
Reducing maternal mortality remains a global priority, as 2020 estimates showed stagnated progress in 2016-2020.1 The global maternal mortality ratio (MMR) was estimated at 223 per 100,000 livebirths in 2020, while sub-Saharan Africa (SSA) had a ratio of 545/100,000 livebirths.1 Inequities in progress exist across countries, and context-specific information is necessary to enable appropriate responses to drivers of mortality and morbidity. In the absence of well-established civil registration systems that provide more reliable data for mortality estimates, population-based household surveys and routine health facility data are commonly used in low-resource settings.2,3 While population surveys are more representative, they are infrequently used to monitor rare events like maternal mortality closely and are not often powered to provide sub-national estimates that could expose inequities in progress.2 Routine facility data provide more frequent and granular data; however, they omit events occurring in communities and may be inconsistent.2,4 Nonetheless, over 60% of women in SSA give birth in health facilities,5 more so in urban areas than rural areas.6 In such settings, exploration of trends in institutional MMR (IMMR) can therefore provide useful insights for mortality reduction efforts and health systems improvement.
Direct obstetric conditions such as postpartum haemorrhage and pre-eclampsia/eclampsia are major causes of maternal deaths in urban-based facilities.7–10 Indirect non-obstetric complications such as malaria and anaemia have also been reported.10 Facility-based maternal deaths are associated with other factors such as maternal age, poor referral, lack of supplies/equipment and infrastructural issues,11,12 as well as system fragmentation and system shocks.13 While these factors may not differ from rural settings, trends in maternal mortality in urban settings in Africa are of interest given the several challenges linked to the ongoing rapid urbanisation.14 Urban areas offer increased availability of health services, including emergency obstetric care (EmOC).15 However, inequality and low socio-economic status of many urban residents increasingly result in limited access to and options for affordable, high-quality care.14,16 Additional barriers are created by the complex mix of healthcare providers within poorly defined and coordinated system structures.17,18 Wong et al. reported variation in the utilisation of maternal health services across cities in SSA.19 IMMR varies in hospitals situated in many African cities7,8,10 and perinatal mortality rate has been reported to be higher in urban areas compared to rural areas.20
Towards accelerating maternal mortality reduction, Uganda launched the investment case for Reproductive, Maternal, Newborn, Child, and Adolescent Health (RMNCAH) Sharpened Plan in 2016.21 High-burden regions in the country and strengthening interventions such as maternal and perinatal death surveillance and response (MPDSR) were prioritised. According to the 2022 Demographic and Health Survey estimates, Uganda’s MMR stood at 189/100,000 live births, showing a 44% decline from 336 in 2016.21–23 While health sector reports show a decline in the national IMMR between 2016 and 2021, there is uneven progress with pockets of high numbers of reported maternal deaths, such as in the capital city, Kampala.24,25 Studies have examined the causes of maternal mortality and related factors in Kampala.9,26–28 However, there has been limited exploration of the progress made in this city since the start of the Sustainable Development Goals in 2016. There is a growing need for evidence on urban health in Africa,29 and knowledge of mortality levels and trends is an important step toward designing high-quality urban health systems. The objective of this study is to describe the trend in IMMR in Kampala for the six-year period 2016-2021, as well as the causes of deaths and related factors, and use these to discuss possible explanations for the observed trends.
METHODS
Study design
We conducted a retrospective study and analysed routine health facility data from 1st January 2016 to 31st December 2021. We estimated the annual IMMR and described the trend over six years. We reviewed medical records for maternal deaths that occurred within the same period at three hospitals to identify possible explanations for the IMMR trend.
Study setting
Kampala is Uganda’s capital city, with an estimated population of 1.7 million residents and an annual population growth rate of 4.0%.30 Residents of neighbouring districts such as Wakiso and Mukono rely on Kampala for economic activities and health services, with Kampala’s day-time population being about 3.5 million people.31 Healthcare in Kampala is provided by public (government-owned), private-not-for-profit (PNFP) and private-for-profit (PFP) health facilities. Public facilities are organised in a hierarchical structure whereby the National and Regional Referral Hospitals are semi-autonomous and report to the Ministry of Health (MoH), while health centre (HC) IVs, HC IIIs and HC IIs, which are primary healthcare levels, are managed by Kampala Capital City Authority (KCCA). PNFP facilities are governed by respective medical bureaus such as the Uganda Catholic Medical Bureau. Over 90% of births in Kampala occur in health facilities19,23 and public facilities account for over 60% of all deliveries.
Kampala has benefitted from several initiatives to improve maternal and perinatal outcomes. For example, the renovation of Mulago National Referral Hospital in 2014 improved infrastructure as the Department of Obstetrics and Gynaecology was expanded to Kawempe National Referral Hospital in 2016. Other initiatives include the Kampala Maternal Newborn Slum project (2019-2021), which, among other contributions, improved referral care coordination by establishing an emergency call and ambulance dispatch centre.32 Also, the Maternal Child Health and Nutrition Activity (2019-2023) supports the implementation of strategies such as MPDSR and has contributed to improved notification and reporting of maternal deaths.25 Additional initiatives such as weekly MPDSR meetings at the city level, local maternity and newborn systems, quality improvement mentorships, and the establishment of the national safe motherhood committee and sub-committees were initiated recently. These initiatives were accompanied by notable political support at MoH, local government (KCCA), and health development partners, with more platforms for improving accountability in maternal health service provision.
Study sample
We used aggregate data relevant for maternal mortality estimation which are routinely reported by health facilities into the district health information system (DHIS2) between 2016 and 2021 (1,487 health facilities in 2016-2019 and 1,760 in 2020-2021). Our analysis included all facilities which provided childbirth services in 2016-2021, defined as those that reported at least one delivery in DHIS2 in any of the six years (255 facilities in 2016-2019 and 247 in 2020-2021). Facility characteristics are provided in Table S1 in the Online Supplementary Document.
The medical records review was conducted at three hospitals purposively selected to represent the three sectors involved in childbirth service provision and different delivery volumes and mortality profiles (Table 1). The three hospitals reported at least one maternal death between 2016 and 2021. Hospitals provide comprehensive EmOC (CEmOC), including caesarean section, blood transfusion, administration of parenteral uterotonics, anticonvulsants, antibiotics, and manual placenta removal, among others.33
Data sources and collection
Routine health facility data: Various maternal health-related data elements, including the number of deliveries, live births and maternal deaths, are expected to be reported by health facilities monthly through DHIS2. In January/February 2022, we extracted annual and monthly aggregate data reported for deliveries, live births, and maternal deaths into Microsoft Excel sheets for January 2016 to December 2021 from the DHIS2. Before analysis, a standard desk review of the quality of the data on deliveries, live births and maternal deaths was conducted, in which reporting completeness, outliers and consistency over time were examined. Overall completeness of data on deliveries and livebirths was at least 50%, with HC IIs or clinics accounting for most zero values, which in Uganda’s service delivery context, do not routinely conduct deliveries and, therefore, are likely to report (true) zero values. The percentage of monthly outlier values was less than 2%. Inconsistency in reporting overtime was notable for maternal deaths.
Maternal death records: We reviewed medical records covering the six-year period of interest between May and June 2022. Data were abstracted to a pre-developed form based on the Uganda maternal death review form34 into KoboToolbox (Kobo, Cambridge, Massachusetts, US). The form captured the woman’s age, residence, admission history, obstetric history, antenatal care attendance, delivery information, cause of death and health system contributing factors. Cases of maternal deaths were first identified by reviewing facility maternity registers, records books (maternity, obstetric and labour wards) and the records offices. A list of inpatient numbers was generated and used to guide the retrieval of files by records officers in each facility. The records reviewed included case files, death notifications and review forms. Reviewed records were based on the definition of maternal death by the World Health Organization (WHO), which is also reflected in Uganda’s guidelines: “a woman who died while pregnant or within 42 days of termination of the pregnancy, irrespective of the duration and site of pregnancy, from any cause related to or aggravated by the pregnancy or its management, excluding accidental or incidental causes”.34,35 We extracted causes of death and health system related factors as documented in the records. Variables extracted from the records are defined in (Table 2). Five research assistants who were trained on the use of tools, including a review of the facility registers and reporting forms and ethical issues related to handling and extracting data from medical records collected the data with supervision by the lead author.
Data analysis
We cleaned and analysed data using Stata 14 (Stata Corporation, College Station, Texas, US) and plotted graphs with Microsoft Excel (Microsoft Corporation, Redmond, Washington, US). To calculate IMMR using DHIS2 data, we used annual aggregate numbers for deliveries, livebirths and maternal deaths based on existing literature.34,35,37 IMMR was computed as the total number of maternal deaths per 100,000 deliveries reported in the same year and for the six-year period. Previous studies have expressed IMMR per 100,000 livebirths.7,11 Thus, we computed the IMMR per 100,000 livebirths within the same review period for comparability. A non-parametric test for trend (np trends, jterpstra) was done in Stata using a 5% level of significance, comparing 2016 to 2019 and 2019 to 2021. We examined the IMMR trend by facility ownership and presented the results using three two-year periods due to the small number of maternal deaths in PFP facilities, causing high levels of variability in annual trends.
Causes of maternal deaths and other characteristics of women who died were summarised using frequencies and percentages, presented in tables and graphs. We computed frequencies and percentages of the characteristics for the six years (2016-2021), and if a year had <100 observations, we collapsed them into time periods. Causes of maternal death were considered as the conditions that initiated the chain of events leading to maternal death based on the WHO definition,35 and our analysis focused on direct obstetric causes. Antepartum and postpartum haemorrhage were combined to estimate the percentage of deaths attributed to obstetric haemorrhage. In cases where the documentation indicated the woman to have more than one cause of death, e.g., pre-eclampsia and pregnancy-related infection, each cause was counted individually. Thus, the percentages reflect the number of cases which were impacted by a given cause. Conditions such as ruptured uterus and obstructed labour were considered individually only when the record did not explicitly specify any other condition in which they are commonly implicated in the chain of events surrounding maternal death. These conditions were grouped as other obstetric causes. We noted the non-obstetric/indirect causes, and cases in which the cause of death was not known, not determined or not explicitly specified were excluded from the analysis.
RESULTS
Levels and trends in institutional maternal mortality in Kampala, 2016 to 2021
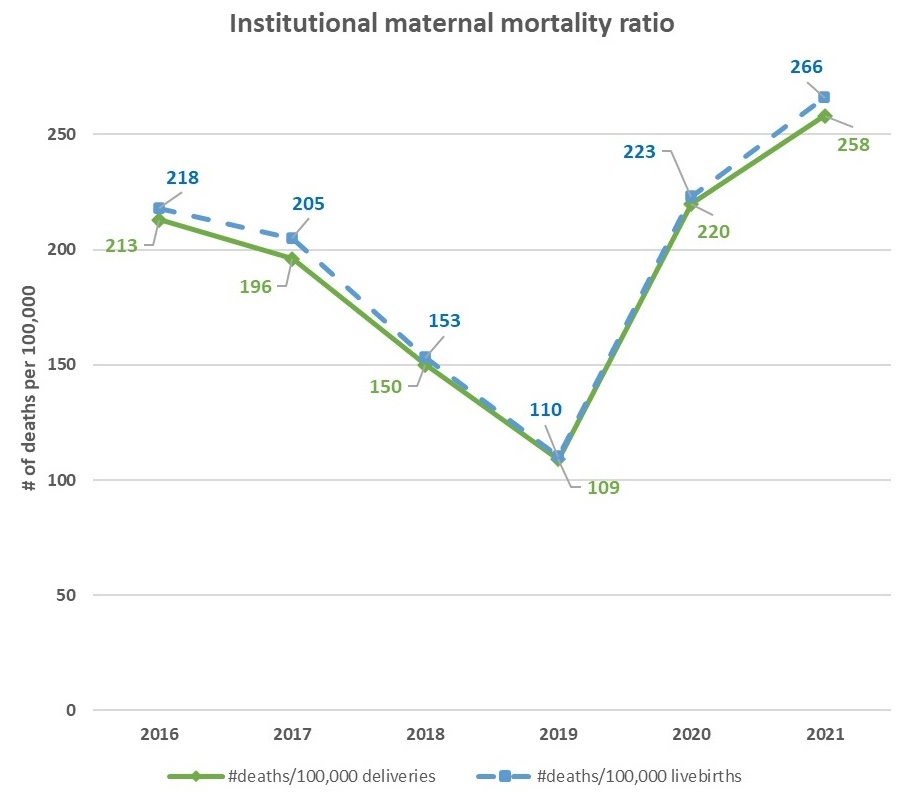
The total number of institutional maternal deaths reported between 2016 and 2021 was 992, ranging from 97 in 2019 to 214 in 2021. The annual number of institutional deliveries reported ranged from 79,876 in 2016 to 95,204 in 2017, and the total for the six years was 524,185. The overall six-year IMMR was 189/100,000 deliveries (194/100,000 live births). Figure 1 displays the annual levels of IMMR, showing a gradual and significant decline between 2016 and 2019 (from 213 to 109/100,000 deliveries, p=0.042). This was followed by an increase to 220/100,000 deliveries in 2020 and 258 in 2021 (p=0.117 between 2019 and 2021). Details of the number of maternal deaths, deliveries and livebirths reported each year and IMMR with a denominator of livebirths are shown in Table S2 in the Online Supplementary Document.

Levels and trends in institutional maternal mortality by facility ownership
Figure 2 shows variation in IMMR across three categories of facility ownership. IMMR was higher in public than PNFP or PFP facilities, except for 2016/17. A steady decline in IMMR was observed in PNFP, while IMMR varied considerably in public and PFP facilities. IMMR was highest in 2020-2021 at 313/100,000 deliveries in public facilities and lowest in 2018/19 at 155. In PFP facilities, IMMR was highest in 2016/17 across the three groups of facilities at 291/100,000 deliveries, and decreased by nine-fold to 32 in 2018/19, then increased to 78 in 2020/21. Figure S1 in the Online Supplementary Document shows the individual year trends in IMMR.

Description of maternal deaths from three hospitals in Kampala between 2016 and 2021
We reviewed 358 maternal death cases across the six years. The average age of women who died was 28(±6) years, ranging from 14 to 46 years. Nearly 50% of women whose records were reviewed lived in Wakiso district outside of Kampala city (Table 3). Approximately 45% of women had a parity of 2-4 on admission. More than 50% of women whose records were reviewed were referred from other health facilities, with at least 30% being referred from hospitals. Stillbirths were documented in 33% of the women who died.
Causes of maternal deaths documented in the medical records
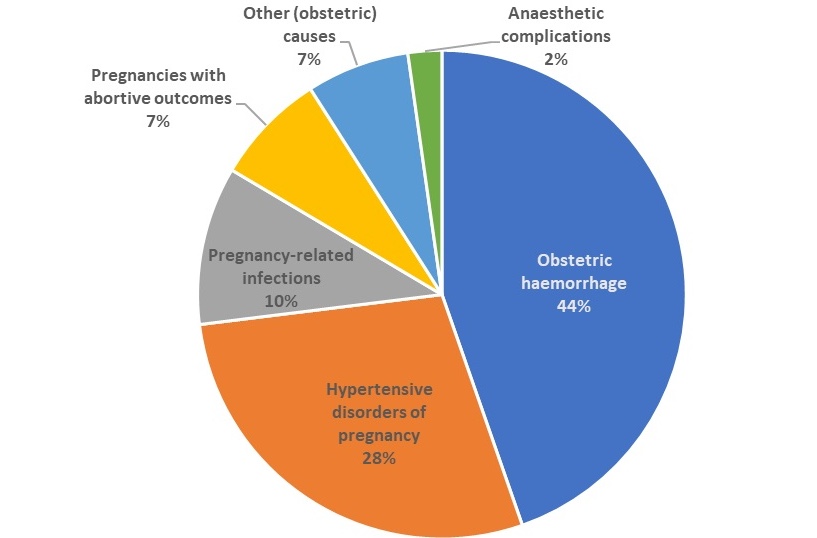
Of the 358 maternal death records reviewed, 44% (n=157) were due to obstetric haemorrhage, with postpartum haemorrhage accounting for 37% (n=134); 28% (n=100) were due to hypertensive disorders of pregnancy (HDP), and 10% (n=37) were attributed to pregnancy-related infections (Figure 3). Approximately 31% of reviewed deaths were complicated by anaemia, while infections not related to pregnancy (Malaria, Human Immuno-deficiency Virus, Corona Virus Disease) alone were documented in 5% of the files reviewed.

Documented system-related factors contributing to maternal deaths
Among the 358 women whose medical records were reviewed, system-related factors were documented in 65% (n=231), with 32% (n=116) being affected by resource-, 28% (n=101) by staff-, and 40% (n=142) by process-related factors. In 6% (22/358) of cases, all three groups of system factors were documented; 13% (45/358) had staff and resource factors; 15% (52/358) had process and staff factors, while 15% (53/358) had process and resource factors. Among deaths attributed to obstetric haemorrhage, system-related factors were implicated in 72% (n=113) of the cases, with resource- and process-related factors accounting for the highest (>40%) percentage (Table 4). System-related factors were reported in 59% of deaths attributed to HDP, with process factors accounting for the highest percentage (43%).
DISCUSSION
Summary of key findings
This study examined levels and trends in IMMR in Kampala city during 2016-2021 using data reported by health facilities through DHIS2. The overall IMMR was 189/100,000 deliveries (194/100,000 live births) and was higher in public facilities than in private facilities. We found a decline in IMMR from 2016 to 2019, followed by a marked increase in 2020 and 2021. Over the six-year period, most maternal deaths were attributed to obstetric haemorrhage and HDP and were among women referred from other health facilities and women who lived in Wakiso district. Health system-related factors were documented in more than half, and stillbirths in about one-third of the reviewed deaths.
Interpretation of findings
IMMR estimates in our study were higher than national IMMR levels within the same period. In 2016, Kampala’s IMMR was 213/100,000 deliveries compared with the national IMMR of <150/100,000 deliveries in 2015/16 or 2016/17; while in 2021, the IMMR in Kampala was 258 compared to the national IMMR of ≤100 in 2019/20 and 2020/21.24,25 The high IMMR in Kampala is unsurprising, given the presence of the national referral hospital (NRH), which cares for complex obstetric cases with a higher risk of poor outcomes. Nonetheless, health system constraints, population dynamics, and the unpredictable demand for EmOC could explain the high mortality levels. Our IMMR estimate is lower than what was found previously in a major hospital in Northern Uganda,38 potentially due to underreporting of maternal deaths in Kampala in 2016-2019. Compared with studies from other urban facilities in Africa, our IMMR estimate is higher than in a tertiary hospital in Minia, Egypt,39 but lower than in hospitals in Jimma, Ethiopia8 and Abuja, Nigeria.7 Our measurement using data from all facilities providing childbirth services within the urban boundary of Kampala and reported in DHIS2 might be more representative, but differences could also be due to variations in review periods and reporting requirements.
We found that an increase followed an initial decline in IMMR. The downward trend in 2016-2019 could be a true decline in mortality due to the implementation of the Sharpened plan for RMNCAH,40 or a result of data inconsistencies arising from failure to capture and report maternal deaths adequately. This might have occurred during the transition of the NRH for obstetrics and gynaecology (2016-2018), which could have created discrepancies in the number of maternal deaths reported. The NRH reports most of the maternal deaths in Kampala and during the transition period, it is likely that some maternal deaths were not captured in the DHIS2. On the other hand, the increase in IMMR after 2019 could be attributed to intensified efforts by the government to improve accountability for maternal deaths within facilities in Kampala, which contributed to improvement in surveillance and reporting of maternal deaths, coordination, and utilisation of emergency obstetric care.32 The rise may also reflect a true increase in the number of facility deaths secondary to health system shortages and indirectly influenced by the initial waves of the 2019 Coronavirus Disease pandemic through its effects on the quality of and accessibility to care.41,42 This observation relates to what was revealed in a systematic review on effects of COVID 19 showing an increase in global maternal deaths.43
An important observation in our study was the variability in IMMR in PFP facilities and the steep increase in public facilities in 2020-2021, which accounted for the overall IMMR trend observed. The high IMMR in public facilities may be attributed to inadequate readiness secondary to limited infrastructure and overwhelming client volumes, which include the majority resident population of low socio-economic status and most obstetric referrals. Moreover, public facilities are better regulated and are more likely to report most (if not all) maternal deaths. On the other hand, PFP facilities comprise mostly facilities with limited capacity to provide obstetric care and conduct fewer (about 16% of all deliveries in Kampala) and less complicated deliveries.44 This may explain the lower number of deaths reported by PFP health facilities, in addition to referrals, especially from the lower-level PFP health facilities. Furthermore, the numerous lower-level PFP facilities are inadequately regulated, and this may contribute to poor/variable reporting of maternal deaths. However, low mortality in PFP facilities could also be attributed to the readiness of private hospitals.
Maternal mortality in Kampala’s health facilities seems to be largely preventable, consistent with studies from other African urban settings.7,9,45 Health system factors in our study, in particular, indicate that disconnections in care provision, whether within one facility (e.g., inappropriate interventions, delay in care, lack of blood products, etc.) or across facilities (e.g., during referral with poor documentation) may be at the root of the problem. In all, 60% of institutional maternal deaths in Kampala were referred from other facilities, suggesting inadequate readiness, poor linkages and continuity of care among CEmOC facilities in and outside Kampala. This may explain why referrals from hospitals, which are designated CEmOC facilities and should have provided the required care, accounted for 30% of maternal deaths in Kampala.27 Furthermore, 40% of deaths in Kampala were among women who lived in Wakiso district. This may be a result of women searching for better care, proximity of facilities in Kampala to women living in Wakiso or failures in the referral system. Poor maternal outcomes among women from city suburbs have been reported.46 Additionally, three in ten of the maternal deaths were accompanied by a stillbirth, which may also have been preventable based on reported contributing factors such as maternal HDP.47 Nonetheless, accessibility issues resulting from socio-economic vulnerability and lack of knowledge of when and where to seek care might exist in Kampala.48
Implications for policy and practice
Our study suggests that data and reporting quality in public and PFP facilities influenced IMMR in Kampala over time. Intensifying efforts to harmonise and improve data quality across the provider mix in urban areas could increase estimates’ reliability and utility in decision-making for urban health improvement. This may further require robust and consistent data capture systems that can adapt to changes in healthcare infrastructure and other service delivery arrangements that affect data sources. Referrals were a major source of maternal deaths in Kampala, implying that substantial improvement in referral processes at different levels in and around the city (with special attention to suburbs) could contribute to maternal mortality reduction. This should be accompanied by capacity strengthening and effective linkages among CEmOC facilities. The concentration of facility deliveries and, inevitably, maternal deaths in public facilities points to the limited availability of affordable quality care in Kampala for most women and underscores the need to expand public health infrastructure. Avenues to facilitate the provision of quality and affordable care in PFP facilities could provide additional benefits. Additionally, intentional maternal and perinatal death surveillance and response with improved governance, where policy makers provide stewardship and are involved in generating solutions to problems contributing to maternal deaths, have potential in improving maternal health outcomes in urban areas. However, a structured evaluation is needed to better understand which specific changes affected IMMR and how, and how strategies which effectively reduce maternal mortality in urban areas can be scaled up.
Suggestions for future research
Further studies should explore explanations for changes in maternal mortality levels using systematic approaches to ascertain the relative contribution of known and nuanced factors underlying mortality changes in urban settings, as well as the various innovations being implemented to improve maternal survival. Such specificity would provide a more robust rationale for targeting efforts and allocating resources to accelerate mortality reduction and contribute to better urban health planning. Relatedly, future research should examine existing data inconsistencies in the reporting of maternal deaths to provide a better picture of the patterns in mortality levels. The findings of this study highlighted important distribution patterns of maternal mortality within health facilities, and to further inform the design of responsive services in urban spaces in Africa, there is a need to understand how women reach appropriate obstetric care, especially those who develop obstetric complications. This would help identify critical steps for further action in improving maternal survival. Monitoring progress using health facility data is an important component of health systems in Africa, but city-level comparison is currently complicated by inconsistencies in data sources and uncertainties around the landscape of obstetric care provision across different cities. Studies that shed light on how IMMR can uniformly be assessed in SSA countries and its potential linkage to MMR, especially in contexts with high facility-based deliveries, will provide useful advances for addressing maternal health in urban settings.
Strengths and limitations
We used data from all facilities that reported having childbirth services, which provides an informative and representative picture of facility-based maternal mortality in Kampala City and highlights useful insights for improving maternal survival. Nonetheless, the study has some limitations. First, we used routine health facility data to assess IMMR, which may have given lower or higher than expected levels due to reporting inconsistencies or outliers, especially for maternal deaths for which corrections or adjustments were not made during analysis. Secondly, while the study targeted all cases of maternal deaths which occurred between 1st January 2016 and 31st December 2021 from the three selected hospitals, records, especially from 2016 to 2019, were fewer compared to 2020-2021. As such, we could have missed out on some characteristics related to institutional maternal deaths in Kampala. However, one recent study conducted in one of our study sites where records review was done showed similar characteristics of deaths between 2016 and 2018.9
CONCLUSIONS
IMMR in Kampala increased in 2019-2021. Health infrastructure changes and maternal health initiatives potentially accounted for the observed trend by affecting data quality. Maternal deaths were mostly attributed to obstetric haemorrhage and hypertensive disorders, while referral and facility readiness were underlying reasons for institutional maternal deaths in Kampala. Addressing bottlenecks in current referral processes within Kampala and surrounding districts will be instrumental in maternal mortality reduction efforts. Further research should determine the relative contribution of key influences on mortality levels and examine the dynamics between women’s care-seeking pathways and service delivery arrangements for emergency obstetric care in urban settings.
Acknowledgements
We thank Dr Aloysius Ssenyonjo and Dr Dinah Amongin for reviewing and providing feedback on the manuscript.
Ethics statement
Ethical approval was obtained from the ethics committees of Makerere University School of Public Health (SPH-2021-169), the Uganda National Council for Science and Technology (HS1952ES), the Institute of Tropical Medicine Antwerp (1529/21) and the University of Antwerp Hospital (2021-1743). Consent to participate in this study was not applicable. All methods were implemented in accordance with relevant guidelines and regulations.
Funding
CB was funded by the Belgian Directorate for Development Co-operation PhD sandwich programme.
Authorship contributions
CB conceptualised the study, analysed the data and produced initial drafts of the paper. ABT, JVO, LB and PW reviewed the design and provided overall study supervision. LB, AS and RMK participated in the analysis. All authors reviewed and edited the initial drafts and approved the final version that was submitted.
Disclosure of interest
Authors completed the ICMJE Disclosure of Interest Form (available upon request from the corresponding author) and disclosed no relevant interests.
Additional material
Included as Online Supplementary Document.
Correspondence to:
Catherine Birabwa
Makerere University School of Public Health
7072, Kampala
Uganda
[email protected]