


The sub-Saharan region of Africa accounts for nearly 75% of HIV/AIDS related deaths that have occurred worldwide since the emergence of the disease in the early 1980s. Despite advancements in the control measures and treatment of HIV, this region is still experiencing many challenges including high rates of new infections, AIDS-related deaths and suboptimal disease management strategies.1,2 The United Republic of Tanzania is one of the countries in the region, which by 2012 had 1.5 million people who were living with HIV/AIDS, representing about 6% of all people who are living with HIV/AIDS (PLWHA) in sub-Saharan Africa.3,4 Furthermore, despite excessive use of antiretroviral therapy (ART) in the world, nearly 40,000 AIDS-related deaths have occurred in Tanzania in 2015 alone.5 The prevalence of HIV/AIDS is high in key populations of the country with geographical and demographical variability.
Several surveys have shown substantial deficiencies in key resources required for successful management and coping with the disease among PLWHA. These include lack of nutritional requirements to withstand the effects of ART, poor treatment adherence, lack of sustained social support, stigmatization, relational distress and pregnancy related mortality.6–8
Any success in reducing the prevalence and impact of HIV depends on how a country designs policies in relation to modifiable and non-modifiable drivers of the HIV epidemic. Modifiable drivers include policy interventions such as those related to the control of secondary infections associated with HIV, negative social and cultural norms, HIV testing, status disclosure and elimination of economic and educational disparities. Non-modifiable drivers include demographic characteristics such as age, marital status, and gender. The government of Tanzania has formulated series of policies aimed at confronting HIV/AIDS across the disease trajectory. These policies are implemented based on research and evaluative studies conducted by the National AIDS Control Program (NACP)9 and Tanzania Commission for AIDS (TACAIDS).10 Some of the key policies led to free provision of ART, growth in HIV testing facilities and counselling centers, and establishment of health care clinics in HIV prevalent areas.11
Although the government of Tanzania as well as the donor community had good intentions in designing and implementing policies in different phases of HIV/AIDS disease, evidence shows there is generally little to no significant involvement of PLWHA as key stakeholders in the policy design and implementation processes. It is important to recognise that HIV/AIDS has entered into a chronic condition phase in which PLWHA have the potential to experience prolonged and productive lives. Previous studies have shown the impact of including PLWHA views in developing policies and interventions against HIV stigma12, in understanding and adherence to treatment regimens,13 and on the psycho-social and social factors surrounding the patients.14 This suggests that in the current era of the disease factors such as quality of life, appropriate social support, management of non-AIDS comorbidities and persistent stigmatization need close attention among policy-makers and service provider communities. PLWHA input can be instrumental in designing policies and programs to meet emerging challenges. We have to seek and consider the voice of PLWHA in needs assessment and policy-setting processes through participatory methods that link the needs of the patients, as perceived by the patients, to the policymaking mechanisms. The current HIV policy in Tanzania is geared heavily toward prevention and clinical aspects of the disease,15 and recently on a law against discrimination of PLWHA in the society.16 Despite the good intentions of these strategies, lack of definitive implementation and/or absence of PLWHA voice on their needs are a major shortfall.
The purpose of this study was to use the photovoice technique to assess the social support and healthcare needs of PLWHAs in relation to their daily experiences in coping with the challenges of living with HIV/AIDS.
METHODS
Design and patient recruitment
A qualitative, cross-sectional design using the Photovoice method was conducted to assess the perceptions of PLWHA relative to service needs associated with HIV care. Photovoice is defined as a participatory process through which marginalised people recognise, exhibit, and improve their living and communities using photography. It is a qualitative and exploratory technique with foundations in women’s studies, through which several studies have utilised photographic evidence to effectively study marginalised populations.17–20 Photovoice approach has been applied in policy design and program implementation initiatives in environmental health issues,21 and in the investigation of the social determinants of health among Black mothers living with HIV.22 Photovoice has the ability to present significant accounts crucial in understanding health implications of individuals. It enables patients to tell their own story in a visually effective way that leverages the participatory action research concept in enhancing collaborations between researchers and participants in the investigation without influencing the participants in their views or opinion.23,24 Additionally, photographs are an embodiment of memory that provides path for evaluating individual’s past and present.25 The images present means through which we could narrate and aid the understanding of daily living experiences. Furthermore, photographic images captured by individuals who are marginalised can significantly influence change in the society.26
The Institutional Review Board of Western Kentucky University and WAMATA (a Swahili language acronym for People in the Fight against AIDS in Tanzania) approved this study. All participants consented to participate in the study and have their images collected and published in media relevant to the aims of this study. WAMATA is a non-governmental agency that provides social support and treatment for PLWHA in Dar Es Salaam, Tanzania. Participants were adult clients of WAMATA. A team of investigators held a meeting with WAMATA leadership to explain the purpose of the study. The team procured the necessary permission needed to recruit patients affiliated with WAMATA. Patients who were willing to participate received information about the purpose of the study and voluntarily signed consent forms. PLWHA who participated in the study were adults aged 21 years and older and at the time of the study were regularly involved in WAMATA’s recreational, educational and health promotion programs.
Data collection
Data collection took place over a four-week period between June and July 2014. During that time, two qualified and locally-based interpreters assisted in facilitating communications between the research team and the patients in data collection activities. During the first week, the investigators held introductory meetings with the interpreters and WAMATA leadership to discuss in detail the Photovoice process, objectives of the study, camera operations, ethical, and safety issues. The team held a similar meeting with the participants to ensure that they completely understood the objectives of the study and how they would operate the cameras, save, and deliver the images. Each participant received a camera to take home to collect images that reflected their daily challenges in living with the disease. In the final two weeks of data collection, the investigators asked the patients to return three images that they selected for the purpose of the study. At the point of submitting the images, the participants were asked to complete a structured questionnaire that sought information regarding their photo selections to identify the types of needs they expressed according to their experiences with the disease.
Information was collected according to SHOWED process,17,19 a technique designed to aid participants explain their photos in Photovoice studies. The original tool consisted of a six-question series, including What do you see here? What is really happening here? Why does this concern, situation or strength exist? How does this relate to our lives? How can we be empowered through our new understanding? What can we do? In the current study, these questions were further tailored to capture patients’ experience relating to HIV, and included open-ended questions such as how does this picture relate to your health? Why do you think this picture should be described and shared with regards to your health and service needs? What symptoms were you experiencing when this picture was taken? What inspired you to take this picture? The research team allowed PLWHA to keep the cameras for any future use that would allow them to record, discuss and present their life realities with the disease to other constituencies.27,28
Data analysis
To explore the content and interpretation of the photographs included in the analyses, we employed previously reported Photovoice techniques that included photo-elicitation29 and phototherapy as reported in a study of marginalised women and children.30 The photos and the interview transcripts were examined through a procedure of content analysis and text analysis.31 This method enabled the study to distinguish signifiers inside visual pictures to aid in understanding of the perplexing meanings the participants hold in the settings they were taken. The underlying coding focused on substantive issues related to hindrances to fundamental needs and resources for PLWHA, including social support, disease management and healthcare factors. For this coding process, a prescribed coding outline was drafted from the recorded personal encounters with PLWHA on the field. To efficiently allow for participant experiences to be understood from the images, we performed a review to learn about individual dimensions of empowerment from their own perspectives, specifically in attaching unique meanings of empowerment in each of the selected photographs.32 Lastly, the investigators reviewed entirely the transcripts from the discussions to holistically examine the global nature of the themes being generated—this served as the verification stage for the meanings embedded in the images selected for analysis.33
RESULTS
Participant characteristics
A total of 17 patients participated in the study. They included 16 females and 1 male who completed all phases of the investigation. This sample size is consistent with another study (n=18) that involved PLWHA in a Photovoice analysis.22 The high degree of gender disproportionality among participants is also consistent with the distribution of PLWHA receiving HIV care at WAMATA, and those with disclosed HIV status in the general population.34 The mean age of the patients was 41.4 years (standard deviation (SD)=11.18). Only one of the participants was married at the time of the survey; a majority were single, divorced or widowed. The data showed nearly half of the patients (8; 47%) were engaged in some form of income generating activities such as tailoring or selling vegetables, snacks and bread. The same proportion (47%) were unemployed, while on the basis of religious affiliation, two were Christians while the rest were of the Muslim faith.
The results of content analysis presented here are organised into four major categories related to participant’s perceptions of HIV/AIDS service needs, namely: 1) financial resources: As patients live longer with the disease, new challenges and needs emerge requiring sustainable financial resources; 2) psychological support: As members of the community, PLWHA is a special class of population that presents unique psychological needs related to their disease, 3) cultural competency: Needs related to or influenced by patient’s belief and values or community perceptions of PLWHA; and 4) patient empowerment and engagement: Enabling PLWHA to be in control of their lives through advocacy and active participation in the community. Within each category, themes and resource types were classified according to patients’ overarching connections between disease experience, perceived needs and coping strategies. Emerging subthemes are summarised according to patients’ photographs and responses that best represented their perspectives.
Financial resources
In the category of financial resources, one theme was generated (service accessibility), through which three subthemes of access to medication, access to food and adequate nutrition, and access to appropriate housing were identified. Most participants in the survey were in petty trades, such as selling household goods, tailoring, and cooking. Although all participants had economic constraints, the rationale for engaging in income-generating activities varied among the patients. PLWHA photographs collectively reflected poor living conditions that may have an impact in coping and disease management. For instance, participants identified concerns such as poor living standards, lack of nutritive diet to support their medication and suppress opportunistic infections, all as part of the problems of service accessibility and affordability.
Service accessibility
Access to medication and HIV screening
Over the years since its establishment, WAMATA has been assisting HIV patients in different aspects of care, including HIV testing, provision of counseling and medication, and facilitation of small-scale finance programs. However, being a non-profit private organization with most of its funding dependent on the donor community, the agency has been facing financial constraints to provide adequate levels of medication for opportunistic infections. For example, Patient 1 stated that, “I cannot afford medication for my skin problem.” The participant’s photo and discussion highlighted the importance of having proper access to medication to treat variety forms of opportunistic infections. Another participant, a 43-year old male (Patient 2) with the same sentiments, stated that "there needs to be better access to medications that treat opportunistic infections; the cost of these medications is too high. We need establishments that can offer the medications at a cheap price so people can afford to get them."
Access to nutritious food
A 51-year old female participant living with her five young kids emphasised her nutritional need in this statement, “I will not always get complete meals.” (Patient 3). A large number of participants who were on HIV medications did not have access to regular diet as further explained by Patient 3 (Figure 1), “I do go some days without eating and end up feeling weak most of the times. If I do not eat while taking my HIV medication it feels like I am taking poison. It hurts my stomach very badly. I am very weak if I do not eat and take medicine. I was told not take my medication without food but sometimes I have gone three days without food.”
.png)
Access to appropriate housing
Some of the participants’ perspectives on the financial needs were attributed to structural barriers such as poor allocation and distribution of resources. Most participants in the study have poor housing and living conditions, and these concerns are raised from different perceptions. According to one participant (25 years old single mother living with three kids) in the survey, 'We need more services and support for people like myself who try to raise children while at the same time taking care of my condition,’ (Patient 4). Another female participant, 48 years old (Figure 2), who lost her husband to AIDS expressed concerns about limited capacity in living arrangements, "Our home is too small and crowded so diseases may spread very quickly" (Patient 5).
.png)
Psychological support
For the category of psychological support, one theme was identified, namely stigma-reduction support.
Stigma of HIV/AIDS
There are multiple reasons why people living with HIV are often afraid to disclose their disease status or fail to live independent lives. One of the fundamental concerns expressed by PLWHA was the fear of being abandoned by family and loved ones. Patient 6 (43 years old female) in our study stated that, “I told my boyfriend about my condition and he told me, “this is your problem, not mine” and he disappeared. My relatives were not there for me and did not want me around. Close people to me neglected me. I don’t have a place to live because people won’t help me – even my own family. I move from place to place.” Loss of social support has impacted the patients both psychologically and economically. Eventually, the living standards of HIV infected persons were hampered, adding to their vulnerability with the disease.
Cultural competency
Cultural values are important vehicles that can improve or inhibit the awareness of educational programs on HIV/AIDS in a society. For example, one female participant (Patient 7) a 60-year old female living with three of her children and one grandchild described that their culture exerts prominent impact on PLWHAs’ wellbeing, thus limiting the awareness strategies attributed towards prevention of sexually transmitted diseases (STDs). For instance, participants pointed out that in most cultures in Tanzania, parents and teachers will not openly discuss about STDs with their children and students: "Parents are not comfortable to have practical conversations with the younger generation about sex as they feel it is a personal matter. Even the biology class taught in school did not properly discuss about HIV/AIDS." Another participant, a 61 years old female added, “Our community does not accept people living with HIV/AIDS. It is difficult for providers and others to educate people who have been discriminated against for so long” (Patient 8).
Patient empowerment and engagement
Participants noted that the approach in this study to present images related to their disease had the potential to help in increasing their confidence as well as reinforce their desire to help others. It also encouraged them into becoming educators and peer educators in the society. Participants were deeply motivated to share their thoughts and were committed to create awareness in the society about HIV prevention. According to one participant, ‘I want to show myself out so that others could see I am infected, but I am still a normal person just like them. I live in a community where some people are infected and some are not. I try to help a girl in this picture because she is infected and needs more assistance in her education.’ (Patient 9). Participants believed that images such as those presented here (Figure 3) could be a useful technique in educating the youth about HIV/AIDS, which could be a successful strategy in reducing both HIV transmission and stigma.
.png)
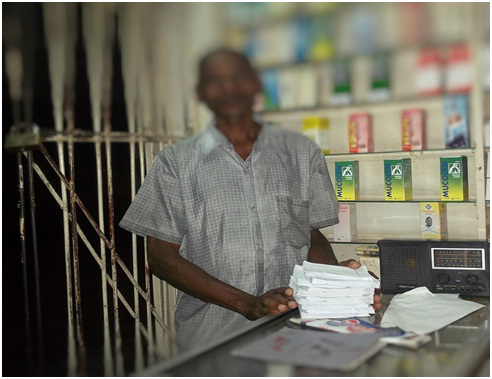
Another participant (Figure 4) stated that, "I want to motivate people to get tested. I tested positive in 2002 and I’m still doing okay today. I want to show people that I can still work even though I am infected, because I take effective medications." (Patient 2).
.png)
Participants noted that the images can increase their ability in reaching out to PLWHA who may be hard to reach due to lack of trust in the health system; that is, the images would help their peers discover they face similar challenges.
Generally, people are initially scared and confused when they learn they have been infected with HIV. However, patients in the study have received health education and medical support from WAMATA, and most have volunteered to educate other people about HIV. Unfortunately, PLWHA continue to face discrimination even when they attempt to make a difference in their communities, as noted by one participant, "I get discriminated against when I try to help or educate other people" (Patient 4). Participants indicated a need to be supported and actively involved/engaged in community outreach activities: “I would like to see more support from our government and not just WAMATA or similar organizations. We need government higher up to come out and talk about HIV, and for PLWHA to talk about their personal experiences with the disease. We need more outreach opportunities to educate the community about HIV/AIDS” (Patient 7).
DISCUSSION
HIV/AIDS is increasingly regarded as a chronic condition in most parts of the world with patients having increasing likelihoods of living longer with the disease upon adopting effective disease management strategies. As PLWHA live longer, they face both new and old challenges associated with the disease, and thus creating an array of needs for their welfare. All patients in the current study participated in a Photovoice research for the first time, and we found that the approach is capable of eliciting courage among PLWHA in a way that could result in increased confidence, self-expression and active participation in matters related on how they cope with the disease. As a result, any resources required to meet the needs of PLWHA would be optimally utilised since the patients themselves would be empowered to encourage program implementation based on their own perspectives of the disease.
Our study found out that poverty was prevalent among study participants and was linked to many other issues faced by PLWHA. Though there was a degree of PLWHA engagement in small businesses, we found that financial challenges and failure in meeting basic necessities for patients and their families were excessive. Previous studies have described poverty as being persistent in PLWHA in most regions of the world.19,35,36 In this way, the images analysed in this study may represent global views of PLWHA as a special population with the need for societal intervention to address disease-specific needs. In particular, poverty presents a significant barrier to educational attainment and developmental opportunities among PLWHA. Consequently, this leads to underemployment, increased exposure to high risk environment, sexual abuse and violence. As a response, key stakeholders should put into place poverty eradication polices targeting PLHWA as a coping mechanism that could give PLWHA, despite their vulnerabilities, a sense of responsibility and aspiration to achieve meaningful goals in life.
Furthermore, in the current study, the importance of access to adequate nutrition was strongly emphasised. PLWHA inability to acquire nutritious food is particularly troubling due to the potential clinical and physical manifestations. On one hand, it is very obvious that availability of ART free of charge to PLWHA is a great societal achievement that has led to the reductions in AIDS-related deaths. On the other hand, however, the use of ART without proper nutrition places the patient at the risk of suffering severe side effects from the drugs. Several studies on nutritional requirements and drug interactions have shown a significant relationship between poor treatment outcomes and lack of adequate nutrition.37,38 Nutrition intervention policies that support food subsidies in the management of HIV should be put in place, especially in low-income resource countries such as Tanzania. It is encouraging to see agencies such as WAMATA providing food assistance to their clients, however, the need is also greater and it requires appropriately formulated policies that bear the voice of PLWHA.
Despite the clinical advancements in preventing AIDS-related deaths, one of the major challenges facing PLWHA is the prevalence AIDS-related comorbidities due to compromised immune systems. Yet, PLWHA have expressed concerns on the lack of adequate accommodation, which presents an additional challenge to PLWHA by increasing the risk of acquiring disease, especially air-borne infections that tend to be easily spread among people in poor living conditions. Education interventions within PLWHA groups and for the community in general is still key for bringing awareness on the negative impact of crowding. At the same time, public health measures such as prevention of malaria and other communicable diseases should be effectively carried out with a clear identification of crowding hotspots in the urban areas.
Our findings were consistent with several studies that reported HIV stigma still being pervasive within the society and in some cases being exhibited by health institutions.39 Stigma presents a negative barrier that affects the lives of PLWHA since it may lead to numerous health consequences such as depression, reduction in intimate relations and discouragement of HIV status disclosure. Frequently, PLWHA are subjected to blame by the society as having acquired the disease at own fault.40 Individual experiences of stigma vary across populations, hence designing of any effective community programs would entail understanding of the impact of stigmatization. For this reason, these programs should be conducted in part by PLWHA as educators and peer educators in the community. We are encouraged by patients in the current study for the willingness expressed to accept such roles. Using PLWHA as community educators should have the immediate impact of empowering the community with the right knowledge offered through the voice of experience. Patient centered programs that empower and engage PLWHA are essential for future HIV programming.
There is no doubt that deep-rooted culture and traditions in the sub-Saharan region of Africa have played a major role in the escalation of HIV/AIDS. These factors still impact PLWHA in many aspects of their lives. Many countries in this region including Tanzania have strong restrictions on sex education among their youth as it is perceived to be a taboo and in most cases immoral.39,41 These beliefs have found their way into the current era of the disease to create barriers in disease management by promoting high-risk sexual behaviors and fueling the persistent stigmatization of HIV/AIDS. Limitations to sex education has created major public health concerns in the history of the disease in sub-Saharan Africa,41,42 and HIV-related stigma has marginalised PLWHA to the extent of creating new health concerns in the community.41 Once again, the involvement of PLWHA in designing and implementation of policies to address these issues could be an effective way of educating the community.39
Governments and non-governmental organizations have great roles to play in promoting the health of PLWHA. This could be executed through several strategies ranging from creating interventions within the PLWHA community, enacting new policies, and facilitating inter-agency collaborations for the provision of care. In our study, we found that though a majority of participants were beneficiaries of the governmental support, they still needed the government to do more, especially with regards to the management of opportunistic infections. The occurrence of these infections, even under the era of free ART in Tanzania, negatively impact the quality of life of PLWHA. The 2008 enactment of HIV and AIDS Act is applauded,16 although it came nearly three decades after the disease was identified in the country and its implementation is still not effective.
Limitations of the study
The findings of this study are limited to the experiences of the participants in a single agency based in one, major commercial city in Tanzania and as such may not be generalizable to the experience of PLWHA across the country. Also, the study included only those PLWHA who were educated on the disease and were open to share their experiences, and as such, did not include experiences of the patients with no such education path. However, from the experience of sub-Saharan Africa region, most of the major cities have been disproportionately affected by HIV/AIDS due to high population density and excessive risks in sexual activity. As a result, a significant proportion of PLWHA still dwells within the cities and suburbs. Thus despite these limitations, our study provides an important framework for understanding the needs of PLWHA in the African context.
CONCLUSIONS
Understanding the experience of PLWHA and inclusion of PLWHA perspectives in designing and implementing interventions for health promotion is an important strategy for success in disease management. Photovoice is a uniquely important process for a qualitative and informative investigation of the needs of PLWHA. Our findings enabled us to understand the barriers these individuals face and how each individual wanted their voice to be heard through the images they produced. We found Photovoice to be an approach that allows for personalised intervention with the capability of promoting empowerment in the target populations through participation, analysis, understanding, and describing challenges, ultimately leading to the right solutions even in problems with global impact such as HIV and AIDS.
Acknowledgements
Grateful acknowledgment is made to WAMATA, Tanzania, for their permission to use the agency to generate information needed for this study.
Funding
This research was supported by Western Kentucky University under FUSE Grant, Award #15-SP279.
Competing interests
The authors have completed the Unified Competing Interest form at http://www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author) and declare no conflict of interest.
Correspondence to:
Dr William N Mkanta
Department of Public Health
Western Kentucky University
1906 College Heights Blvd. #11082
Bowling Green, KY 42101
United States of America
[email protected]