014 Winkler and colleagues demonstrated cessation or reduction of head nodding frequency in the majority of patients treated with anti-epileptic drugs.76 However, in 2015 de Polo and colleagues treated 21 patients with carbamazepine as a mono- or combination therapy and found that none obtained good control of any form of seizure associated with NS.77 Benzodiazepines are indicated for icteric patients,5 and given the symptomatic overlap between NS and catatonia, lorazepam has been piloted in NS patients.78 Within one hour of lorazepam administration the severity of catatonia symptoms was reduced in 10/16 patients, and by more than 50% in six.78
Mental health comorbidities have been observed among NS patients, including post-traumatic stress disorder and depression.52 Use of the tricyclic antidepressant imipramine has been recorded for three cases, in which the mood of two improved. However, it was administered as part of a wider treatment programme and the precise contribution of imipramine was unclear.52
Finally, there are treatments aimed at potential aetiologies. Antibiotic elimination of the symbiotic Wolbachia bacteria from the OV nematode has been shown to reduce the inflammation caused by, and contribute to premature death of, the nematode.79,80 An ongoing clinical trial is investigating doxycycline for the treatment of NS, with the aim of elucidating whether Onchocerca or Wolbachia may drive the disease.80,81 There is also an ongoing clinical trial in the Democratic Republic of Congo examining the effect of ivermectin administration in reducing the frequency of OAE, which may have implications for NS patients.82 Three OV- NS patients have been treated with plasmapheresis or intravenous immunoglobulin for presumed autoimmunity, however the results have not been recorded in sufficient detail to appraise treatment efficacy.48
DISCUSSION
Although it is 53 years since NS was first described, the underlying aetiology and pathogenesis remain unclear. This systematic review has collated evidence for metabolic, psychogenic, infectious and autoimmune theories, the limitations of which will now be discussed. Whatever the aetiology, it must explain the age range of patients and disparate nature of clinical findings.29,38,43,44 Notably, probable cases dating from 1934 would call into question hypotheses based solely on modern phenomena.2
The epidemiological history of NS is intriguing: an endemic pattern of cases in the URT and one large epidemic among a broadly malnourished and traumatised Ugandan and South Sudanese population that appears to have a 5-7 year temporal disparity with conflict, food shortages and/or MV epidemics, and no new epidemic cases since 2013. Familial clustering has also been observed, with one case series reporting that 79.6% of NS patients had a family history positive for NS or epilepsy.17,76 Given this apparent familial clustering of NS cases within blackfly exposed locales, genetic and epigenetic genome-wide association studies (GWAS) are warranted and could offer insight into the aetiology of NS and differential susceptibility. The epidemic versus endemic nature of NS is important and calls into question metabolic or psychiatric associations with relief food, IDP camps, conflict and psychological trauma.32,83 Alternatively, NS in the URT may represent a distinct condition.83 It has been suggested that if NS is driven by a specific pathogen, an epidemic could reflect the movement of a non-immune population into an affected area.46 However, if an OV-driven autoimmune aetiology is ultimately described, then regional differences between OV, Wolbachia or the blackfly could explain the differential presence or manifestation of NS. Aside from infectious or immunological theories, observed correlations with biomarkers for malnutrition remain unexplained, although these may be incidental.
The epidemiological association between OV and NS has been questioned.84 OV occurs in 34 countries in Africa, the Middle East, South and Central America, with an estimated 17.7 million people affected.85 In contrast, there have only been several thousand cases of NS in restricted parts of Africa.3 An attempt to resolve this discrepancy has been made by the recent classification of NS under the umbrella term OAE.9 There is substantial evidence in favour of OAE,10 and NS is presumed to represent a point on this proposed clinical spectrum, much of which may remain unappreciated. Meta-analysis of the relationship between OV and epilepsy demonstrated a pooled OR of 2.49 (95% CI=1.61-3.86; P< 0.001), or 1.29 (95% CI=0.93-1.79; P=0.139) when controlled for age, residence and gender86; a significant association was found using studies that reported the presence of OV nodules.86 A recent prospective study from an OV focus in Cameroon has demonstrated a relationship between childhood skin microfilarial density and subsequent risk of epilepsy or seizures.12 Moreover, a fall in the number of cases of NS, as well as cases of epilepsy and Nakalanaga syndrome, appears to correlate with the reestablishment of onchocerciasis control.59 Such correlations could be investigated by further prospective studies. Nevertheless, it is unclear, given the large numbers of OV patients, why NS has not been documented in other OV-endemic regions, although this could reflect greater OV elimination efforts or genotypic differences between populations.51,87,88 Moreover, the interpretation of case-control studies, including those included in the meta-analysis, may be limited by the availability of data about ivermectin therapy given to individuals in such studies. If NS is indeed associated with OV then administration of ivermectin to NS patients may confound observations of this association. It would be ideal if all case-control studies clearly reported ivermectin administration data pertaining to periods before and after the onset of NS, however many studies do not.
The clinical similarities between NS and SSPE have been discussed elsewhere,41 however the association with MV remains unclear. The only significant OR reported had very wide confidence intervals,41 suggesting the study should be repeated with a larger sample size. There is limited correlative evidence suggesting an association between MV and NS epidemics,41 the authors are not aware of reports of NS-like disease in other MV endemic areas, and seizures associated with some cases of MV infection may have led to some patients incorrectly being classified as NS cases.45 Although MV is immunosuppressive,89 it is noted that for immunosuppressed patients to only acquire OV or MP as opportunistic infections is unusual. In contrast, acquired immunodeficiency syndrome patients readily acquire a range of opportunistic infections, including common fungal infections of which there is no recorded association with NS.90 Moreover, it has been suggested that the crystalline inclusions thought to mimic those observed in SSPE represent post-mortem artefacts.64 Histopathological investigations are ongoing, and recent unpublished investigations suggest that NS may be a unique neurodegenerative disorder comparable to a frontotemporal degenerative tauopathy.91
An autoimmune reaction driven by molecular mimicry between OV and human LM-1 was recently proposed.8 However, while Johnson and colleagues demonstrated an association between the presence of anti-LM-1 Ig (subtypes G and M) and NS, whether anti-LM-1 Ig contributes to, is a consequence of or is coincidental with the pathology of NS remains unclear. The naturally occurring presence of autoreactive B cells is well documented.92 While autoantibodies can cause pathology, they can also arise because of cell damage, which may occur secondary to seizures.63 Autoimmune conditions are often associated with inflammatory responses and, at the time of writing, the current lack of evidence for neuroinflammation in NS patients remains intriguing. Moreover, despite expression of LM-1 in myocytes, there are no reports of autoimmune myopathy among NS patients.63 The antibody subtypes identified were IgG and IgM.8 The latter could suggest an ongoing immune response, and subtyping of IgG could offer further insights. The response of NS patients to carefully managed corticosteroids could reveal whether sources of inflammation remain to be identified. The outcome of the treatment of three NS patients with IVIG or plasmapheresis has not yet been made available in detail, but will contribute to the debate.48 The molecular mimicry theory must also explain the presence of NS in OV- patients, although it’s unclear whether or not these were OV naïve patients.8 The presence of OV+ NS patients negative for anti-LM-1 Ig could be explained by detection difficulties or the gradual loss of antibodies following an initiating event, however many autoimmune conditions are chronic and progressive.
Limitations of this review include the exclusion of a small number of studies that were not available in full-text form (Appendix S3, Online Supplementary Document). For their studies to have the greatest impact in the field authors should strive to publish in open-access indexed journals. Moreover, publication of the same data multiple times, encountered several times, does not increase its impact. Assessment of the titles, and where possible abstracts, of these studies suggested that their omission is unlikely to have greatly altered this review. Five potentially relevant studies were not identified by the systematic search strategy. These may have been incorrectly indexed and were included manually to ensure as much relevant data as possible was screened. This approach enhances the transparency and reproducibility of this study, although we cannot exclude the possibility that other non-indexed studies were unknowingly omitted. This study may also be limited by not being pre-registered. Registration of reviews is a non-essential recommendation designed to encourage transparency, improve quality and reduce duplication. Pre-registration of reviews that are never completed is not recommended.93 This study was conceived as a student project, many of which are not published, and the authors therefore decided it was inappropriate to register retrospectively. However, the authors are not aware of any similar studies underway and complied with the PRISMA statement throughout.
A further potential limitation of this study is its focus specifically on NS. While we appreciate that NS may be found to exist as part of a spectrum of OAE, the focus of this study was to review literature pertaining only to NS. A systematic review specifically exploring the link between epilepsy and OV was performed in 2013,86 but as there has been much new work in this area an updated review could be considered. Lastly, it must be remembered that systematic reviews are only ever a snapshot of a dynamic literature and at the time of writing the NS field awaits clear and open reporting of important results, including ongoing trials, post-mortem analyses and immunomodulatory treatment efficacy.38,61,81,94
The aetiology of NS remains unclear with each of the proposed theories still having questions to address. Ongoing trials and further correlative work (e.g. GWAS) may help direct the field towards a conclusive mechanism. It is important to understand the aetiology of NS to care for those affected and to better prevent or treat future epidemics. It is intriguing that no new epidemic cases have been reported since 2013, but this will offer little reassurance until the aetiology and therapy of NS is better understood.
Acknowledgements
The authors wish to thank Dr Medhat Khattar (Division of Infection and Pathway Medicine, University of Edinburgh) for constructive criticism of the manuscript. We wish to thank the two anonymous reviewers of this manuscript for their constructive input.
Ethics approval and consent to participate
Not applicable.
Competing interests
The authors completed the Unified Competing Interest form at http://www.icmje.org/coi_disclosure.pdf, and declare no conflicts of interest.
Funding
None. Access to MedCalc was through a license provided by the Biomedical Teaching Organisation, University of Edinburgh.
Correspondence to:
Dr Joshua D. Jones MA MRes PhD (Cantab)
Division of Infection Medicine
Edinburgh Medical School: Biomedical Sciences
University of Edinburgh
1 George Square
Edinburgh EH8 9JZ
UK
[email protected]